
Abstract
Introduction:
To assess the medium-term weight loss and maintenance of lean body mass (ideal weight/weight loss maintenance) following the Roux-en-Y gastric bypass (RYGB) surgical procedure with or without the use of a rigid gastric ring.
Method:
An observational cohort study with a retrospective approach was conducted to evaluate the effectiveness of RYGB with and without a band in patients with morbid obesity. The outcomes were assessed by analyzing data obtained from medical records, including pre- and postoperative data.
Results:
A total of 239 patients who underwent surgery between 2001 and 2018 were included, with 150 undergoing RYGB without a ring and 89 using a ring. The group subjected to the intervention with a rigid ring showed a significantly higher average body mass index loss than the ringless group (coefficient −2.45; 95% confidence interval [CI]: [−3.92 to −0.97], P < .001) at 1 year. After a follow-up period of 5 years, the use of a gastric ring was still associated with significant improvement in weight loss, even after multivariate adjustment (coefficient 6.62, 95% CI: [+ 4.30 ± 8.95], P < .001). Less than 5% of patients needed gastric band removal during the follow-up period.
Conclusion:
In this retrospective cohort of 239 patients, using a ring in RYGB was associated with a significant increase in weight loss and maintenance of lean body mass.
Introduction
Obesity is a complex disease that leads to changes in body structure, resulting in several comorbidities. Over the years, it has become a significant problem, with health system expenditures exceeding U.S. $654 million in 2019 in Brazil. 1 Obesity contributes to other diseases such as type 2 diabetes mellitus (DM2), systemic arterial hypertension (SAH), sleep apnea, asthma, coronary heart disease, stroke, and cancer.2–5
The World Health Organization (WHO) defines obesity based on anthropometric data, particularly the body mass index (BMI), calculated as the ratio of body mass in kilograms to height in square meters. 6 Individuals are classified as normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), obesity grade I (30–34.9 kg/m2), obesity grade II (35–39.9 kg/m2), and obesity grade III (above 40 kg/m2). 6 The WHO emphasizes that obesity is a multifactorial disease requiring comprehensive treatment approaches to address the associated risks and complications. 6
Treating obesity requires multifaceted approaches such as dietary changes, physical activity, and management of comorbidities. However, maintaining long-term weight loss can be challenging.7,8 Clinical and drug treatments are often the first line of therapy, but due to costs, poor adherence, and limited multidisciplinary follow-up, these approaches may not yield long-term success.9–11 Bariatric surgery has emerged as a viable option for weight reduction and long-term lean body mass maintenance.12–14
Bariatric surgery has demonstrated excellent results in achieving weight loss and improving comorbidities, particularly in patients with obesity. One of the most widely used procedures is the Roux-en-Y gastric bypass (RYGB), which offers significant benefits in terms of weight reduction and metabolic improvements. 15 Given the prevalence of obesity and the challenges associated with long-term weight management, it is essential to explore different surgical techniques and their long-term outcomes. This study aims to compare the efficacy of RYGB with and without the use of a rigid gastric ring in patients undergoing bariatric surgery.
Materials and Methods
Study design
This is a retrospective observational study with a prospective cohort. The checklist for STROBE cohort studies was used as a methodological framework for writing this research report. 16
Study location
The study was carried out in a private outpatient clinic of Bariatric and Digestive System Surgery in the city of São Paulo, which serves the population by spontaneous demand in the private modality and via complementary health medical plans.
Patients with an indication for bariatric surgery are seen in person by the multidisciplinary team in the areas of surgery, nutrition, and psychology during the pre and postoperative process, in the immediate postoperative period (up to 7 days after surgery), and late (after 7 days since surgery, 1 year, and up to 5 years of follow-up).
Surgical interventions and possible hospitalizations during treatment and in the postoperative period of bariatric surgery are performed in several hospitals in São Paulo.
Casuistry
Adult patients underwent bariatric surgery from 2001 to 2018, totaling 239 eligible patients: 150 who underwent RYGB without using a ring and 89 who underwent RYGB with a ring. Of these, 61 patients were female (68.53%), and the median age observed was 36 years (interquartile range [IQR]: 29–44.5). In the ringless RYGB group, 90 women (60%) had a median age of 36.57 years (IQR: 31–44).
Inclusion and exclusion criteria
From the population studied, a convenience sample was selected according to the following criteria: age over 18 and under 65 years old; diagnosis of class III obesity, with or without comorbidities and/or grade II with comorbidities; and have undergone gastric bypass in the Roux-en-Y modality by videolaparoscopy with or without a ring. The exclusion criteria were the absence of data on pre- and postoperative outcomes, patients undergoing other concurrent procedures, and revisional bariatric surgery.
Data collection
In the initial stage of the study, the electronic medical records of patients who underwent surgical interventions during the designated period and who met the inclusion criteria were thoroughly examined, and thus, spreadsheets of the number of patients involved in the study, gender, age, comorbidities, height, weight, and the entire postoperative process were created. Immediate postoperative complications were strictly defined as bleeding, fistula, obstruction, reapproach, and deaths occurring within the first 7 days after the surgical procedure. In addition, late complications were strictly defined as weight regain, malnutrition, conversion from surgery, reintervention after the initial procedure, cholelithiasis, and postoperative deaths (30 days). Data collection instruments were a sociodemographic and clinical data form and a postoperative clinical and surgical outcome form.
Data analysis
In the present study, the data were tabulated in an Excel(R) spreadsheet (Microsoft 365(R), 2019) and statistically analyzed, applying the STATA software, standard edition, version 18. For the descriptive analysis, absolute quantities, measures of central tendency (mean and median), and distribution (minimum, maximum, and percentage) were used using the Student’s t-test.
Differences in means were obtained for the analysis of the primary outcome. Adjusted coefficients were obtained (corrected for age, sex, hypertension, DM2, liver disease, presence of neoplasia, heart failure, smoking, and peripheral vascular disease) using linear regression. A statistical significance level of 5% was considered.
Ethical aspects
The ethical requirements recommended by Resolution 466/12 of the National Health Council of Brazil were respected. The project was approved by the Research Ethics Committee of the University of São Leopoldo Mandic and approved by Plataforma Brasil under number 66632722.2.0000.5374.
Surgical technique
The patients were submitted to general anesthesia, positioned in the supine position in the semi-lithotomy position, with the surgeon positioned between the legs. Five trocars were placed: one of 10 mm for optics, 5 cm above and to the left of the umbilical scar; another 12 mm trocar on the left hemiclavicular line 2 cm below the left rib cage; another 12 mm trocar on the right hemiclavicular line 5 cm below the right rib cage; 1 × 5 mm trocar parallel to the optical portal at a distance of 10 cm from it on the left flank; and finally, the fifth trocar at the level of the xiphoid appendix for placement of the liver retractor.
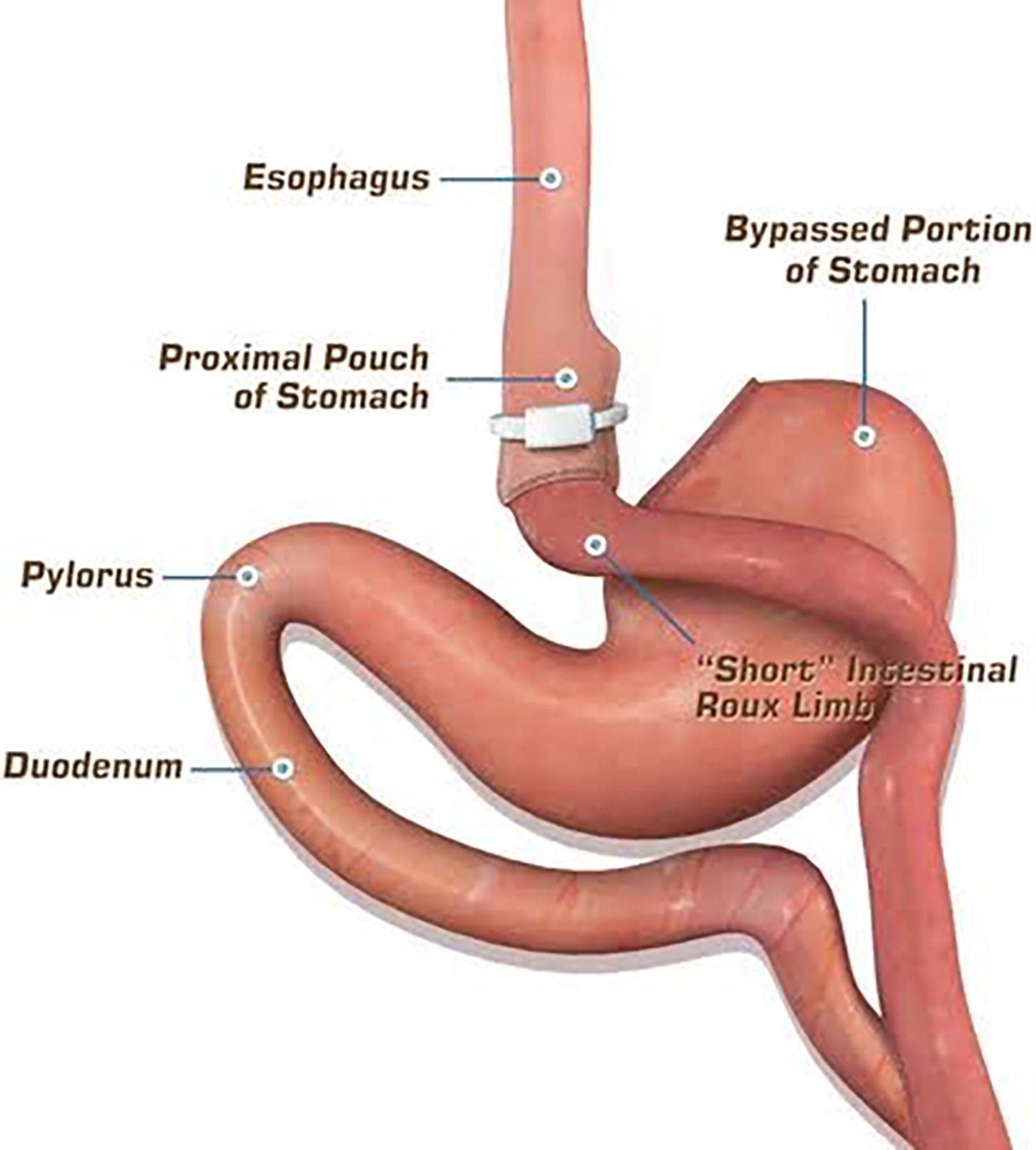
The first step involves dissection of the esophagogastric angle, exposing the left arm of the left diaphragmatic abutment. A Fouchet probe is inserted orally to shape the gastric pouch and gastrojejunal anastomosis. A hole is made in the epiploon in the smaller perigastric curvature, about 5–7 cm from the esophagogastric transition. The stomach is sectioned horizontally using a laparoscopic linear stapler in a section of about 4 cm. A vertical section of the stomach is performed parallel to the minor curve toward the angle of Hiss molded under a 32 Fr Fouchet probe. The infra-mesocolic gait is passed, identifying Treitz’s angle, and isolating the biliary loop and is about 80 cm long. The transition between the alimentary and bile loops is demarcated at this level. The set is elevated to the supramesocolic floor in precolic and pregastric situations, and gastrojejunal anastomosis is performed by inserting a laparoscopic linear stapler at the distal point of the gastric pouch and into the jejunal loop. The enterostomy is closed with extramucosal suture with PDS 3-0 thread. Next, the 120-cm food segment is measured, which is anastomosed to the bile loop with a laparoscopic linear stapler. The stapler’s gap is closed with extramucosal suture with PDS 3-0 thread. The anastomosis integrity test is then performed with methylene blue solution. The mesenteric gap is closed with continuous 3-0 Ethibond® suture. When a containment ring is used, a band with a circumference of 6.2 cm, providing a diameter of 1.5 cm, is placed approximately 2 cm above the gastrojejunal anastomosis (Figure 1).
The bile loop is separated from the feeding loop with a laparoscopic linear stapler. The abdominal cavity is drained. When a retainer ring is used, a ring with a circumference of 6.2 cm is passed, which gives a diameter of 1.5, about 2 cm above the gastrojejunal anastomosis. This time is always performed after the preparation of the gastrojejunal anastomosis, and the ring is fixed with a 2-0 cotton stitch. 23
Results
In all, 239 patients were included for analysis, 150 underwent ringless RYGB, and 89 underwent ring-bearing RYGB (Table 1).
Clinical Characteristics Comparison
BMI, body mass index; IQR, interquartile range; RYGB, Roux-en-Y gastric bypass.
In the banded RYGB group, there were 26 patients with SAH (29.21%) and 14 patients with diabetes (15.73%). The median baseline BMI was 45.66 (IQR: 41.25–48.87). Of these, 61 patients were female (68.53%), and the median age observed was 36 years (IQR: 29–44.5).
In the ringless RYGB group, there were 90 women (60%), 43 patients with SAH (28.66%), 27 patients with diabetes (18%), and a median age of 36.57 (IQR: 31–44). The median baseline BMI was 40.86 (IQR: 38.04–43.56).
Weight loss in 1 year
After a 12-month postoperative follow-up, BMI was measured in both groups. The median loss of BMI points in the group without a ring was 14.15 (IQR: 13.44–14.85). Meanwhile, the median loss of BMI points in the ring group was 16.6 (IQR: 15.03–18.16). The difference in mean BMI loss between the groups was significant, with a P value of .0013.
After multivariate analysis adjusted for possible confounding factors, ring use was also associated with significantly greater weight loss (coefficient +2.44, 95% CI: [3.92–.97], P < .001) (Table 2).
BMI Loss Comparison
BMI, body mass index; CI, confidence interval; RYGB, Roux-en-Y gastric bypass.
Weight loss in 5 years
After a 60-month postoperative follow-up, the median loss of BMI points in the group without a ring was 12.43 (IQR: 8.33–15.14), while in the group with a gastric ring, the median loss of BMI points was 17.26 (IQR: 13.85–21.77). After multivariate analysis by linear regression, the use of a ring was associated with a significant increase in the loss of BMI points (coefficient 6.62, 95% CI: [+4.30 ± 8.95], P < .001) (Table 3).
Median BMI Loss Comparison
BMI, body mass index; CI, confidence interval; IQR, interquartile range; RYGB, Roux-en-Y gastric bypass.
Immediate postoperative complications
Three patients had complications in the immediate postoperative period, two in the group without a ring and one in the group with a ring. In the ring group, one case of hypertension was recorded with the need for follow-up of the patient in the intensive care unit. In the ringless group, one patient had gastrointestinal bleeding requiring reoperation, and one patient had staple line bleeding corrected with endoscopic therapy. There was no significant difference between immediate postoperative complications between the two groups (RR: 0.85, 95% CI: [0.08–9.22], P = .892).
Late postoperative complications
Late postoperative complications were observed in 20 patients in the ringless bypass group (13.33%) and in 13 patients in the ring group (14.60%). The most common postoperative complication in both groups was cholelithiasis—in 11 patients without a ring and 10 patients with a ring. Other complications observed included anastomotic stenosis (two patients without ring), malnutrition requiring ring removal in one patient, gastric fistula in two patients in each group, one marginal ulcer in the ring group, and one internal hernia in each group. After multivariate analysis, there was no significant difference in the incidence of complications between the groups (RR: 1.10, 95% CI: [0.56–2.08], P = .810).
Gastric ring removal
During the follow-up period of the patients, five cases (5.6%) were observed in which there was a need for ring removal due to dysphagic conditions and/or migration. In none of the cases of band migration was an intestinal resection required during surgical interventions. The procedures performed to address the complications arising from migration consisted exclusively of band removal, without repositioning the device. Patients who underwent band removal showed no clinical evidence of weight regain following the procedure.
Discussion
In this retrospective cohort, using a gastric ring was associated with more significant weight loss, both in the short and long term, without an increase in postoperative complications.
Recent studies such as Dimou et al. (2022) and Tsai et al. (2021) have shown that including a gastric ring in RYGB procedures enhances the restrictive aspect of the surgery. By maintaining the size of the gastric pouch, the ring limits the stomach’s capacity, contributing to long-term weight loss. Dimou et al. observed a greater reduction in BMI at the 5-year follow-up for patients who received a gastric ring, further supporting the efficacy of this intervention. 17 These findings align with our study, where patients with a gastric ring showed a significantly higher loss of BMI points after 5 years. This emphasizes the mechanical role that the ring plays in controlling weight regain. The long-term effectiveness of the gastric ring is further supported by studies that suggest that without a ring, the diameter of the anastomosis may increase over time, leading to faster gastric emptying and, consequently, diminished weight loss. 18
In a study by Skidmore and Holt (2022), patients who received a gastric ring experienced a 15% greater average weight loss than ringless patients. The use of a ring was associated with better short-term outcomes and a higher rate of sustained weight loss over 3–5 years. This supports the findings in our cohort, where ringed patients maintained superior weight loss even in long-term follow-up. 19 The restrictive effect of the ring appears to contribute to both the immediate and sustained weight loss observed in our study, further validating its inclusion in bariatric procedures. This is particularly important for patients who struggle with weight regain after non-banded procedures. The enhanced restrictive properties of the ring may prevent the stomach from expanding, ensuring long-term efficacy in maintaining weight reduction.
In our study, the average BMI reduction in the ring group exceeded that in the nonring group by five points after 5 years. Valezi et al. (2008) observed similar results in their study of the effectiveness of gastric rings in controlling weight regain. The authors suggest that the long-term benefits of the ring are due to its mechanical influence on reducing the size of the anastomosis, which prevents the stomach from expanding postoperatively. 20 Our results mirror those of Valezi et al., with patients in the ring group showing sustained weight loss over a long period. This reinforces the importance of the ring in controlling postoperative weight gain, a major challenge for many patients undergoing bariatric surgery.
Regarding postoperative complications, our findings indicate that the incidence of complications was low in both the ring and nonring groups. This aligns with research by Tsai et al. (2022), who found that complication rates, including ring migration and dysphagia, were minimal and occurred in less than 5% of patients. 18 Similarly, our study found that less than 5% of patients in the ring group required band removal, and the overall complication rate was comparable between both groups. These results support the safety profile of the gastric ring in the long-term management of bariatric patients. Furthermore, the consistency of these findings with other studies indicates that the risk associated with using the ring is relatively low, particularly when compared to the long-term benefits of weight maintenance.
Our study further reinforces the safety of gastric rings in bariatric surgery. The study by van Dam et al. (2023) showed no significant increase in immediate or late postoperative complications with using rings. This supports the conclusion that rings are a safe addition to RYGB when properly managed. 21 Despite concerns over potential complications such as ring migration or stenosis, our findings confirm that these risks remain minimal, especially when proper surgical techniques are employed. The results of this study, in conjunction with other similar findings, suggest that rings can be safely integrated into bariatric procedures without a significant increase in the risk of complications.
Cholelithiasis was the most common complication observed in our study, a finding consistent with global trends in bariatric surgery. For instance, in a study by MacLean et al. (1993), cholelithiasis was identified as a common postoperative complication in bariatric surgery, with incidence rates reaching 20% in long-term follow-ups. This aligns with our findings of similar incidence rates between the ring and nonring groups. 14 Cholelithiasis remains a well-documented complication in bariatric surgery, and its occurrence in both groups indicates that it is not necessarily linked to the presence of a gastric ring. Rather, it appears to be a general risk associated with rapid weight loss post-surgery.
Our study adds to a growing body of evidence that gastric rings provide additional benefits in RYGB, especially in terms of weight loss maintenance. Recent studies by Tsai et al. (2021) and Skidmore et al. (2022) have corroborated the long-term advantages of using rings, suggesting that their continued use could be beneficial in select patient populations, especially those struggling with weight regain after nonringed procedures.18,19 The growing consensus in the literature supports the notion that the restrictive nature of the ring provides an effective mechanism for long-term weight control, particularly in patients prone to weight regain. Given the findings of our study, we recommend further research into the long-term benefits of gastric rings, particularly in diverse patient populations.
The decision to incorporate a band during an RYGB should be individualized, as the addition of a band can influence weight loss outcomes and complication rates. Studies have shown that banded RYGB may result in greater and more sustained weight loss compared to nonbanded RYGB. For instance, Goitein et al. reported that banded RYGB patients achieved a 5-year excess weight loss of approximately 72.5%, which was sustained at 10 years. However, the addition of a band is also associated with specific complications. The same review noted band-related reoperation rates of about 4.1%, with complications such as gastric outlet stenosis, band erosion, and band slippage. 22
In summary, while banded RYGB can enhance weight loss outcomes, it also introduces potential complications. The decision to use a band should be based on a comprehensive evaluation of individual patient factors and a thorough discussion of the potential benefits and risks.
Conclusion
This study demonstrates that the use of a rigid gastric ring in RYGB significantly enhances weight loss outcomes compared to the ringless procedure, both in the short (1 year) and long term (5 years). Including the ring offers a mechanical advantage by maintaining the size of the gastric pouch, which contributes to sustained weight reduction without increasing the incidence of postoperative complications. The low rates of complications such as ring migration or dysphagia further support the gastric ring’s safety profile, making it a viable adjunct for patients facing weight regain challenges. These findings underscore the potential for gastric rings to improve the long-term success of bariatric surgery, particularly in populations at higher risk for weight recidivism.
While this study provides promising results, further research is needed to confirm the long-term benefits of gastric rings beyond 5 years. Randomized controlled trials are necessary to eliminate potential biases and validate the superiority of ringed RYGB over the ringless procedure. Additionally, future studies should explore the long-term metabolic effects, quality of life improvements, and the durability of weight loss over periods of 10 or 20 years. Expanding research to include diverse patient populations, particularly those with severe obesity and comorbidities, will be critical to optimizing patient outcomes and refining the role of gastric rings in bariatric surgery.
Footnotes
Acknowledgments
The authors thank the administrative team at São Leopoldo Mandic, whose assistance made this research possible. The authors are also grateful to the patients who participated in this study.
Authors’ Contributions
The authors of this work contributed significantly to the development, research, and writing of this article. Their individual contributions are outlined as follows: A.C.A.C.: Conceptualization, methodology, data analysis, and article writing. R.M.d.A.L.: Literature review, data collection, and article editing. W.P.S.: Statistical analysis, results interpretation, and final article review. D.d.M.: Supervision, funding acquisition, and project administration. B.Z.: Supervision, funding acquisition, and project administration. All authors have read and approved the final version of the article and agree to be accountable for all aspects of the work to ensure its accuracy and integrity.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This work was funded by the authors themselves.