
Abstract
Objective:
To evaluate the operative outcome of the use of intracavitary retractors in transumbilical laparoendoscopic single-site (LESS) adrenalectomy in comparison with the conventional multiport laparoendoscopic procedure.
Methods:
Between July 2021 and December 2023, 34 patients underwent transumbilical LESS adrenalectomy with intracavitary retractors, while 47 patients underwent conventional multiport laparoscopic adrenalectomy. Comprehensive data were compared, including demographics, intraoperative outcomes, perioperative complications, postoperative visual analog pain scale score, analgesic requirement, and short-term measures of convalescence.
Results:
Baseline characteristics were similar between the groups. All procedures were successfully completed without additional access or open conversion. The mean operative time and estimated blood loss for LESS adrenalectomy were comparable with multiport adrenalectomy. The LESS group had significantly shorter incision length (3.07 cm versus 5.16 cm, P < .01), lower postoperative pain scores (3.29 versus 4.91, P < .01), less analgesic drug use (29% versus 53%, P = .03), and better cosmetic scores (9.29 versus 7.28, P < .01). No significant differences were observed in time to resume oral intake, time to ambulation, or postoperative hospital stay. Complication rates were similar between the groups.
Conclusion:
The utilization of intracavitary retractors in transumbilical LESS adrenalectomy has demonstrated feasibility, effectiveness, and the potential to reduce technical complexities with satisfactory cosmetic effects. This technique enhances visualization of the surgical field without the need for extra ports.
Introduction
Adrenal tumors are commonly encountered neoplastic lesions in the field of urology. Although these tumors are typically benign, they often disrupt hormone balance and require surgical intervention. The primary goals of such procedures are to minimize surgical trauma and achieve aesthetically pleasing outcomes. Laparoscopic adrenal surgery is widely considered the preferred approach for the surgical treatment of adrenal tumors.1,2 However, multiport laparoscopic techniques can result in three to five permanent scars, affecting cosmetic appearance. 3 With advancements in surgical instruments and techniques, minimally invasive surgery has made significant improvements. Laparoendoscopic single-site (LESS) adrenalectomy is a minimally invasive procedure that leaves no visible scars or causes minimal scarring. This approach is not only less invasive but also promotes faster recovery and enhances the cosmetic result for the patient. 4
The umbilical region naturally serves as a scar. When performing LESS adrenalectomy through an umbilical incision, the surgical cut is concealed by the natural shape of the belly button, resulting in no visible scarring and improving the satisfaction of patients with the aesthetic outcome. However, the nearly parallel insertion of multiple instruments into the abdominal cavity presents a significant challenge in manipulating nearby organs. Additionally, the close proximity of the instruments often hinders the creation of a sufficient operative workspace, known as the “operational triangle,” which can lead to instrument interference and negatively impact the surgical process and visual field clarity. This technique is complex and requires a high level of technical skill, with a steep learning curve. 5 To address these challenges, we have developed a self-designed intracavitary retractor that assists in exposing the surgical area without the need for additional incisions. In this report, we shared our experience using the intracavitary retractor in LESS adrenalectomy and comparative aspects with the multiport laparoscopic adrenalectomy.
Methods
Patients
From July 2021 to December 2023, a total of 34 patients underwent transumbilical LESS adrenalectomy with the assistance of self-developed intracavitary retractors at our center. In the same time period, 47 patients underwent multiport laparoscopic adrenalectomy using a retroperitoneal approach. This study was approved by the ethics committee of the Second Affiliated Hospital of Nanjing Medical University.
All patients underwent preoperative assessment using either computed tomography or magnetic resonance imaging. The characteristics of the patients are described in Table 1. Transumbilical LESS adrenalectomy was exclusively recommended for unilateral adrenal tumors that met specific criteria: a small adrenal mass (≤4 cm). Larger tumors may require extending the incision, which would reduce the cosmetic effect of LESS procedures. If a preoperative examination indicated the presence of adrenal pheochromocytoma, hyperaldosteronism, or hypercortisolism, patients were advised to undergo appropriate pharmacological preparation in accordance with established guidelines. All procedures were performed by the senior surgeons. We administered a questionnaire 1 month after the surgery to assess the cosmetic score (ranging from 1 to 10) for each patient regarding their surgical scar.
Patient Demographics
ASA, American Society of Anesthesiologists; BMI, body mass index; LESS, laparoendoscopic single-site.
Surgical technique
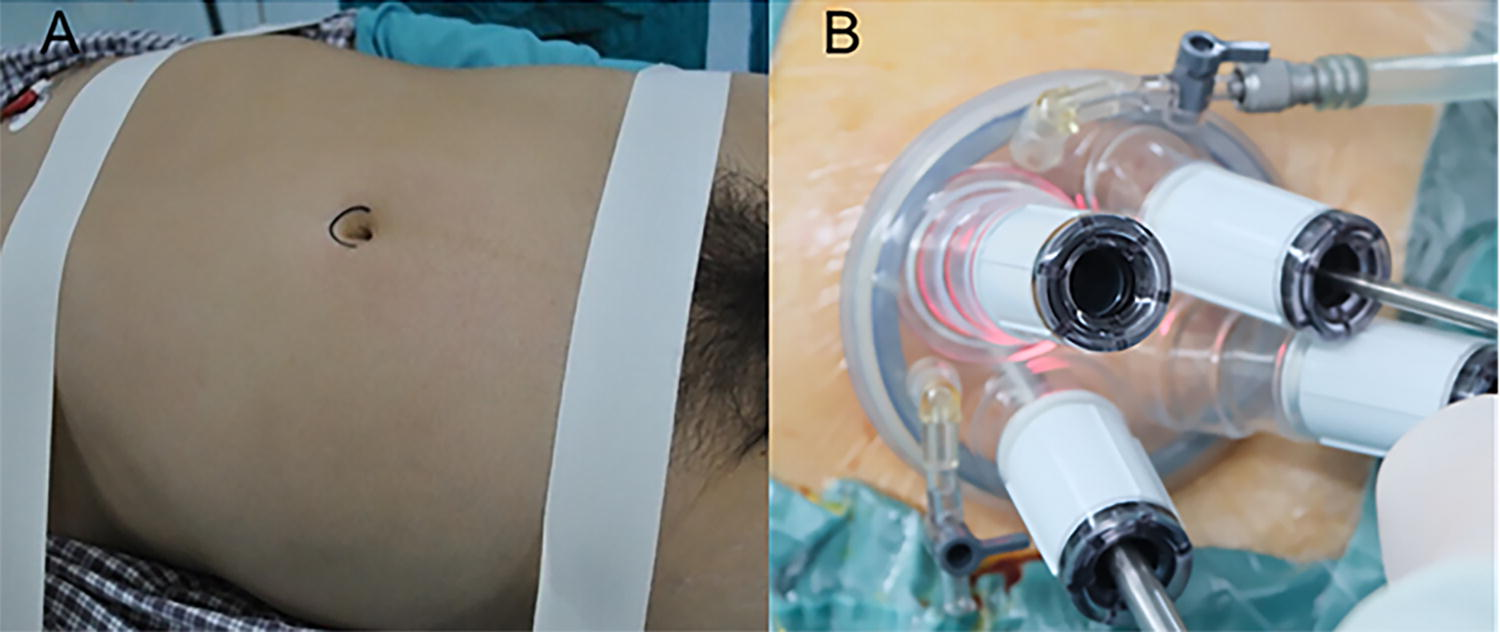
The patients, under general anesthesia with endotracheal tubes in place, were positioned at a 45° flank angle and supported with appropriate padding for stability and comfort (Fig. 1A). The operating table was then adjusted to position the patients in an almost supine position to facilitate making incisions. A transumbilical incision measuring ∼3 cm in length was performed. Following this, a multiport laparoscopic surgery trocar, which accommodated four ports (Lagis Enterprise Co., Ltd., China), was inserted (Fig. 1B). The operating table was then adjusted to position the patients in an almost lateral position. For the procedure, a 30° rigid laparoscope (Olympus Corporation, Japan) was used. There was no need for the utilization of angled laparoscopic instruments.
On the left side, the lateral peritoneum of the descending colon was incised along Toldt’s line, and the descending colon was opened along the blood-free anatomical space between the perirenal fascia and the mesocolon. Subsequently, we entered the avascular plane between the perirenal fascia and the mesocolon, opening the descending colon along this path. Our dissection continued upward, dissecting through the space, which involved separating the splenorenal ligament and the splenophrenic ligament. This technique allowed for the spleen and pancreatic tail to be exposed, leading to the visualization of the adrenal gland. Next, the perirenal fascia was incised to locate the left central adrenal vein at the upper margin of the left renal vein. Once the vein was isolated, it was securely ligated and severed. We proceeded to detach the upper pole of the kidney from the adrenal gland, staying close to the renal parenchyma surface. The dorsal aspect of the adrenal gland was released along the psoas major muscle’s surface. Following the division of the adrenal gland and the renal pedicle, the adrenal gland was carefully mobilized, and the tissue lying between the adrenal gland and the abdominal aorta was meticulously transected.
On the right side, after initiating the hepatic deltoid ligament’s partial transection and severing the hepatorenal ligament close to the liver’s lower extremity, the adrenal tissue was thoroughly revealed. Another assistant used Golden Finger through the port of the trocar for liver retraction (Fig. 2). The inferior vena cava’s sheath was then incised at the lower boundary of the caudate lobe, unveiling the right renal vein. Along the right edge of the inferior vena cava, we dissected the right central adrenal vein. Once the vein was isolated, it was securely ligated and severed. The kidney’s upper segment was carefully separated from the adrenal gland, with precise adherence to the surface of the renal parenchyma. Following the transection of tissue between the renal pedicle and the adrenal gland, we elevated and shifted the adrenal gland upward, skimming the surface of the psoas major muscle. The connecting tissue between the liver and the adrenal gland was meticulously dissected. We placed a negative pressure drainage tube, directing it through the initial incision site. The port was then removed, and the incision was closed with great care using precise suturing techniques.
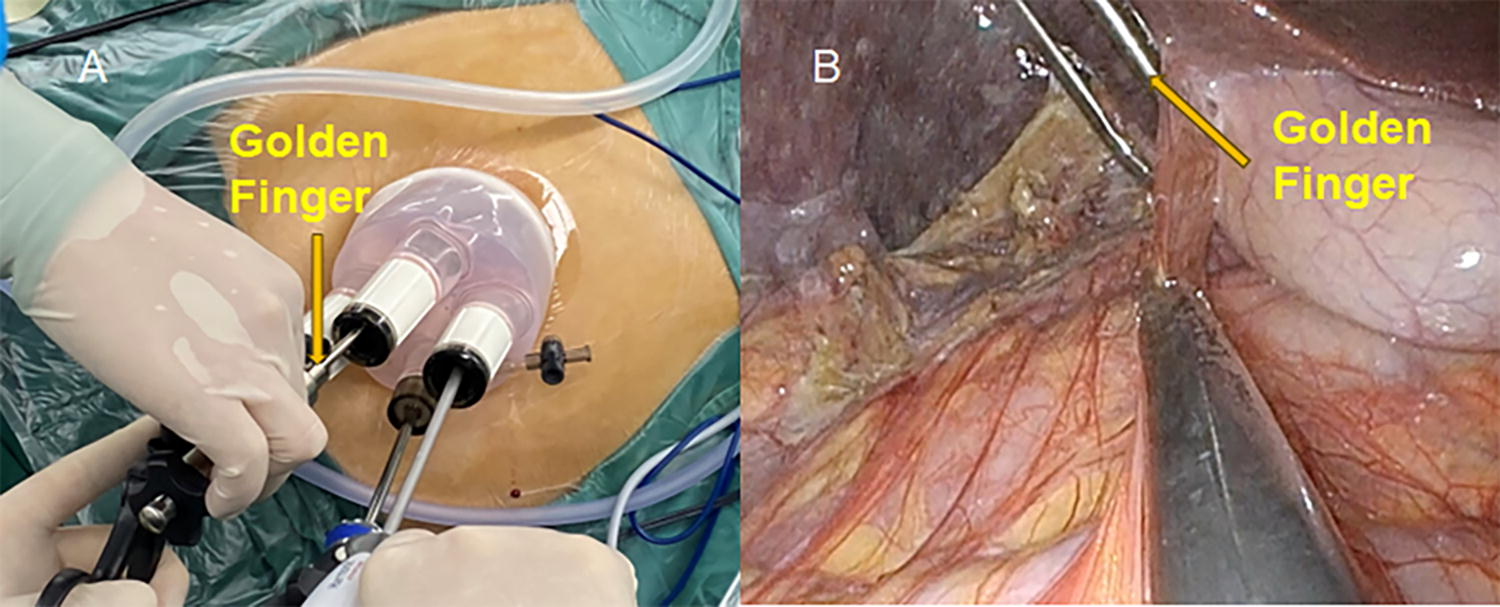
On the right side, the assistant used a Golden Finger through the port of the trocar for liver retraction.
To achieve sufficient exposure of the adrenal gland area, we utilized a self-developed intracavitary retractor (Fig. 3A). This retractor consists of a clamp without teeth at one end and a curved wire at the other, allowing for gentle and precise tissue manipulation. After adequately dissecting the surgical site (Fig. 3B), the retractor was secured with forceps and inserted into the abdominal cavity through a 12-mm trocar port. The clamp end without teeth was then attached to the tissues near the surgical site, including any fibrous or adipose tissue (Fig. 3C). The opposite end of the retractor was used to pull back the tissue on the other side. The central wires of the retractor were bent into an arc facing the abdominal cavity, enhancing visibility to assist with procedures such as dissecting the central adrenal vein (Fig. 3D). If the retraction during the procedure was deemed insufficient, we could add another retractor (Fig. 3E) or simply adjust the positioning of the retractor (Fig. 3F) to improve the exposure of the surgical field.

The retroperitoneal approach of multiport laparoscopic adrenalectomy has been wildly described by previous reports. 6
Statistical methods
Statistical analyses were conducted using IBM SPSS, version 23.0. Quantitative data were presented as mean ± standard deviation and analyzed using t-tests. For categorical data, the chi-square test was applied. Non-normally distributed quantitative data were described using medians, and group comparisons were performed using the rank-sum test, a non-parametric test. A P value <.05 was considered statistically significant.
Results
Baseline demographic characteristics were similar between the two groups (Table 1). The demographic characteristics of the patients were similar between the two groups in terms of age, gender, body mass index, American Society of Anesthesiologists classification, laterality, tumor size, and preoperative diagnosis. All procedures were successfully completed without the need for additional surgical access or conversion to open surgery.
In Table 2, we present the intraoperative and postoperative outcomes. The mean operative time for the LESS group was compared with that in the multiport group (85.44 ± 16.25 minutes versus 84.26 ± 13.83 minutes, P = .72). The mean incision length for the LESS group was 3.07 ± 0.22 cm, while the combined mean length of incisions in the multiport group was 5.16 ± 0.36 cm (P < .01). In the LESS group, the estimated blood loss was 38.82 ± 22.53 mL, whereas in the multiport group, it was 40.64 ± 25.40 mL (P = .74). None of the cases in either group required blood transfusion.
Intraoperative and Postoperative Results
VAPS, Visual analog pain scale.
The LESS group exhibited significantly lower postoperative Visual Analog Scale pain scores (3.29 ± 0.63 versus 4.91 ± 0.62, P < .01) and less analgesic drug use (29% versus 53%, P = .03) compared with the multiport group. There were no significant differences between the two groups regarding the time to resume oral intake, time to ambulation, or postoperative hospital stay.
There were no significant differences in the rates of complications observed between the two groups. In the LESS group, one case of delayed wound healing (Clavien grade I) and one case of postoperative fever treated with antibiotics (Clavien grade II) were reported. In the multiport group, two cases of subcutaneous emphysema (Clavien grade I) and one case of postoperative fever treated with antibiotics (Clavien grade II) were documented.
Discussion
Laparoendoscopic adrenalectomy is now the preferred method for removing small adrenal masses, renowned for its reliability, effectiveness, and low complication rates. Recent studies highlight the successful outcomes achieved with laparoendoscopic adrenalectomy through both transabdominal and retroperitoneal approaches. 7 Over the past decade, there has been a surge in investigations into single-incision laparoscopic surgeries that aim to minimize or eliminate scarring from operations. A recent comprehensive review contrasted the outcomes of LESS adrenalectomy with multiport laparoendoscopic adrenalectomy. 4 This review discovered that LESS adrenalectomy correlated with reduced pain after surgery and quicker recuperation times. However, the extended duration of surgery for LESS adrenalectomy in comparison with the multiport technique stands as a notable drawback. The technical difficulties encountered with LESS adrenalectomy, such as overlapping surgical instruments, less-than-ideal ergonomic conditions, and the lack of triangulation capability for tools, present substantial obstacles and have restricted its full-scale integration into medical practice.
Key discussions around LESS involve its steep learning curve, which often results in longer operative times and necessitates a high level of laparoscopic proficiency. To mitigate these challenges, strategies such as introducing extra surgical ports or needlescopic instruments, or alongside employing uniquely curved instruments, have been suggested. 8 In our study, we integrated several enhanced technical strategies and procedural tricks. First, we utilized a high-definition, long-shaft laparoscope with a 5 mm, 30° lens, allowing the assistant to maintain a clear working space free from the surgeon’s tools. Second, we leveraged the natural effects of gravity to aid in exposure where viable. It’s crucial to thoroughly separate the right liver as well as the left spleen and pancreas, with special care given to the ligament of the left splenic diaphragm. Placing the patient in a lateral position allows the spleen and pancreas to move aside from the operating area, thus granting ample exposure. More crucially, we utilized an intracavitary retractor to ensure superior retraction of the operative field without inflicting collateral damage during the surgery. For individuals who are obese or have perirenal adhesions, a pair of intracavitary retractors can be used simultaneously. By using intracavitary retractors, the operation time in LESS group was comparable with that in the multiport group, without any cases necessitating extra ports or conversion to conventional open surgery techniques.
In the patients treated with LESS adrenalectomy, a marked reduction in postoperative pain was observed when compared with the multiport group. A review of prior research indicates that the pain post-LESS adrenalectomy is inferior to that experienced following the conventional multiport procedures, whether these are performed transabdominally or retroperitoneally. 9 The administration of pain relief drugs postsurgery was noted in five separate analyses.10–14 Within these, 48.03% of patients who had undergone LESS adrenalectomy needed pain medication, a contrast to the greater 69.27% of those who required medication following multiport procedures. Our research revealed a similar trend, with the LESS adrenalectomy cohort using fewer analgesic drugs than the group undergoing multiport procedures. The LESS procedure is acknowledged as being less invasive when compared with standard laparoscopic methods, primarily due to the smaller incision size, which tends to result in less tissue damage. This particular aspect may contribute to the diminished pain levels experienced after surgery.
The primary advantage of LESS surgery is the better cosmetic outcome it offers. Patients, particularly younger individuals and those with benign conditions, tend to experience higher satisfaction levels due to this aspect of the procedure. 15 Previous studies have reported that patients in the LESS group, utilizing either the retroperitoneal or the transperitoneal approach, exhibited higher levels of satisfaction with regard to scar appearance compared with those in the multiport group.14–17 However, when it comes to aesthetics, the navel is often considered the most preferable entry point for LESS procedures. In transperitoneal LESS adrenalectomy, subcostal incisions tend to result in more noticeable scars as opposed to transumbilical incisions. 14 The results of our study demonstrated that the transumbilical incision in the LESS group was significantly smaller, leading to a higher cosmetic satisfaction score when compared with the multiport group.
Our study has some limitations. First, it should be acknowledged that our findings are not based on a randomized study design. Further investigations should be conducted, including randomized control trials, in order to obtain a higher level of evidence. Second, to optimize the cosmetic outcome, we performed LESS adrenalectomy using a transumbilical incision via the transperitoneal approach. However, due to surgical habits, our center routinely performs multiport procedures via a retroperitoneal approach. Previous studies have demonstrated the safety and comparable outcomes of both retroperitoneal and transabdominal laparoscopic adrenalectomy, particularly in experienced hands. Despite these limitations, our results still provide support for the effectiveness of intracavitary retractors in transumbilical LESS adrenalectomy.
Conclusion
The utilization of intracavitary retractors in transumbilical LESS adrenalectomy has demonstrated feasibility, effectiveness, and the potential to reduce the technical complexity of this procedure by enhancing the visualization of the surgical field without the need for adding extra ports.
Footnotes
Authors’ Contributions
Conceptualization: L.S. Methodology: W.L. and R.J. Formal analysis: H.H. and F.L. Data Curation: Y.W. Writing—Original Draft: W.L. and F.L. Writing—Review & Editing: H.H. and L.S. Supervision: Q.Z. Funding acquisition: L.S. and Q.Z.
Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work is supported by the medical research project of