
Abstract
Background:
The concept of preoperative prehabilitation has garnered attention as a means to manage the comorbidities of patients undergoing ventral hernia repair (VHR). In this regard, some comorbidities have been studied as potential risk factors for postoperative complications following VHR, such as diabetes, immunosuppression, and smoking. However, evidence regarding the impact of sarcopenia, defined by reduced muscle mass and highly associated with frailty syndrome, remains a gap. We aimed to perform a systematic review and meta-analysis analyzing the impact of sarcopenia on VHR outcomes.
Methods:
Cochrane Central, Embase, PubMed, MEDLINE, and Web of Science were searched for studies analyzing the impact of sarcopenia on VHR from inception until April 2024. Outcomes assessed were recurrence, surgical site occurrences (SSO), surgical site infection (SSI), and hospital length of stay (LOS). Data analysis was done using RStudio 4.1.2 Software.
Results:
The initial search yielded 263 results, of which 172 were screened after the exclusion of the duplicates. The full-text review was done for eight studies, of which three were included after applying the eligibility criteria. Our sample comprised 275 patients, of which 79 (28,7%) presented with sarcopenia. All included studies used radiological muscle findings to define sarcopenia. Our analysis showed no differences in recurrence rates between patients with sarcopenia and controls (risk ratios [RR]: 1.24; 95% confidence interval [CI]: 0.79–1.94; P = .35). Furthermore, no differences were found in SSI (RR: 0.7; 95% CI: 0.39–1.25.; P = .23). Interestingly, a higher SSO rate was noted for patients without sarcopenia (95% CI: 0.35–0.96; P = .04). No differences were found in LOS (mean difference 4.7 hours; 95% CI: −0.67 to 10.1; P = .4).
Conclusion:
Our analysis showed no differences were found in recurrence, SSI, and LOS following VHR in patients with sarcopenia. Furthermore, there was a reduced SSO for patients with sarcopenia.
Introduction
Ventral hernias are common abdominal pathologies, with an incidence of up to 20% 1 and can exceed 40% when analyzing incisional hernias following abdominal procedures.2,3 Many risk factors for poor outcomes after ventral hernia repair (VHR) have been investigated. These factors include diabetes mellitus (DM), older age, higher body mass index (BMI), neoplasia and consumptive syndrome, liver and pulmonary disease, and immunosuppression.4–7
In this context, sarcopenia is a comorbidity defined as the reduction of muscle mass, which can be associated not only with advanced age but also with comorbidities such as advanced cancer and liver disease, DM, and even obesity with the infiltration of muscle tissue by adipose tissue.8–10 Previously diagnosed clinically in the advanced stages of consumptive diseases, sarcopenia has, in recent decades, become a comorbidity diagnosed through imaging in the preoperative period, typically via computerized tomography (CT) scan, with the assessment of muscle mass. 11
Therefore, it is crucial to identify the patient’s risk factors, including the presence of sarcopenia, to determine the optimal risk-benefit ratio of the surgical intervention, as well as the need for preoperative prehabilitation. 12 Previous reviews on the impact of sarcopenia on surgical outcomes have shown higher mortality and up to three times more postoperative complications in patients with sarcopenia.13,14 However, these studies mostly included patients undergoing surgeries for neoplasms, colorectal diseases, or trauma surgery, and the literature is still conflicting regarding the impact of sarcopenia on VHR outcomes. Thus, we conducted a systematic review and meta-analysis to compare the postoperative outcomes of patients with and without sarcopenia in VHR.
Methods
This meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses statement and recommendations from the Cochrane Collaboration Handbook for Systematic Reviews of Interventions. 15 We prospectively registered our research protocol in the International Prospective Register of Systematic Reviews on July 7, 2024 (ID CRD42024562859).
Eligibility criteria
Our PICO strategy was: (P) patients undergoing VHR, (I) patients with a diagnosis of sarcopenia, (C) patients without sarcopenia, and (O) recurrence and surgical site-related complications. We included in this meta-analysis studies that met all the following eligibility criteria: observational studies, comparing patients older than 18 years old with sarcopenia, with patients without sarcopenia, and undergoing VHR. As for sarcopenia definition, we considered a muscle index cutoff of <52.4 cm2/m2 for men and <38.5 cm2/m2 for women measured at the CT scan. 16 We excluded studies with no control group (including only patients with sarcopenia); different outcomes of interest; overlapping populations, defined as studies recruiting from the same institution over an overlapping period; systematic reviews, case reports, or conference abstracts.
Search strategy and data extraction
Two authors (C.A.B.S. and D.B.S.Z.-O.) independently and systematically searched PubMed, Embase, and Cochrane Library from inception to April 5, 2024. The following terms were used without filters, publication date, or language restrictions: (“Disuse atrophy” OR “muscle atrophy” OR sarcopenia) AND (ventral OR incisional OR umbilical OR epigastric OR lateral OR paraumbilical OR periumbilical OR midline) AND hernia. We included in our search strategy all mesh-related terms derived from our original search strategy.
The references from all included studies, and previous systematic reviews were also searched manually for any additional studies. Eventual conflicts were resolved by consensus among the authors. Two authors (C.A.B.S. and D.B.S.Z.-O.) independently extracted the following data from selected Randomized Controlled Trials: (1) country; (2) number of patients; (3) preoperative sarcopenia diagnostic tool; (4) VHR technique; and (5) hernia characteristics.
Endpoints
Our primary endpoints were recurrence and surgical site-related complications, including surgical site infection (SSI) and surgical site occurrences (SSO). SSO composes wound cellulitis, nonhealing incisional wounds, fascial disruption, skin or soft tissue ischemia, necrosis, serous or purulent wound drainage, stitch abscess, seroma, hematoma, infected or exposed mesh, or the development of an entero-cutaneous fistula as described by Haskins et al. 17 Recurrence analysis was performed with a minimum of 6-month follow-up postoperatively. As an additional outcome, we analyzed the hospital length of stay (LOS).
Quality assessment
We evaluated the risk of bias using version 2 of the Cochrane Risk of Bias in Non-Randomized Studies—of Interventions Tool (ROBINS-2), wherein each study is scored as critical, serious, some concerns, or low risk of bias. 18 The assessment was performed by two independent authors (C.A.B.S. and A.C.D.R.) and disagreements were resolved through consensus after discussing reasons for discrepancy.
Statistical analysis
We computed risk ratios (RR): using the Mantel–Haenszel test for dichotomous outcomes and used 95% confidence intervals (CIs) as a measure of effect size. We considered P-values of less than .05 to be statistically significant. We used mean differences (MD) as the effect measure for continuous outcomes, also with 95% CI.
To assess heterogeneity, Cochran’s Q test and I2 statistics were utilized. We classified I2 values of <25%, 25–75%, and >75% as representing low, moderate, and high heterogeneity, respectively. To account for potential disparities in both clinical and methodological aspects across studies, we applied the restricted maximum-likelihood estimator and random effects models for outcomes. Furthermore, we performed a funnel plot as needed to investigate heterogeneity between study-specific estimates. Our meta-analysis was conducted using the meta package for RStudio version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study selection and characteristics
The initial search yielded 263 results. After removing duplicate studies, 172 records were identified through database searching and their summaries were screened for eligibility. Of these, eight remained and were fully reviewed based on predefined eligibility criteria (Fig. 1). A total of three studies were ultimately included comprising 275 patients, of which 79 (28.7%) presented with a sarcopenia diagnosis preoperatively. All the studies were retrospective cohorts, of which two included all types of VHR, while one included only complex ventral hernias. Table 1 summarizes individual studies’ characteristics.
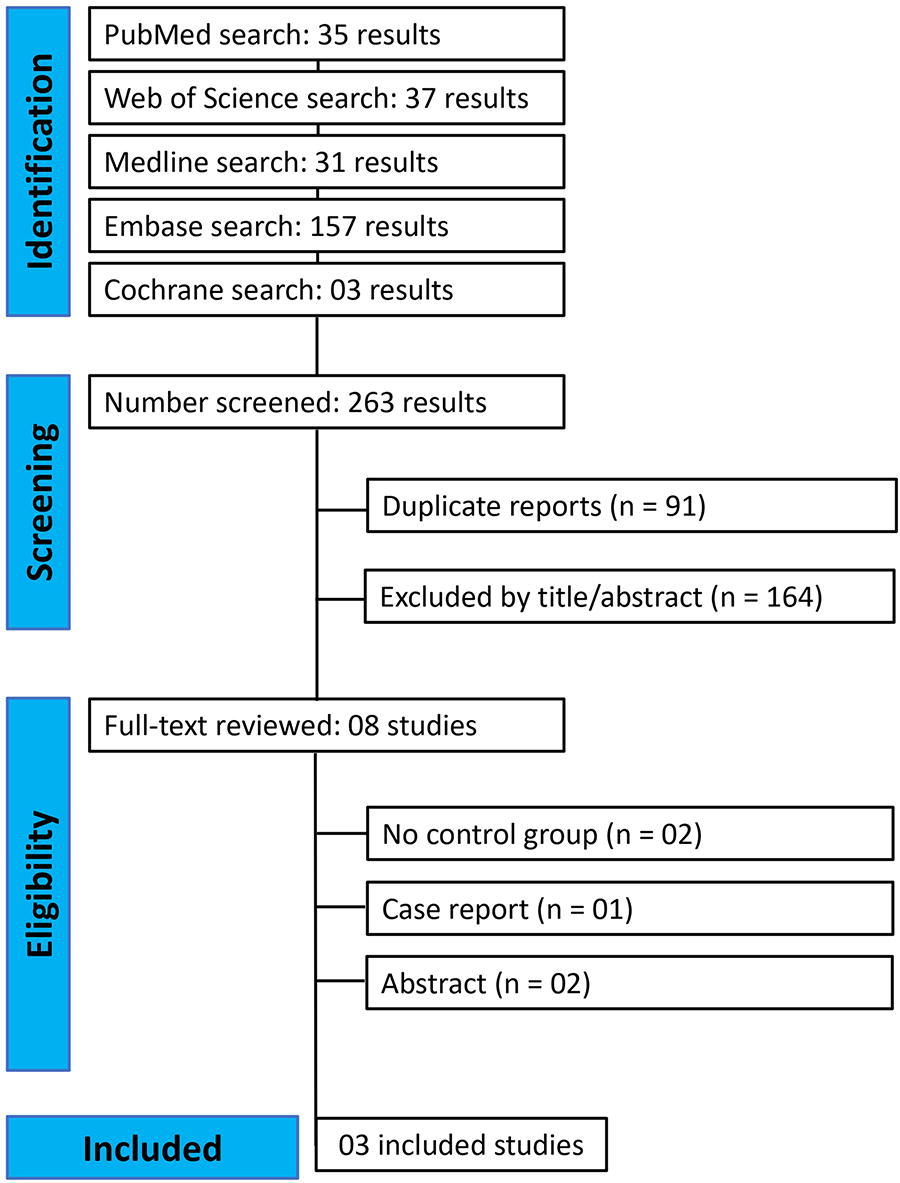
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flow diagram of study screening and selection.
Baseline Characteristics of the Studies Included
BMI, Body mass index; SD, Standard deviation; IQR, Interquartile range; N/A, Information unavailable.
Endpoints
In a pooled analysis of the three studies, no differences were found between patients with and without sarcopenia regarding recurrence rates (RR: 1.24; 95% CI: 0.79–1.94; P = .35; Fig. 2).
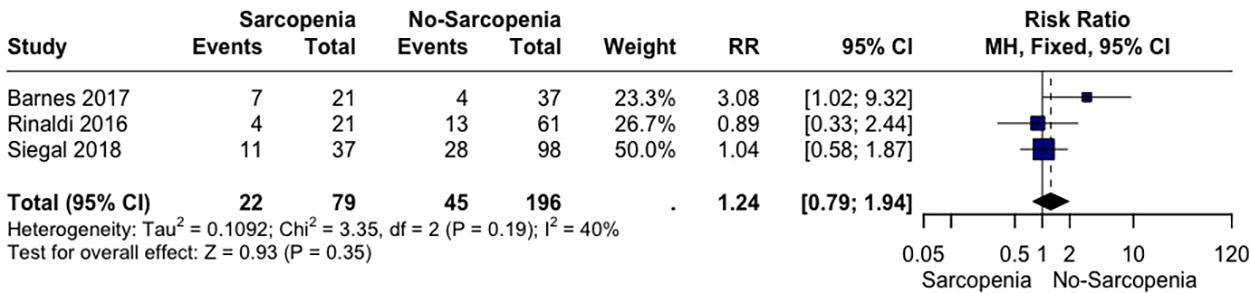
Forest plot of recurrence rates.
Also, no differences were found in SSI (RR: 0.7; 95% CI: 0.39–1.25; P = .23; Fig. 3). Interestingly, a higher SSO rate was noted for patients without sarcopenia (RR: 0.59; 95% CI: 0.36–0.96; P = .04; Fig. 4).

Forest plot of surgical site infection (SSI).

Forest plot of surgical site occurrences (SSO).
Furthermore, no differences were found in our additional outcome of LOS between patients with and without a preoperative diagnosis of sarcopenia (MD 4.7 hours; 95% CI: −0.67 to 10.1; P = .4; Fig. 5).

Forest plot of length of hospital stay.
Risk of bias
The overall risk of bias in nonrandomized studies ranged from low risk in two studies to moderate risk of bias in one study. Reasons for bias arousal were due to the confounding and selection of participants. Bias in those studies was raised mainly from its retrospective design, bias in the selection of surgical candidates, and relatively small sample, and in one of these studies, types of hernia repairs and types and location of mesh placement were not specified. The full risk of bias assessment is available in Figure 6.
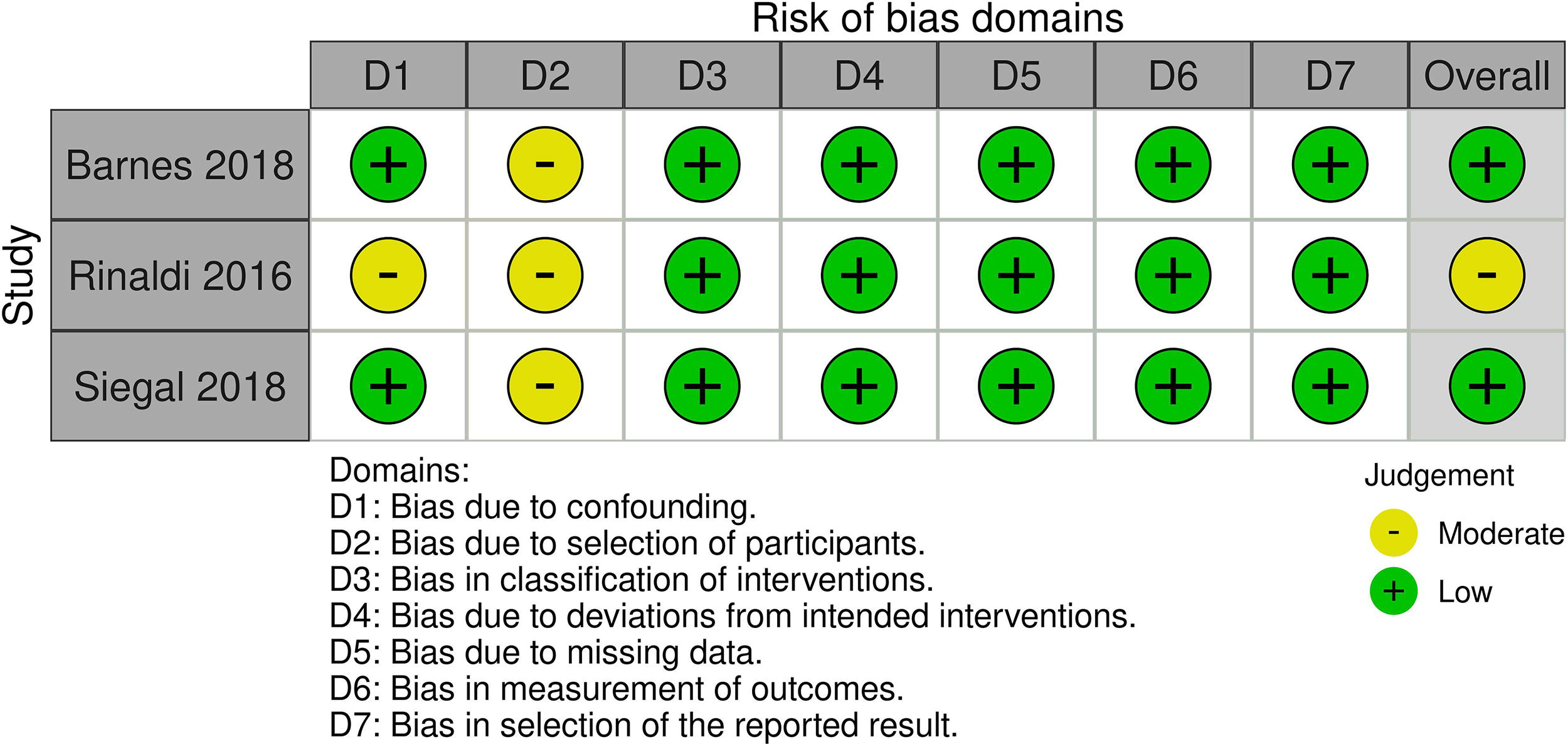
Risk of bias of the included studies (Risk of Bias in Non-Randomized Studies—of Interventions Tool [ROBINS-I]).
Discussion
In this systematic review and meta-analysis, we identified 275 patients from three studies analyzing the impact of a preoperative diagnosis of sarcopenia on VHR outcomes. We found no differences in recurrence, SSI, and LOS for patients with sarcopenia compared with patients without sarcopenia. However, patients with sarcopenia presented lower SSO compared with the control group.
Sarcopenia is associated with a reduction in lean muscle mass, with or without infiltration of the muscle by adipose tissue. 9 There are assumptions that this reduction in muscle mass could be linked to an increase in negative postoperative outcomes following VHR, particularly a higher recurrence rate. 19 This could be justified by the fact that many types of hernias are associated with collagen defects in their etiopathogenesis. 20 The reconstruction of the abdominal wall relies on the muscular structures for the closure of the defect in many types of hernia repairs. Therefore, the absence of sufficient musculature could lead to a weakened wall and subsequently an increased risk of recurrence.14,19
However, we did not find differences in recurrence rates for patients with sarcopenia compared with the control groups. Defects defined as complex VHR may have a higher tendency to fail in patients with sarcopenia since many of these defects require component separation techniques, with the management and use of muscular structures being essential for the repair.21–24 Nonetheless, the only study included in our analysis that solely addressed complex ventral hernias also did not show a difference in recurrence rates between the groups (P = .706). 8 Interestingly, in the only study that presented a statistically significant higher recurrence rate for patients with sarcopenia, the sarcopenic group had a significantly larger hernia area compared with the control group, 368 cm2 versus 150 cm2. 25 In this regard, the difference in recurrence could be attributed solely to the differences in hernia sizes, rather than the presence of sarcopenia.26,27
Furthermore, our analysis showed no differences in SSI, but an increased SSO rate for the sarcopenic patients. No clear evidence in the literature has associated differences in muscular volume with an increased rate of SSO. However, factors associated with sarcopenia, such as malnutrition, cancer, and immunosuppression, may be linked to poor wound healing and higher SSO rates following surgical procedures. 28 Previous studies in breast reconstruction for malignancy have evidenced higher rates of skin flap necrosis and wound healing delay.28–30 However, none of those studies found an association between sarcopenia and SSI, seroma, or hematoma rates.28–30 Additionally, among the studies analyzing the impact of sarcopenia on VHR, none of the individual-included studies found differences regarding SSO or SSI for patients with sarcopenia.8,31
The radiological diagnosis of sarcopenia can be incorporated into the preoperative CT evaluation of the hernia defect, which is already performed in the majority of VHR cases. 32 This implies that such an assessment may not incur additional costs and can be routinely conducted during the preoperative evaluation, serving both diagnostic and follow-up purposes. Furthermore, since our analysis suggested that sarcopenia is not associated with increased LOS, probably there would be no significant impact on the duration of hospitalization and its related cost.
Our analysis did not find differences that would justify any preoperative changes, such as delaying surgery due to a diagnosis of sarcopenia. Such delays could be associated with an increased risk of hernia incarceration, particularly in larger defects and incisional hernias.33,34 Additionally, it remains challenging to dissociate the presence of sarcopenia from other comorbidities, such as cancer-associated cachexia and the use of immunosuppressants. 35 In this context, although the presence of these comorbidities is a risk factor for worse outcomes following VHR, there is still no evidence that delaying surgery for these patients is advantageous. The risk-benefit ratio must be analyzed individually for each patient.5,36,37
It is imperative to acknowledge certain limitations in our study. First, the limited data available on this topic, with only three studies published accomplishing our eligibility criteria. Also, all the studies were retrospective, presenting selection bias inherently to its methodology. However, we performed a comprehensive risk of bias analysis that showed low-to-moderate risk in the included studies. Finally, it was not possible to balance other conditions such as cancer, immunosuppression, and older age, so those covariates could have contributed to our overall analysis.
Conclusion
Our meta-analysis of three studies comprising 275 patients found no differences in recurrence, SSI, and LOS between patients with and without sarcopenia. These findings suggest that we don’t have data that support the delay of VHR due to the presence of sarcopenia, but more studies with control of covariates are needed to elucidate the individual impact of sarcopenia on VHR.
Data Sharing Statement
Because this meta-analysis was based on data extracted from previously published research, all the data and study materials are available in the public domain. The authors of this meta-analysis do not have access to patient-level data of the individual studies. Researchers interested in individual-level data from the studies included in this meta-analysis are encouraged to contact the corresponding author from each study for such requests.
Footnotes
Authors’ Contributions
Study design: A.C.D.R., C.A.B.S., D.L.L., J.P.G.K., and F.M. Data collection and analysis: A.C.D.R., C.A.B.S., D.L.L., J.P.G.K., and D.B.S.Z.-O. Article preparation and editing: A.C.D.R., C.A.B.S., D.L.L., J.P.G.K., and D.B.S.Z.-O, and F. M.
Disclosure Statement
A.C.D.R., C.A.B.S., D.L.L., J.P.G.K., and D.B.S.Z.-O. disclose no conflicts of interest. F.M. discloses consulting fees from BD, Intuitive, Integra, DeepBlue, Allergan & Medtronic, outside the submitted study.
Funding Information
The authors did not receive support from any organization for the submitted work.