
Abstract
Objective:
To investigate the safety and feasibility of single-port-plus-one (SP + 1) thoracoscopic lobectomy in the treatment of congenital pulmonary airway malformation (CPAM) in infants.
Methods:
The clinical data of 35 infants who underwent SP + 1 thoracoscopic lobectomy from May 2017 to December 2023 were retrospectively analyzed. The median age was 7 months, and the median weight was 8 kg. Included: 4 cases of upper lobectomy, 3 cases of middle lobectomy, and 28 cases of lower lobectomy.
Results:
SP + 1 thoracoscopic lobectomy was successfully completed in all infants. One case developed a postoperative air leak. There were no deaths and no other postoperative complications such as pulmonary infection, bleeding, atelectasis, bronchopleural fistula, and chylothorax.
Conclusion:
SP + 1 thoracoscopic lobectomy for infants with CPAM is safe, feasible, and cosmetic with satisfactory perioperative results in our preliminary experience.
Introduction
Congenital pulmonary airway malformation (CPAM) is the prevalent form of congenital lung malformation. It is identified by a histological profile characterized by extreme proliferation and expansion of terminal bronchioles leading to the loss of normal alveoli. 1 The majority of CPAM can be detectable during antenatal screening. While most infants with CPAM are asymptomatic, there is a risk of recurrent infection and malignant transformation. Therefore, lobectomy is the recommended treatment. 2 In the pursuit of reducing trauma, minimizing postoperative pain and complications, and accelerating postoperative recovery, thoracoscopic lobectomy has gained popularity worldwide. Based on traditional three-port thoracoscopic lobectomy, we propose single-port-plus-one (SP + 1) thoracoscopic lobectomy to further minimize chest wall trauma and enhance aesthetic outcomes. The following report presents our findings:
Materials and Methods
Patients
From May 2017 to December 2023, 35 infants with CPAM were admitted to the Pediatric Surgery Department of the Second Hospital of Hebei Medical University. The age ranged from 2 months to 2 years, with a median age of 7 months. The weight ranged from 4.3 kg to 14 kg, with a median of 8 kg. All infants underwent chest enhancement and high-resolution thin-layer computerized tomography (CT) scanning prior to surgery in order to locate and determine the extent of the lesion. The diagnosis of CPAM was confirmed through pathology reports. The lesions were found in the upper lobe in 4 cases, the middle lobe in 3 cases, and the lower lobe in 28 cases. The exclusion criteria were as follows: (1) patients with lesions in multiple lobes; (2) patients experiencing severe complications and are unable to tolerate one-lung ventilation or artificial pneumothorax; (3) patients without complete perioperative clinical data.
The study was approved by the Institutional Review Board of Second Hospital of Hebei Medical University, and written informed consent was obtained from legal guardians.
Operative method
Single-lumen and bronchial blockers were utilized for one-lung ventilation according to the patient’s needs. Following sufficient anesthesia, the patient was positioned in lateral decubitus. An axillary roll is positioned under the uniport site to widen the intercostal space maximally at this level. The surgeon and assistant stand at the front of the patient. A TRIPORT is inserted through a 1.5 cm incision made in the front axillary line of the fifth intercostal space. Subsequently, CO2 was infused into the chest cavity at a pressure of roughly 5 mmHg to establish an optimal operational area. A 5 mm thoracoscope is inserted through the anterior port following the “traffic light” model; the camera is positioned at the top red-light position, and a hand instrument is inserted at the green-light positions. 3 Then, another 3 mm or 5 mm trocar is inserted with direct vision at the 8th intercostal space for middle/lower lobectomy and the 7th intercostal space for upper lobectomy in the mid-axillary line (Fig. 1), based on the CT-scanned lesion location. We chose a standard anterior approach and single-direction dissection.4–6 Upper lobe resection: the upper lobe was rotated dorsally to expose the pulmonary hilum, and the superior pulmonary vein, upper lobe artery, and upper lobe bronchus were exposed from anterior to posterior. Middle lobe resection: the middle lobe was also rotated dorsally, and the middle lobe vein, middle lobe bronchus, and middle lobe artery were exposed from anterior to posterior. Lower lobe resection: according to the position of the working ports, the lower lobe artery, lower lobe bronchus and inferior pulmonary vein were exposed from head to foot (Fig. 2) . After removing the specimen from the single port in the anterior axillary line, the chest cavity was flushed with warm saline, and the lung was carefully examined to confirm that there was no active bleeding or air leak. After inflation of the lung, a chest tube was placed in the midline axillary puncture.

The position of the working ports.
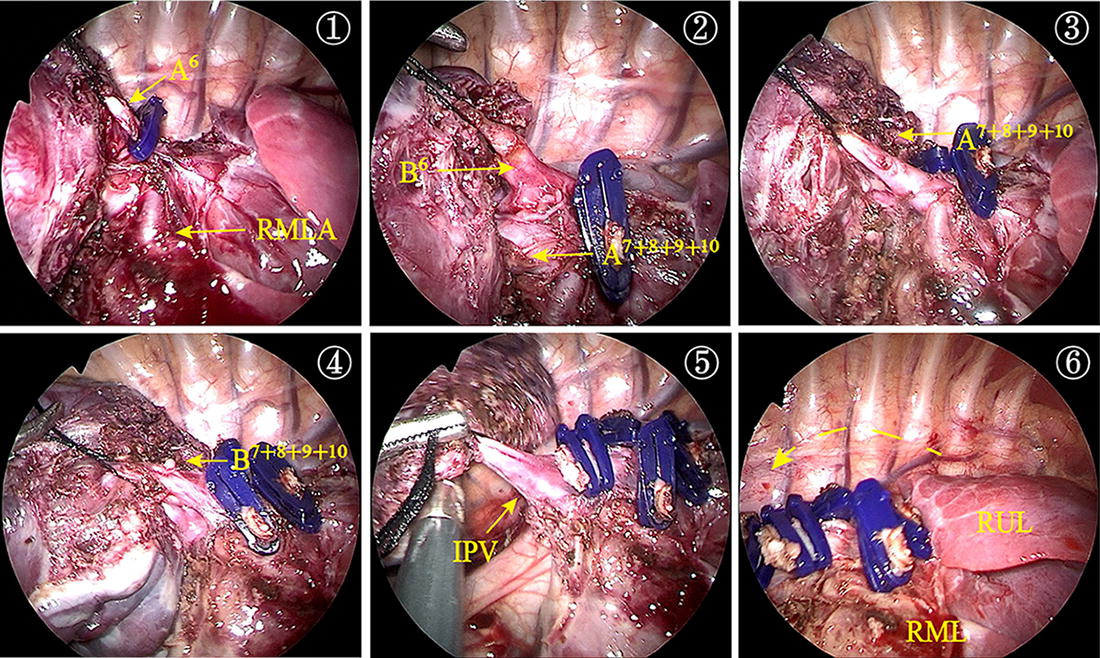
Right lower lobectomy: RMLA right middle lobe artery, IPV inferior pulmonary vein, RUL right upper lobe, RML right middle lobe, dotted line is shown as the anatomical direction.
Results
All 35 infants successfully completed SP + 1 thoracoscopic lobectomy. The average operation time was 65 minutes, ranging from 55 minutes to 100 minutes. The mean intraoperative blood loss was 16 mL, ranging from 5 mL to 30 mL. The postoperative drainage tube indwelling time was (3.0 ± 1.3) days, ranging from 2 days to 10 days. The postoperative hospital stay was (5.0 ± 1.5) days, ranging from 4 days to 13 days. There was 1 case of early postoperative air leakage, but there were no deaths, pulmonary infections, bleeding, atelectasis, bronchopleural fistulas, chylothorax, or other postoperative complications. All children recovered satisfactorily during their outpatient follow-up.
Discussion
Thoracoscopic surgery for CPAM has been expanding worldwide. Currently, the three-port method is the most widely used surgical technique in clinical practice. As surgeons improve their proficiency and skills in endoscopic surgical techniques, some researchers have started to investigate more “minimally invasive” techniques. Single-port thoracoscopic surgery offers the benefits of reduced chest wall trauma, less postoperative pain, and improved cosmetic outcomes. This technique has been well established and widely utilized in adult patients. 7 However, single-port thoracoscopic surgery in children is rarely reported in the literature due to the anatomical characteristics of the pediatric chest, the low incidence of thoracic diseases, the “chopstick” effect, and the limited operating angles during surgery. 8 Here, we designed a SP + 1 thoracoscopic surgery method and achieved favorable results in clinical practice.
Since the first report by Rothenburg in 1993 on thoracoscopic lobectomy in children and the subsequent detailed summary of the surgical procedure, the three-port method recommended by Rothenburg has become a standard surgical procedure for congenital lung malformation in children. 9 Although the three-port technique requires only three 3 mm or 5 mm incisions to perform the procedure, it is often necessary to enlarge one of the incisions while removing the specimen. We have developed an SP + 1 method that improves the three-port technique by incorporating camera port and a working port. This modified approach provides a convenient size for removing the entire excised lobe without further incision expansion, minimizing chest wall trauma and reducing postoperative pain by diminishing an incision (infamous in thoracic surgery),10,11 ultimately which avoids early pulmonary complications caused by postoperative pain and facilitates rapid postoperative recovery. Moreover, the method maintains the triangular target principle of the three-port technique, allowing for operation from various angles, facilitating bronchial and vascular dissection, while also circumventing the problems of instrument crowding, fencing and limited operating angles associated with single-port thoracoscopic surgery. In addition, this layout of camera allows for frontal vision of the target area; the surgeon operates with eyes and hands in the same plane, similar to thoracic surgery, as a result, the operator can easily identify the anatomical three-dimensional structural relationship.
Another challenge in pediatric thoracoscopic surgery is the limited space. Opting for the anterior approach, which takes into account the anatomy of the thoracic cage in infants, can enhance the operating distance and space. 8 Single-lung ventilation is the preferred mode of ventilation, as it allows for an expansive field of vision and space by collapsing the lung on the affected side. This can be accomplished by: double-lumen endotracheal intubation, which is only suitable for older children weighing over 30 kg; single-lumen endotracheal intubation with a bronchial blocker, which is challenging to manipulate and necessitates the aid of bronchoscopy; and single-lumen tracheal catheterization of the contralateral bronchus, which is a simple approach but may result in inadequate collapse of the affected lung, which commonly requires external pressure from artificial pneumothorax to achieve complete collapse. Selective endobronchial intubation was utilized in most cases during this study to achieve one-lung ventilation. The TRIPORT was employed to obtain a closed thoracic space, which can be combined with artificial pneumothorax and external pressure to induce adequate lung collapse. If the child is unable to tolerate one-lung ventilation during surgery, the anesthesiologist can reposition the tracheal tube to the main airway to facilitate bilateral lung ventilation and adjust the respiratory rate, tidal volume, and peak pressure in conjunction with artificial pneumothorax with a pressure of 4–6 mmHg and at a flow of 1–2 L/min to increase space and ensure procedural success. 9 For emphysema-type or large cystic lesions, it can be combined with an ultrasonic scalpel to shrink or fenestrate the lesions and create additional space.
The single-direction dissection, which has been successfully implemented in adults, has been deemed safe and feasible for performing lobectomy in children, as reported in a recent article. 12 Our procedure for upper and middle lobectomy is in accordance with this report. For lower lobectomy, we mostly employ a one-way dissection from head to foot, sequentially cutting off the lower pulmonary artery, lower pulmonary bronchus, and inferior pulmonary vein. Using this technique, each structure can be revealed sequentially and cut-off layer by layer, in keeping with the endoscopic perspective. It facilitates the spatial identification of anatomical structures while avoiding flipping the lung lobes in a small space, thus reducing surgical complexity and ensuring reproducibility.
In this study, one patient developed alveolar air leakage after the operation, and was discharged from the hospital after self-healing extubation by prolonging the indwelling time of the drainage tube without reoperation. During the operation, it was noted that the patient associates with severe incomplete interlobar fissure. When the interlobar artery, which was completely buried in the lung tissue, was exposed, the surgeon encountered an unclear direction, resulting in excessive anatomical resection of the lung tissue. In the follow-up cases, we adopted the pulmonary hilum approach, and the prognosis was significantly improved. 13 Benefit from the TRIPORT facilitated the use of various endoscopic instruments, ensuring proper closure of blood vessels and bronchi; no bleeding or bronchopleural fistula occurred post-operation. Generally, a 5 mm sealing device is sufficient for most pulmonary vessels and bronchi in infants. In a few cases, 10 mm sealing device is and 12 mm endoscopic linear staplers may be required to close large pulmonary vessels and bronchi; at this point, it is necessary to enlarge the SP incision to 20 mm. (Fig. 3).

Applying a 12 mm Endo-GIA to seal and cut off the bronchus.
In conclusion, SP + 1 thoracoscopic lobectomy for infants with CPAM is safe, feasible, and cosmetic. (Fig. 4). It can reduce chest wall trauma, relieve postoperative pain, and facilitate rapid postoperative recovery. Additionally, it maintains the triangular operating principle of conventional laparoscopic surgery, thus reducing the technical complexity of the procedure and increasing its reproducibility. There are still limitations to our study, including the inherent limitations of a single-center retrospective population study and a relatively small sample size that may restrict analytical capabilities. Future research should seek to confirm our findings through prospective and comparative studies.

The postoperative incisions.
Footnotes
Acknowledgments
The authors are grateful for the finical support provided by the Hebei Provincial Government Funded Clinical Medicine Excellent Talent Training Program “Research and Promotion of Screening and Treatment Techniques for Severe Structural Deformities” (2019008) DOI:10.3760/cma.j.cn101785 -202012064.
Authors’ Contributions
X.Y.: Conceptualization; writing—original draft. C.S. and H.Z.: Data curation; formal analysis. Y.W. and W.W.: Investigation. M.L.: Formal analysis; writing—review and editing. S.L.: Funding acquisition; writing—review and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Hebei Provincial Government Funded Clinical Medicine Excellent Talent Training Program (2019008).