
Abstract
Background:
Laparoscopic cholecystectomy is one of the most common surgical procedures. Several techniques of ligating the cystic duct have been compared in randomized trials, but data on comparative effectiveness are missing. Our aim was to systematically review the literature and, if appropriate, synthesize the available evidence.
Methods:
A systematic search of PubMed, Scopus, Ovid, and Cochrane Library was conducted to identify randomized studies comparing different ligation techniques of the cystic duct in laparoscopic cholecystectomy. Network meta-analysis synthesized evidence from all available techniques. Techniques compared were metal (MC), absorbable (AC), or polymer clips (PC), suture ligation (SL), and ultrasonic shears (US).
Results:
Twenty-three randomized studies with 2851 patients were included in our study. A well-connected network was formed for bile leak and a star-shaped network for operative time, with MC as the common comparator. No difference was found when SL, AC, US, or PC were compared for bile leak. Operative time was statistically significantly reduced when US were compared to MC (mean difference [MD] = −14.32 [−19.37, −9.28]), SL MD = −20.16 (−10.84, −29.47), and AC MD = −18.32 (−1.25, −35.39). The remaining techniques had similar operative times. PC had the highest probability of being the best technique P = 41.8, and SL had the highest probability P = 46.1 of being the second best for bile leak. US had a 98.1% chance of being the best technique for operative time.
Conclusions:
Given that all techniques demonstrate similar efficacy, the decision should be based on cost, familiarity with the technique, and environmental factors.
Introduction
Gallstones can affect up to 15% of the population, and once symptomatic, a cholecystectomy is indicated.1,2 Laparoscopic cholecystectomy (LC) remains one of the most common surgical procedures in the United Kingdom. 3 Bile leakage is a significant complication that can occur after a cholecystectomy and can reach up to 2%. 4 The most common cause of bile leakage is from the cystic duct stump and can be caused by poor application, slipping of the clips, or necrosis of the cystic duct stump. 5 Several techniques have been used to ligate the cystic duct in LC, such as metal (MC) or polymer clips (PC), ultrasonic shears (US), and suture ligation (SL), by forming an intracorporeal or extracorporeal knot or using a preformed loop. Multiple randomized trials comparing the above techniques have been reported with inconsistent or conflicting results. A recent pairwise meta-analysis, including 14 studies, four of which were randomized, could not recommend any of the above techniques. 6 A survey of current practice in the United Kingdom showed significant variability between surgeons. 7 Currently, the decision on the method of cystic duct closure is based on surgeon’s preference, cost, and availability. 8 This study aims to comprehensively assess all available techniques compared in randomized trials by systematically reviewing the literature and providing the first comparative effectiveness data.
Methods
The study protocol can be found in Prospero (CRD42022371647). The Prisma extension 9 for network meta-analysis has been used as a reporting guideline in this meta-analysis.
Inclusion and exclusion criteria
Randomized trials comparing different techniques of cystic duct ligation in LC have been considered for inclusion in our study. Nonrandomized studies were not considered for inclusion to protect transitivity and to prevent the introduction of selection bias in our review. Studies reporting on ex vivo techniques, animal studies, or using a combination of two techniques for ligation of the cystic duct were excluded. Our primary outcome was bile leakage. Secondary outcomes included bile duct injury (BDI), reoperation, operating time, length of hospital stay, and surgical site infection. In the event of two studies being published with an overlapping population, the most recent study was included in our review. There was no limitation on publication language, publication status, or indication for cholecystectomy.
Search and selection strategy
PubMed, Embase (Scopus), Ovid, and Cochrane Library were interrogated for studies fulfilling the inclusion and exclusion criteria by two of the authors independently till October 2022. If there was disagreement between the authors regarding inclusion of a study, a senior author was consulted. The following search terms and their combination were used: laparoscopic cholecystectomy, cholecystectomy, gallbladder removal/excision, cystic duct ligation or ligature, metal clip, absorbable clip, Hem-o-lok, polymer clips, suture ligation, suture, ultrasonic shears, random, and randomized clinical trial (RCT).
Data abstraction and validity assessment
Data on possible effect modifiers such as age, gender, cystic duct size, percentage of complicated cholecystitis, and presence of common bile duct stones were extracted from all studies independently by two of the authors. Inclusion and exclusion criteria, year and country of publication, and outcomes of interest such as bile leakage, BDI, operating time, reoperation, length of stay, failure of the technique of choice to ligate the cystic duct, rates of biloma/abscess, mortality, and appropriate use of statistical methodology were extracted to tables. The Jadad score was used for the quality assessment of the included studies.
Data analysis
Pairwise meta-analysis
Both pairwise and the network meta-analyses were performed in Stata 14 MP. The odds ratio (OR) and its confidence interval (CI) were calculated and reported for dichotomous outcomes. Enough data to form a contingency 2 by 2 table were needed to be reported by studies for dichotomous outcomes to be included in this meta-analysis. The Mantel–Haenszel test was used in the analysis of dichotomous data. The mean and standard deviation or median and range had to be reported for continuous outcomes to be included in our study. The weighted-mean difference (WMD) was calculated and reported for continuous outcomes. The chi square and I2 were calculated to test the presence of statistical heterogeneity. Moderate heterogeneity was considered when I2 >30% and substantial heterogeneity when I2 > 50%. The fixed and random effects of model were reported according to the level of statistical heterogeneity. Publication bias was investigated by examining funnel plots. Sensitivity analysis was performed according to the quality of the studies.
Network meta-analysis
Network meta-analysis is a generalization of pairwise meta-analysis. It can synthesize evidence from multiarm studies and studies comparing different techniques by pooling direct and indirect evidence from common comparators. Network meta-analysis can provide data on the comparative efficacy of all techniques and calculate the probability of each technique being the best. Furthermore, all available techniques can be ranked from best to worst. 10 A network plot was formed for each outcome of interest. Each technique of interest was represented with nodes and each comparison with an edge. For each outcome of interest, a network plot was created and its geometry assessed. Overall inconsistency was tested using the Stata inconsistency model and loop inconsistency using the loop splitting model. In the event of significant inconsistency, the Lu and Ades model was reported. Continuous outcomes were reported as WMD, and 95% Credible Intervals (CrI) and dichotomous outcomes were reported as logOR and 95% CrI. Surface under the cumulative ranking curve (SUCRA) and P scores were used to rank all techniques. A probability of more than 90% of being the best technique was required to be given credence. The frequentist approach was used in this network meta-analysis.
Results
Selection and quality assessment
The systematic search of databases identified 1357 studies. Twenty-eight RCTs8,11–26 were found, of which five27–31 were excluded as in both groups the same or a combination of two techniques were used for ligation of the cystic duct or different techniques for cholecystectomy were described in the two groups. The total number of patients in this review was 2851. Ten studies compared US to MC, eight compared SL to MC, one compared SL to PC, two compared AC to MC, and one compared SL to PC. One multiarm study compared AC to US and SL. Only four11,14,15,23 of the studies reported on the percentage of patients who had acute cholecystitis ranging from 6.7% to 100%. With the exception of one 14 study that included only acute cholecystitis patients, the remaining did not report on outcomes of acute cholecystitis patients separately. Nine studies reported on conversion to open surgery, with four12,20,25,32 of the studies reporting a conversion rate of zero and the remaining reporting conversion rates of 2.9% to 33%. Quality assessment of the studies can be found in the appendix.
Pairwise meta-analysis
US versus MC
Bile leakage
Bile leakage was reported in ten13–15,17,19,20,25,33–35 studies, seven13,17,20,25,33–35 of which reported no cases of bile leakage. No statistical heterogeneity was identified I2 = 0. No statistically significant difference was found between the US and the MC [OR = .75 (.16, 3.39); P = .70].
Operative time (minutes)
Nine studies reported this outcome.13–15,17,19,20,25,33,34 There was significant statistical heterogeneity I2 = 97%. The random effects model was reported. A statistically significant difference was found favoring the US group with a decrease in operative time [WMD = −16.20 (−17.15, −15.25); P < .00001].
Hospital stay (days)
Seven studies reported this outcome.14,15,17,19,20,25,34 There was significant statistical heterogeneity I2 = 88%, so the random effects model was reported. No significant difference was identified in hospital stay [WMD = −.18 (−.24, −.13); P < .00001].
Biloma/Abscess
Four studies19,20,25,34 reported this outcome of which one reported no cases. No statistically significant difference was found between US and MC [OR = .44 (.10, 2.02); P = .29].
SL versus MC
Bile leakage
This outcome was reported in eight studies,8,18,21–24,26,36 four8,22,26,36 of which reported no cases. No statistically significant difference was found between SL and MC [OR = .39 (.13, 1.17); P = .09] with no statistical heterogeneity.
Operative time (minutes)
This outcome was reported in three studies.21,23,26 Moderate statistical heterogeneity (I2 = 43%) was identified. A statistically significant difference was found favoring MC with a decrease in operative time [WMD = 3.07 (1.67, 4.48); P < .0001].
Network meta-analysis
MC were used as the common comparator. Interval and SUCRA plots were drawn for all outcomes of interest. The pooled OR was reported for binary outcomes and MD and CrI for continuous outcomes.
Bile leakage
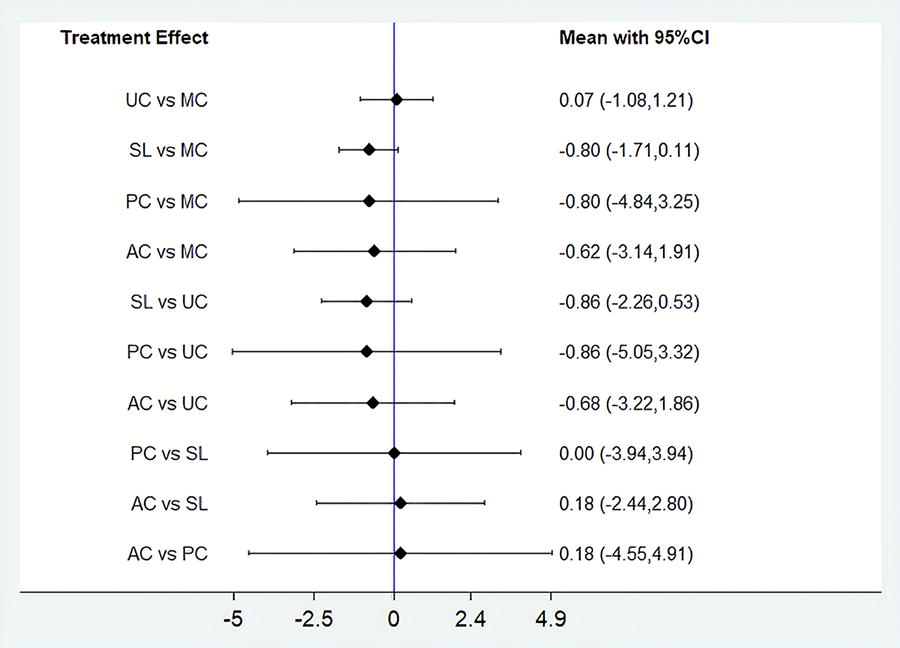
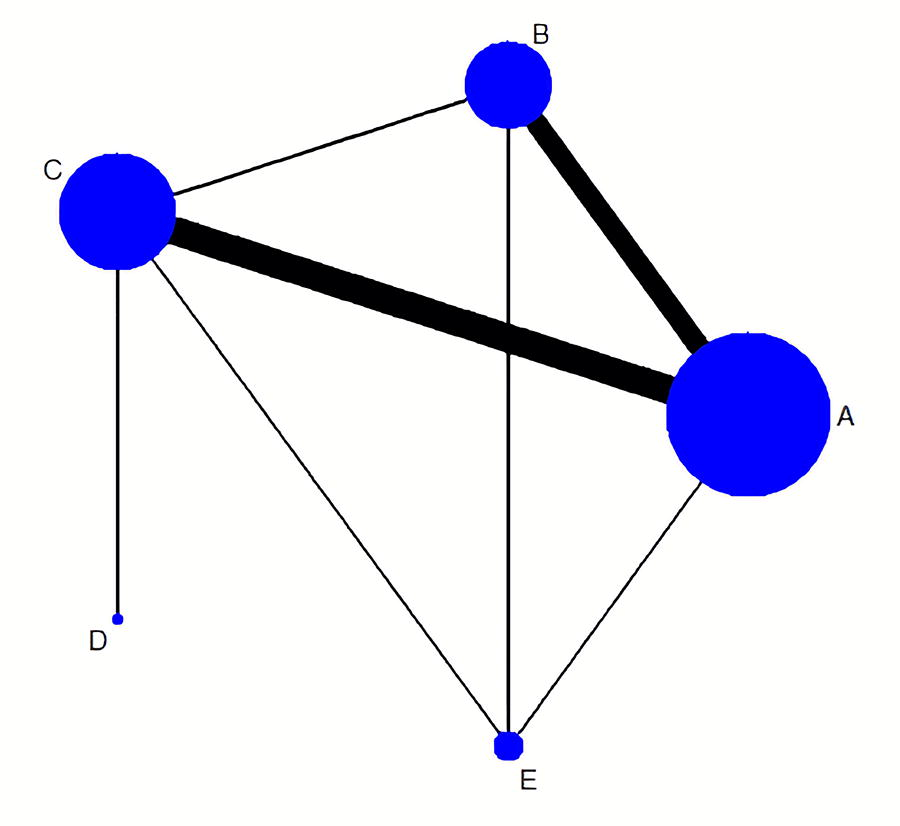
Assessment of the network geometry for bile leakage revealed a well-connected network (Fig. 1). No inconsistency was identified in this outcome. The majority of the evidence comes from studies comparing SL and US to MC. When PC were compared with MC OR = −.80 (−4.84, 3.25), SL with MC OR = −.80(−1.71, .11), or SL with PC OR = .00(−3.94, 3.94), no statistically significant difference was identified for bile leakage (Fig. 2). No difference was found when PC were compared with AC or US. No statistically significant difference was identified in the remaining comparisons. PC (P = 41.8%), AC (P = 29.2%), and SL (P = 25.5%) were the three techniques with the highest probability of having the lowest leak rate.
Network Plot Bile Leakage.
Interval Plot Bile Leakage.
Operative time
A star-shaped network with common comparator, the MC technique, was drawn for this outcome. When US were compared with MC, a reduction of operative time (MD −14.32 and 95% CrI [−19.37, −9.28]) was found. Compared with SL MD = −20.16 (−10.84, −29.47) and AC MD = −18.32 (−1.25, −35.39), a reduction in operative time was noticed. The rest of the techniques had equivalent operative time. US had a 98.1% chance of being the technique with the shortest operative time, and MC had a 63.4% chance of being the second-best technique.
Intra-abdominal collection/biloma
A star-shaped network with common comparator, MC technique, was drawn for this outcome. No difference was identified when US OR = −.70 (−2.12, .72) or SL OR= .00 (−3.96, 3.96) was compared with MC. SL compared with US OR = .70 (−3.50, 4.91) had no difference for this outcome. The rest of the techniques had equivalent operative time. US had a 56.2% chance of being the technique, and MC had a 50.5% chance of being the second-best technique.
Hospital stay
This outcome was reported only by studies comparing MC with US, and its meta-analytical outcomes can be found in the pairwise meta-analysis section.
Discussion
To the best of our knowledge, this is the first network meta-analysis providing comparative efficacy data on techniques used to ligate the cystic duct in laparoscopic cholecystectomy. Although several randomized trials have been published, clear evidence of any technique’s superiority had not been established yet. A previous Cochrane review, 31 including three randomized trials, and a pairwise meta-analysis, 6 including five randomized and observational studies, also could not reach any conclusions.
This network meta-analysis showed that all techniques had an equivalent bile leak rate. Unfortunately, data on complicated cholecystitis or cases with a dilated common bile duct are not reported in most of the included studies. Most of the evidence comes from direct comparisons of studies comparing US and SL with MC. PC had the highest chance of being the best technique for this outcome, but did not reach the required predefined probability of 90%.
Regarding operative time, US had a clear advantage compared with all other techniques. Minimizing instrument changes and quicker gallbladder dissection from the liver bed can explain this. The rest of the techniques were equivalent regarding operative time. Hospital stay was reported only by studies comparing US and MC, and both techniques had equivalent outcomes, as expected. Regarding biloma, no difference was found between the techniques. Due to the paucity of data on complicated cholecystitis or cases with dilated cystic ducts, sensitivity analysis could not be performed. Variability was also noticed in the quality of studies. Statistical heterogeneity reflects the variability of inclusion and exclusion criteria, as well as differences in the learning curve of the operating surgeons and their familiarity with the technique used.
In this network meta-analysis, the results of both the pairwise and network meta-analysis are in concordance, which suggests that the transitivity assumption holds. Network meta-analysis synthesizes evidence from all available techniques and provides comparative effectiveness data even in techniques that have not been compared in a head-to-head trial. Network meta-analysis has the advantage of identifying statistical significance quicker and more efficiently than pairwise meta-analysis. 32
Given that all techniques demonstrate similar efficacy, environmental and sustainability factors should influence the decision-making process. Reusable MC and PC can significantly decrease costs. The cost of the endoloop is slightly higher, 37 at $17 (£13.50) in the United Kingdom, and sometimes applying an endoloop or ligating the cystic duct laparoscopically can be time-consuming and cumbersome. However, this must be weighed against the time efficiency offered by US. In high-income countries, where the cost of operating time can be up to $46.04 ± $32.31 per minute, 38 the 16-minute decrease in time translates to a $736 saving. However, the cost of the device could be similar, making cost-effectiveness a critical consideration.
Our study found that all the evaluated techniques have equivalent efficacy in chronic cholecystitis/biliary colic cases. The decision should be based on cost, familiarity with the technique, and environmental reasons.
Footnotes
Authors’ Contributions
C.A.: Conceptualization, methodology, investigation, formal analysis, writing—original draft, and writing—review and editing. A.R.: Data curation, investigation, methodology, and writing—review and editing. M.S.Q.: Data curation, investigation, methodology, and writing—review and editing. V.K.: Supervision, validation, and writing—review and editing. A.K.: Supervision, validation, and writing—review and editing. S.A.: Supervision, validation, and writing—review and editing.
Author Disclosure Statement
There are no conflicts of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.