
Abstract
Background:
Esophageal cancer surgery aims for curative intent but carries high complication rates. Transthoracic esophagectomy is the dominant approach, however, transhiatal esophagectomy (THE) offers selective advantages in certain clinical scenarios. Minimally invasive THE (MI-THE) is an evolving technique with limited data.
Methods:
This retrospective study reviewed 38 patients with esophageal cancer who underwent MI-THE using “Antegrade Inversion Technique” between 2013 and 2023 at a tertiary care center. Perioperative outcomes were analyzed. Data were presented as mean with standard deviation, median with interquartile range, and percentages.
Results:
Most patients (86.8%) had early-stage cancer. Median operative time was 375 minutes, hospital stay was 8 days, and intensive care unit stay was 3 days. All patients achieved a negative resection margin. Pleural effusion (57.9%) was the most common complication, followed by pneumothorax (31.6%) and surgical site infection (15.8%). Anastomotic leak rate was 13.2%. There was no mortality.
Conclusions:
MI-THE appears safe and feasible with encouraging perioperative outcomes, particularly for early-stage disease and high-risk patients. While potentially offering advantages over open THE, further research is needed to definitively establish its role compared to traditional approaches.
Introduction
Esophageal cancer is an aggressive disease with a poor prognosis. Despite advancements in multimodal treatment, surgery remains the cornerstone of curative treatment. Esophagectomy is a major gastrointestinal surgical procedure with significant morbidity and mortality rates.1–3 Postoperative complications not only diminish the quality of life but also adversely impact long-term survival rates.4,5 There are two primary approaches: transhiatal esophagectomy (THE) and transthoracic esophagectomy (TTE). The advantages and disadvantages of these approaches have been extensively debated.
Since its introduction by Orringer and Sloan in 1978, THE has gained popularity as an alternative to TTE, offering decreased pulmonary morbidity. 6 Several studies have highlighted THE advantages in the early postoperative period. Over the past few decades, there’s been a shift toward minimally invasive esophagectomy (MIE). MIE has become widely accepted, with studies showing similar long-term outcomes to open surgery but with lower complication rates and improved quality of life.7–10 In addition, when an anastomotic leak occurred, the associated morbidity was significantly lower as compared to cases of intrathoracic leakage in TTE. 11 Several retrospective and prospectively controlled studies have been conducted comparing and contrasting the effectiveness between THE and TTE approaches.3,12–15
Over the past few decades, there’s been a clear shift toward minimally invasive (MI) approaches in esophageal cancer surgery with the aims of improving survival rates while reducing complications and mortality. At present, MIE has become widely accepted.16–18 Several randomized controlled trials have compared MI-TTE with the open approach. These studies found similar 3-year disease-free survival (DFS) rates with MI-TTE, but with the added benefits of lower complication rates and improved quality of life for patients.18–21 MI-THE was first described by DePaula et al. 22 While its safety and effectiveness have been confirmed in retrospective studies, there’s a lack of large-scale trials comparing MI-THE to open THE (O-THE). This study aims to describe our surgical technique “Antegrade Inversion Technique” for MI-THE and evaluate the perioperative outcomes in esophageal cancer.
Methods
Patient selection
This retrospective study reviewed esophageal cancer patients who underwent MI-THE at our institution between 2013 and 2023. Patients requiring conversion to open surgery or unable to undergo anastomosis were excluded. All patients provided written informed consent for inclusion in the database (IRB#1759).
Preoperative staging involved CT scans, PET scans, and multidisciplinary review. Neoadjuvant chemoradiotherapy was administered as indicated. We used the American Joint Commission on Cancer (AJCC) 8th Edition for cancer staging. Operative details, including duration, blood loss, and hospital stay, were recorded. The duration of surgery was recorded in minutes, blood loss in milliliters, and hospital stay in days. Re-admission was defined as hospitalization required for surgical complications within 6 months of surgery. Hospital mortality was defined as death within 90 days of surgery.
Operative procedure and technique
Laparoscopic phase
Before the operation, the patient’s cervical range of motion is assessed, followed by prophylactic antibiotics and antiembolism stockings. A nasogastric tube is placed. The patient is positioned in a split-legged posture, arms tucked, with a gel shoulder roll installed for maximal neck extension. The laparoscopic phase begins with a Veress needle insertion at Palmer’s point to create pneumoperitoneum. Port placement is determined by the patient’s body habitus and any previous abdominal surgeries (Fig. 1). The camera port is positioned 17 cm below the xiphoid process in the left paraumbilical area. A left 12-mm working port is placed ∼12 cm laterally from the sternal tip and 3 cm below the left rib margin. Another 12-mm working port is positioned beneath the right rib margin, 9 cm from the xiphoid process, and 3–5 cm down depending on the left liver lobe size. A 5-mm trocar is placed in the lateral left axillary line for the first assistant and a final 5-mm port is inserted in the patient’s right mid-abdomen, usually at the level of the umbilicus. A Nathanson liver retractor is used to elevate the left liver lobe.
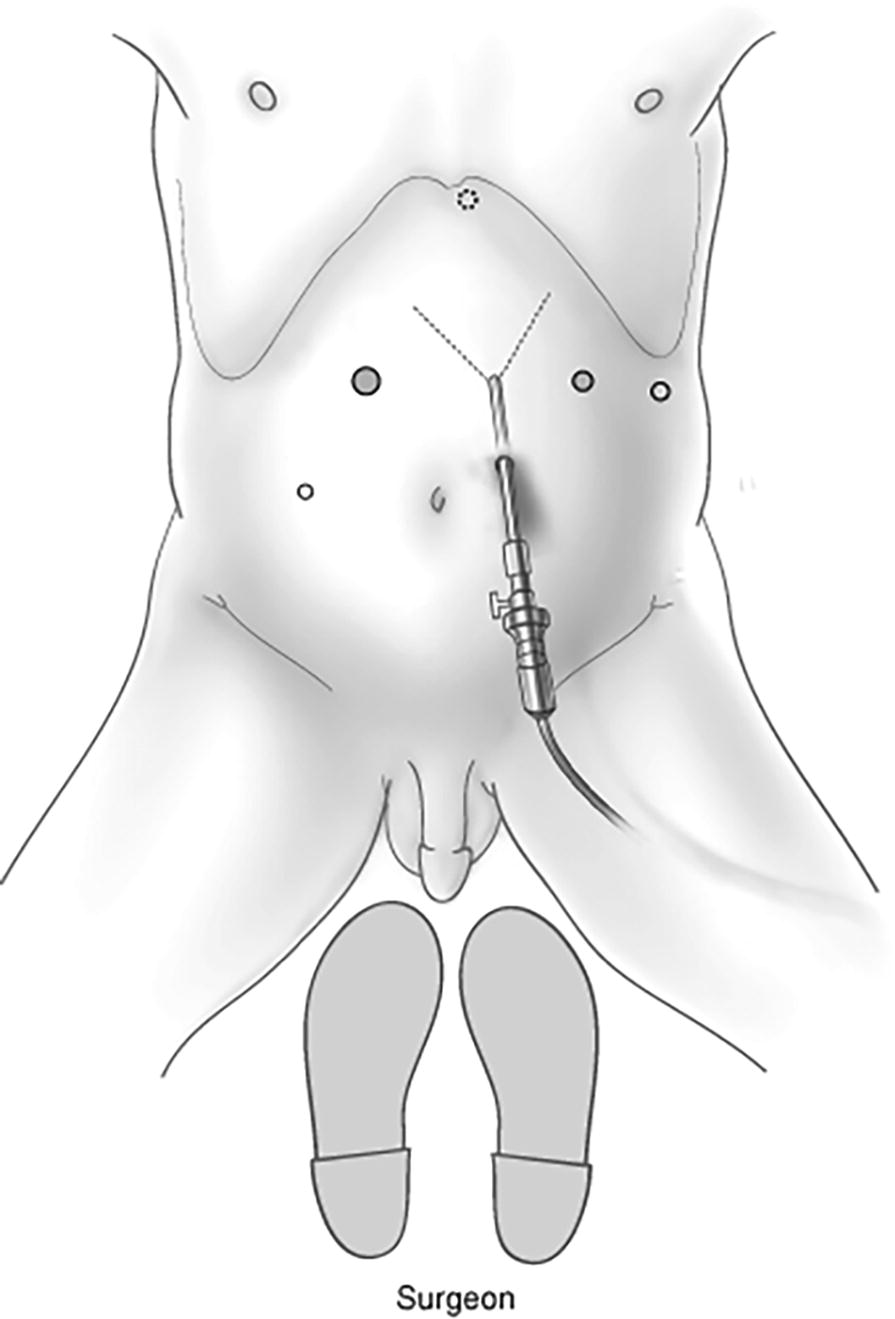
Port placement demonstration. (Reproduced from “Atlas of Minimally Invasive Surgical Operations” with permission from Corinne Sandone, CMI, FAMI, © 2018 JHU AAM; Department of Art as Applied to Medicine; The Johns Hopkins University School of Medicine.).
The ultrasonic dissector divides the gastrohepatic ligament along the right gastric vessels, liver edge to phrenoesophageal ligament. The short gastric vessels and entire gastrocolic omentum are divided, with careful preservation of the right gastroepiploic pedicle (Fig. 2). Posterior medial mobilization of the stomach continues until the gastroduodenal artery becomes visible. An extensive Kocher maneuver (mobilization of the duodenum along the lateral attachments) is performed to expose the posterior pancreatic head and thus freeing the third portion of the duodenum, and facilitating mobilization that is demonstrated by lifting the pylorus toward the diaphragmatic hiatus.

Division of the gastrocolic ligament. (Reproduced from “Atlas of Minimally Invasive Surgical Operations” with permission from Corinne Sandone, CMI, FAMI, © 2018 JHU AAM; Department of Art as Applied to Medicine; The Johns Hopkins University School of Medicine.).
Next, the posterior esophageal window is created by dissecting the right crus, encircling the esophagus with a Penrose drain, mobilizing the mid-to-distal esophagus, and clearing the posterior mediastinum. The celiac lymph nodes along the splenic and hepatic arteries at the pancreas’ superior border are then dissected. Proximal left gastric pedicle lymphadenectomy involves isolating left gastric vessels and transection with a vascular sealing linear stapler (Fig. 3). The gastric conduit is created by selecting a point on the lesser curvature 5 cm proximal to the pylorus. The site is cleared of attachments and transected the right gastric vessels using a vascular load stapler. The surgeon flattens the stomach by retracting the superolateral curve and pulling inferomedially. This allows for creation of a 3-cm wide conduit with sequential endo-stapling devices through the right upper abdominal 12-mm port (Fig. 4).
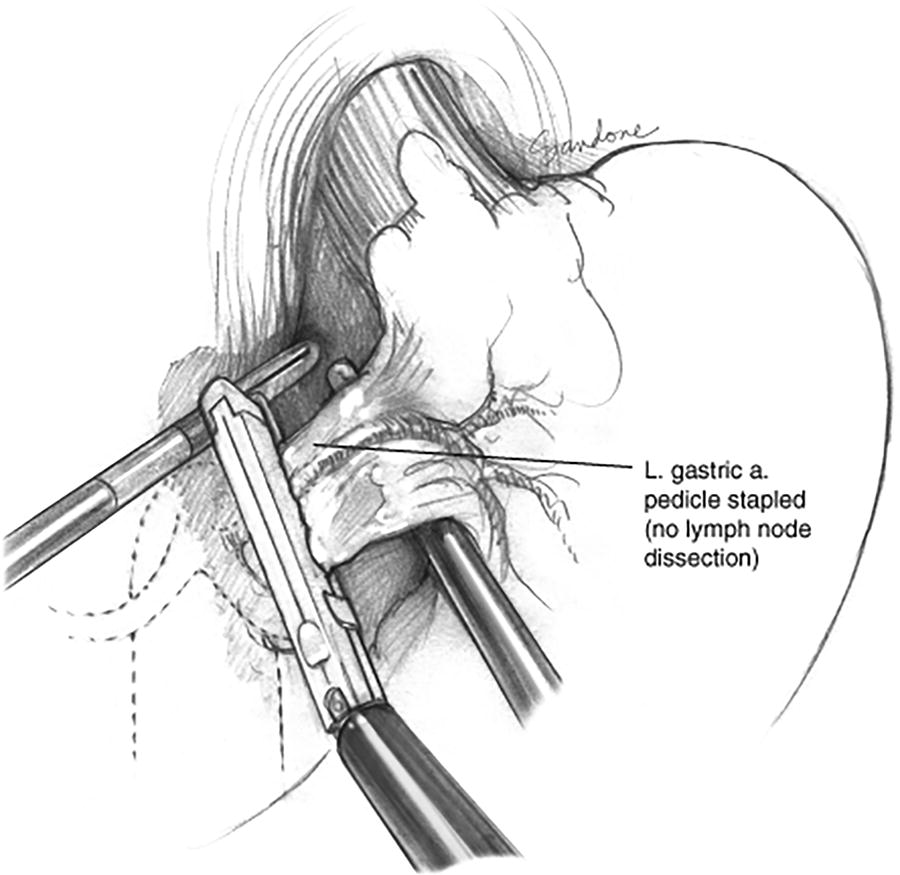
Left gastric vessel dissection and transection. (Reproduced from “Atlas of Minimally Invasive Surgical Operations” with permission from Corinne Sandone, CMI, FAMI, © 2018 JHU AAM; Department of Art as Applied to Medicine; The Johns Hopkins University School of Medicine.).
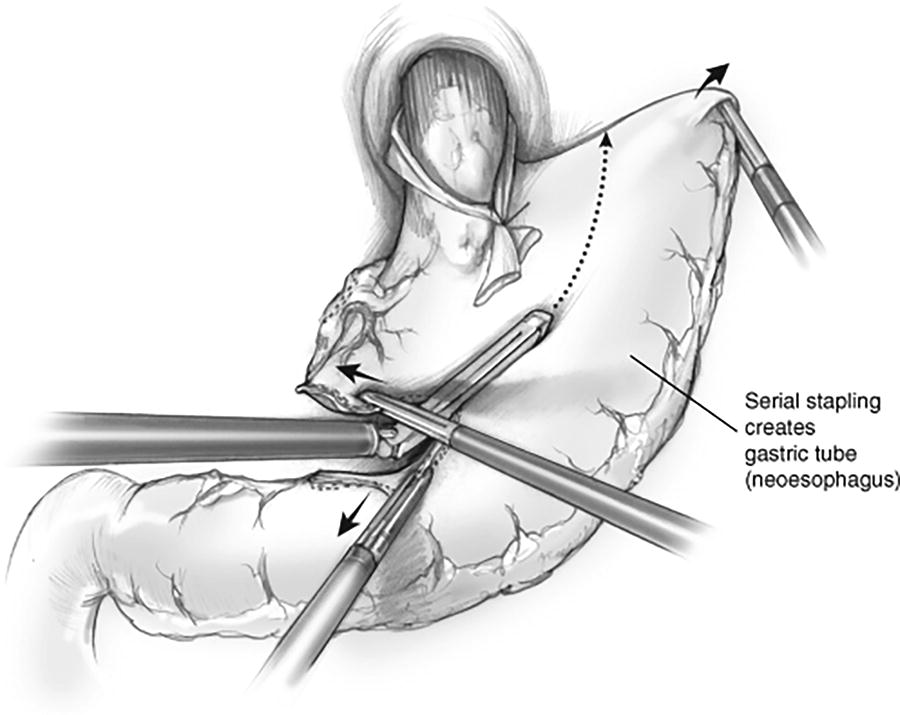
Creation of gastric conduit. (Reproduced from “Atlas of Minimally Invasive Surgical Operations” with permission from Corinne Sandone, CMI, FAMI, © 2018 JHU AAM; Department of Art as Applied to Medicine; The Johns Hopkins University School of Medicine.).
Cervical phase
The cervical phase involves a left transverse neck incision above the clavicle, creating subplatysmal flaps, and dividing the strap muscle groups. The thyroid gland is retracted infero-medially and the inferior thyroid artery and middle thyroid vein are accessed, divided, and ligated with silk sutures. Tissue attachments and small vessels are cauterized or ligated to avoid injuring the recurrent laryngeal nerve, which is visualized after exposure and retraction of the thyroid is achieved. Peri-esophageal tissue is divided on the esophagus. An umbilical tape is placed around the esophagus with the aid of the renal pedicle clamp, and the remaining tissues are bluntly dissected. After optimal inferior dissection, the nasogastric tube is retracted and distal stay sutures are placed on the lateral esophageal walls. The cervical esophagus is transected with a linear cutting stapler above the stay sutures, while maximizing the proximal esophageal length.
Antegrade inversion technique
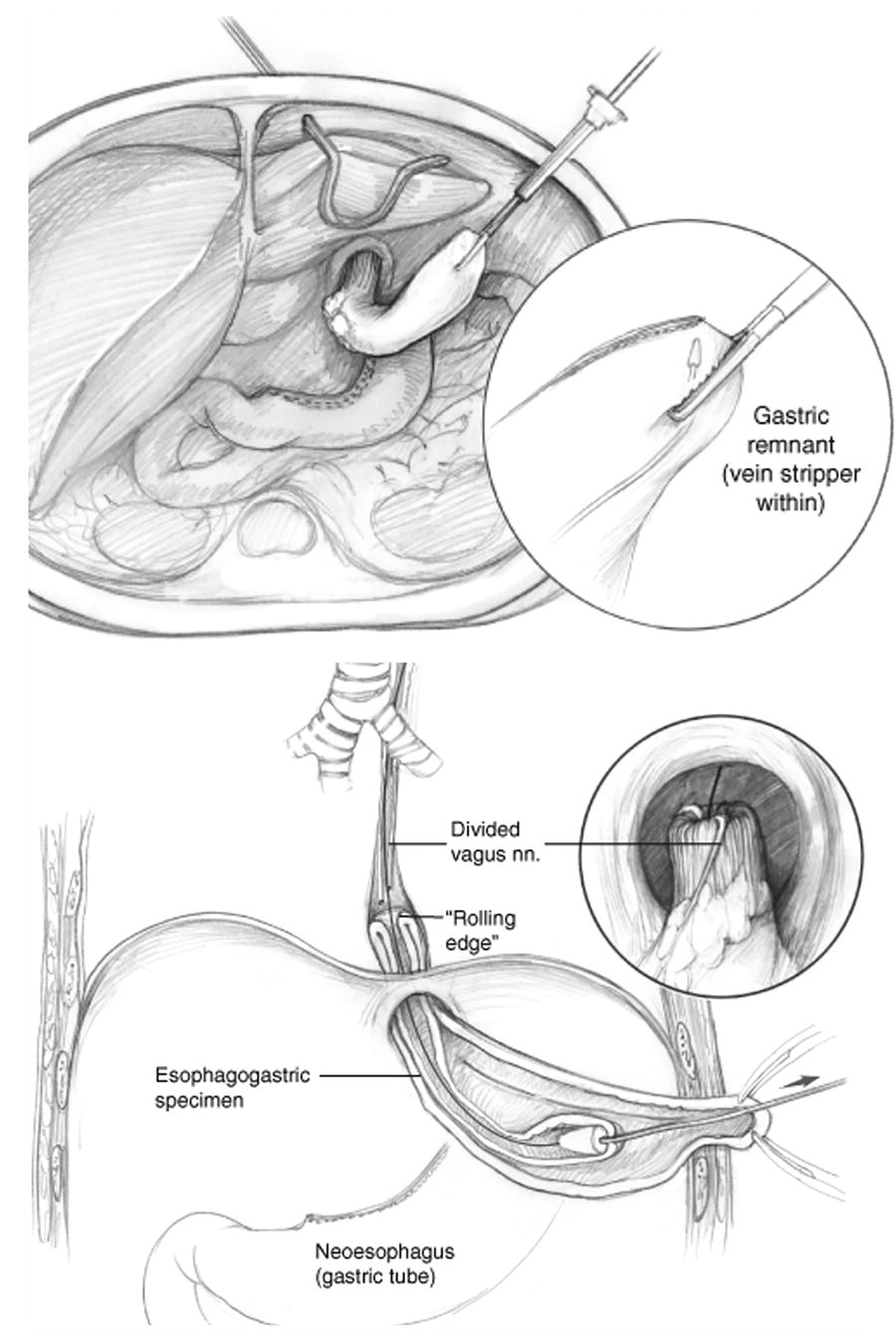
The mid-esophageal section is dissected using a vein stripper device and an antegrade inversion technique. This method is preferred for preserving the esophagogastric junction, avoiding cancer seeding, and minimizing wound contamination. A minor esophagotomy is performed to facilitate the passage of the vein stripper and two stay sutures and a purse string are placed into the proximal stapled end of the esophagus. The vein stripper is inserted and demonstrated to slide easily into the mucosa of the esophagus (Fig. 5). The vein stripper’s tip is directed toward the apex of the lesser curvature gastric specimen. The left upper laparoscopic 12-mm port site is extended and a wound protector device is inserted instead of the port. The gastric remnant is grasped (across the tip of the vein stripper) and extracted from the left subcostal port site. The stomach tip is grasped with hemostats and the vein stripper’s tip is accessed with a small gastrotomy. The abdomen is re-insufflated and two surgical gauzes are introduced to prepare for potential bleeding which if occurs, can be significant and the team has to be prepared for this. If the vagus nerve has not been divided, it will need to be divided before specimen extraction. The antegrade stripping procedure involves using a long silk suture to connect the inverted esophagus to the bougie dilator at the neck as it passes through the hiatus. The specimen is pulled through the left upper quadrant port site, and the abdomen is re-insufflated.
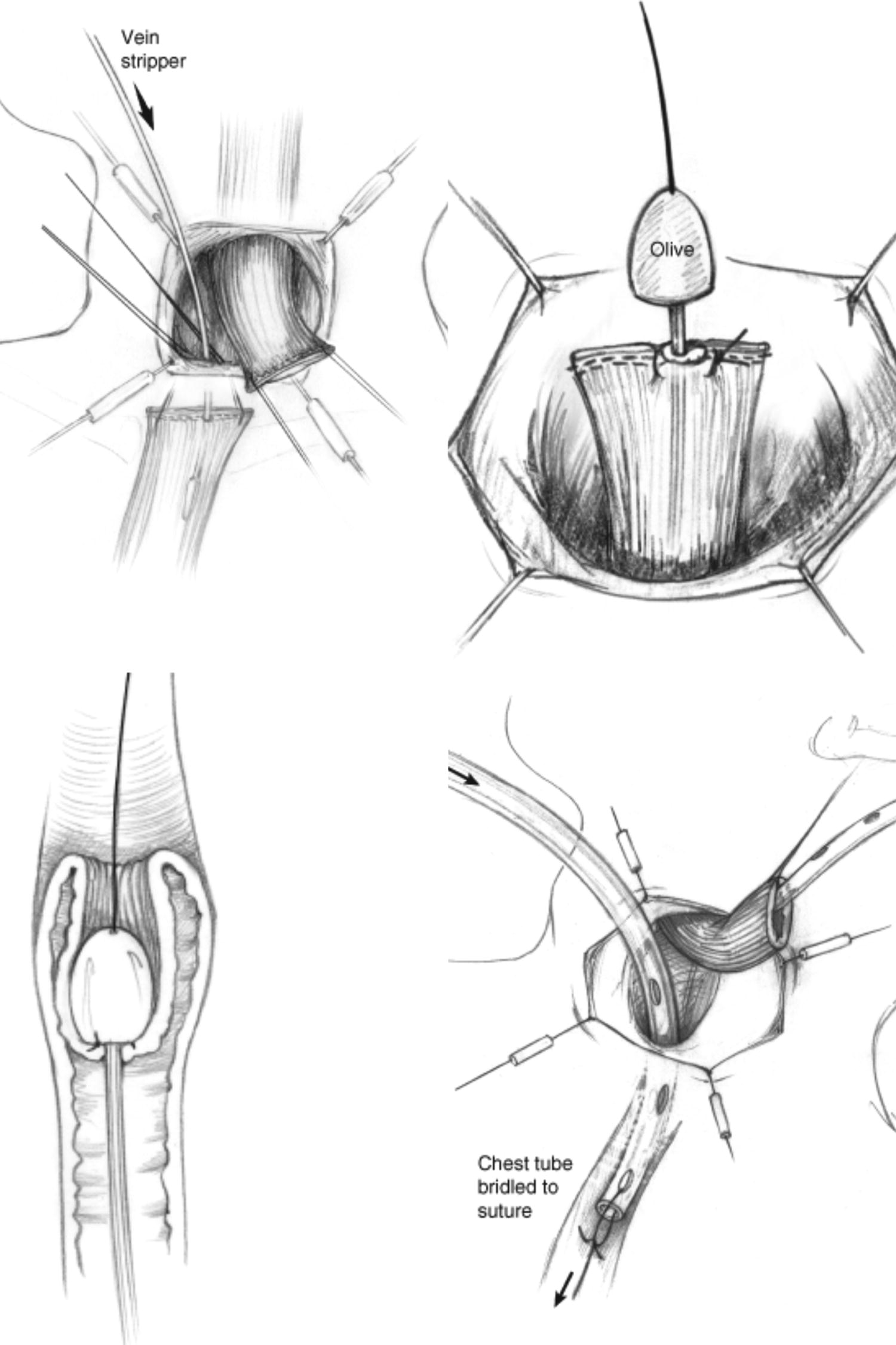
Antegrade inversion technique at cervical part (Reproduced from “Atlas of Minimally Invasive Surgical Operations” with permission from Corinne Sandone, CMI, FAMI, © 2018 JHU AAM; Department of Art as Applied to Medicine; The Johns Hopkins University School of Medicine.).
A 60-French bougie dilator is connected to the cervical incision and the neck surgeon inserts it into the posterior mediastinum, while pulling the silk suture downward to widen the thoracic inlet. The bougie dilator is then withdrawn to the neck and the long silk suture is moved from the bougie dilator to connect with the chest tube. A clamp is placed at the cervical end of the chest tube to prevent leakage of pneumoperitoneum. The neck surgeon inserts the chest tube into the posterior mediastinum while simultaneously pulling down the silk suture from the abdominal side (Fig. 6). Once the chest tube becomes visible below the hiatus, the silk suture is cut off. In the abdomen, the upper part of the conduit is sewn to the chest tube using two 0-braided permanent sutures. The gastric conduit is laparoscopically guided through the hiatus in the correct orientation.
Antegrade inversion technique at abdominal part. (Reproduced from “Atlas of Minimally Invasive Surgical Operations” with permission from Corinne Sandone, CMI, FAMI, © 2018 JHU AAM; Department of Art as Applied to Medicine; The Johns Hopkins University School of Medicine.).
Cervical anastomosis
The esophagogastric anastomosis is created using a side-to-side partially stapling technique. The staple line is positioned to the right of the esophagus and any excess or compromised tissue is removed (Fig. 7). Lembert sutures are placed, inverting the proximal conduit staple line. A silk stay suture is placed on the inferior anterior aspect of the conduit, followed by a 1.5-cm gastrotomy. A 45-mm linear endostapler is carefully inserted cephalad into both the esophagus and the conduit, avoiding the nasogastric tube. The nasogastric tube is then passed through the newly formed anastomosis and positioned distally within the gastric conduit. The common esophagogastrostomy is closed with two running 3–0 absorbable monofilament sutures and 2–0 silk Lembert stitches. Finally, the anastomosis is carefully positioned within the posterior mediastinum and a 10-French Jackson–Pratt drain is placed in the neck to drain any fluids. The patient’s neck is then returned from the extended position and the platysma muscle is reapproximated with a continuous absorbable suture.

Creation of cervical esophagogastric anastomosis. (Reproduced from “Atlas of Minimally Invasive Surgical Operations” with permission from Corinne Sandone, CMI, FAMI, © 2018 JHU AAM; Department of Art as Applied to Medicine; The Johns Hopkins University School of Medicine.).
Pyloromyotomy and jejunostomy (optional)
While the neck surgeon performs the anastomosis, a laparoscopic surgeon may concurrently perform a pyloromyotomy and jejunostomy. The pylorus is identified and sutures are placed across the muscle. The serosa is scored with an “L” hook electrocautery device, dividing the muscle fibers of the pylorus. If a mucosotomy occurs, the pyloromyotomy may be converted to pyloroplasty. The patient is positioned for jejunostomy, which is performed with absorbable enteropexy sutures in a diamond pattern. The patient is placed back in the steep reverse Trendelenburg position after this step. A methylene blue leak test is performed through the nasogastric tube testing the cervical anastomosis as above as well as the pyloromyotomy/plasty simultaneously. The anastomosis is positioned permanently in the posterior mediastinum and any redundant laxity is pulled through the hiatus. After this, the conduit is then securely attached to the hiatus with interrupted, single-pledgeted (on the hiatus) braided permanent sutures. The left upper quadrant port site is closed with a running absorbable monofilament sutured fascial closure.
Statistical analysis
All statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 29.0 (IBM Corp., Armonk, NY, USA). Parametric continuous data were expressed as mean with standard deviation (SD), nonparametric continuous data and categorical data as median with interquartile range and percentages, respectively.
Results
There were 38 patients with esophageal cancer included. Detailed demographic and clinical data are presented in Table 1. The average age of the patients was 67.2 years. Most were male (92.1%), White (97.4%), and classified as ASA Class 3 (86.8%). A history of smoking was present in 60.6%. Comorbidities, excluding hypertension, were identified in 10.5%–23.7% of patients. Stage 1 was the most frequent diagnosis (68.4%). Neoadjuvant chemoradiotherapy was administered to only five patients (13.2%).
Demographic Characteristics
As demonstrated in Table 2, the predominant histological subtype of esophageal carcinoma observed in this study was adenocarcinoma, identified in 97.4% of patients. The majority of tumors were located within the lower third of the esophagus, accounting for 22 cases (57.9%). The pathological stage distribution revealed that 55.2% of patients were diagnosed with stage 1, followed by 31.6% with stage 0, and 13.2% with stage 2. Lymph node metastasis was absent in 86.8% of patients. The most prevalent histological grade observed was moderately differentiated. All patients achieved negative resection margins. However, only one patient among those who underwent neoadjuvant chemoradiotherapy exhibited a pathological complete response.
Tumor Characteristics and Histopathological Findings
Detailed findings regarding the perioperative outcome and postoperative course are presented in Table 3. The median operative time was 375 minutes. The median hospital stay was 8 days, with a median of 3 days in the intensive care unit (ICU). Postoperative respiratory complications were observed including pneumonia occurring in three patients (7.9%), pleural effusion in 22 patients (57.9%), and pneumothorax in 12 patients (31.6%). Anastomotic leak occurred in five patients (13.2%), while surgical site infection was observed in six patients (15.8%). Vocal cord dysfunction was identified in two patients (5.3%). Conduit necrosis occurred in only one patient (2.6%) and necessitated reoperation. Readmission within 6 months after surgery was required for eight patients (21.1%). No mortality was reported in this patient cohort.
Operative Details and Outcomes
ICU, intensive care unit; IQR, interquartile range.
Discussion
Currently, the transthoracic approach dominates 80% of esophagectomy procedures; however, the transhiatal approach remains a viable alternative offering distinct advantages for select patients. 23 THE may be opted for when a two- or three-field TTE is deemed unnecessary, when extensive lymphadenectomy is not warranted, although this is debated. 24 Esophagectomy without lymphadenectomy is appropriate for high-grade dysplasia and T1a esophageal cancer not amenable to successful endoscopic resection. While occasionally used for T1b esophageal cancer, THE should be carefully considered due to its higher chance of lymph node metastases, ranging from 20% to 37%.10,24–26 Notably, tumors located in the middle thoracic area may pose risks during blind dissection in THE.27,28 In addition, THE could serve as an alternative surgical option for patients with poor performance status, for whom thoracotomy or single lung ventilation carries significant risks. 10 The choice between THE and TTE should be tailored to individual patient and tumor characteristics.
A key randomized controlled trial by Hulscher et al. (2002) demonstrated comparable median DFS between TTE and THE, serving as a cornerstone for comparing the effectiveness of both method. 29 Further, THE offered significant advantages in terms of operative duration, intraoperative blood loss, pulmonary complications, and chylous leakage. Notably, long-term survival analysis revealed no difference in 5-year overall survival (OS) between the two approaches, 7 similar to the meta-analysis encompassing over 5905 patients reported by Boshier et al. 8 Despite the established value of trimodality therapy for esophageal cancer, well-designed randomized controlled trials are required to compare the outcomes of THE and TTE in patients receiving chemoradiation. This would provide valuable evidence to guide optimal surgical decision-making in this evolving treatment landscape.
In recent decades, a much needed paradigm shift has occurred in esophageal cancer surgery, with a growing emphasis on MI approaches. While thoracoscopic techniques have rapidly supplanted open thoracotomy, the integration of MI techniques into the transhiatal approach has seen a more gradual adoption since its initial description in 1995. 22 The current evidence on MI-THE is limited, primarily consisting of retrospective cohort studies, which do not provide definitive conclusions regarding the outcomes compared to O-THE.30–32 However, the available data suggest potential advantages of the MI approach. Several studies have demonstrated that MI-THE can lead to lower morbidity, shorter hospital stays, and decreased intraoperative blood loss compared to O-THE.30,32 This may be attributed to the enhanced visualization and magnification provided by the laparoscopic approach, which facilitates more precise dissection and lymph node retrieval in the lower mediastinum without the need for blind dissection. 33 The MI technique also avoids the morbidity associated with thoracotomy incisions required for TTE.
Importantly, there is a study demonstrating no significant differences in long-term oncological outcomes, such as OS, between O-THE and MI-THE. 34 This suggests that the MI approach can achieve comparable oncological outcomes. Nonetheless, that study reported higher rates of specific complications, such as anastomotic leaks and chylous leaks, with MI-THE compared with O-THE. 34 This may be related to the technical challenges inherent in performing a complex esophageal reconstruction through a MI approach. The learning curve associated with mastering the MI-THE technique could also contribute to these findings. It is imperative to meticulously adhere to the critical surgical steps to carry out a safe operation. However, data analyzing the details of surgical steps used in MI-THE are lacking.
This retrospective study meticulously describes our surgical technique for performing MI-THE and evaluates the perioperative outcomes of this technique in 38 patients with esophageal cancer. Most patients (86.8%) were diagnosed with early-stage esophageal cancer (stage 0 or 1). Our findings show favorable perioperative outcomes. The median operative time (375 minutes), hospital stay (8 days), and ICU stays (3 days) are comparable to previously reported data for MI-THE.35–37 All achieved negative surgical margins. The most frequent complication was pleural effusion (57.9%), then pneumothorax (31.6%), and surgical site infection (15.8%). The anastomotic leak rate (13.2%) is comparable with other studies on MI-THE.38–40 There was no mortality within 90 days of surgery. This study suggests that MI-THE is a feasible and safe approach for esophageal cancer resection, with encouraging results in terms of morbidity and mortality. Notably, there were no instances of postoperative mortality, and patients experienced short hospital stays and ICU stays.
The limitations in this study include its retrospective design and the relatively small sample size. The authors favor MI-THE for early-stage cancer not resectable by endoscopically; hence, there were a low number of patients receiving neoadjuvant chemoradiotherapy which limits the generalizability of oncological outcomes in this study. The paucity of high-quality comparative studies, such as randomized controlled trials, highlights the need for further research to definitively establish the potential benefits of MI-THE over O-THE. Larger, well-designed studies are necessary to provide robust evidence on the short-term and long-term outcomes, including oncological, functional, and quality of life measures. In addition, studies evaluating the learning curve and the impact of surgeon experience on the outcomes of MI-THE would be valuable.
Conclusions
MI-THE appears to be a safe and feasible approach for esophageal cancer resection, with promising results and the potential to improve perioperative outcome and decrease morbidity. MI-THE offers select advantages for early-stage cancer and high-risk patients. As existing data are limited, further research is needed to fully elucidate the role of MI-THE in esophageal cancer management.
Footnotes
Acknowledgments
The authors would like to thank Corinne Sandone and the Department of Art as Applied to Medicine at Johns Hopkins University School of Medicine for granting permission to use the images from “Atlas of MI Surgical Operations.”
Authors’ Contributions
Collected data, conducted data analysis, performed a literature review, and wrote the article: T.C. Edited and reviewed article: A.Q. Edited and reviewed article: J.H. Made substantial contributions to the conception and design of the study and edited article: S.W.
Availability of Data and Materials
Research data are stored in an institutional repository and will be shared upon request with the corresponding author.
Ethical Approval and Consent to Participate
This study was approved by the institutional review board committee at the University (IRB No.1759). The informed consent was waived due to its retrospective study type.
Disclosure Statement
All authors declared that there are no conflicts of interest.
Funding Information
No funding was received for this article.