
Abstract
Introduction:
Historically, colon resection was recommended after one episode of complicated diverticulitis. However, current trends favor a more individualized approach. This review examines elective sigmoidectomy for complicated diverticulitis as well as robotic approaches for diverticular disease.
Methods:
The literature was reviewed for timely (post 2000) and relevant articles regarding robotics and diverticulitis. The articles included large prospective series, retrospective analysis, meta-analyses and randomized controlled trials.
Results:
Primary anastomosis with or without protective ileostomy has emerged as an alternative to the Hartman’s procedure in emergent or urgent surgery in patients without significant comorbidities. Elective sigmoidectomy after an episode of complicated diverticulitis should be decided on a case-by-case basis considering patient characteristics, continued subacute symptoms, complications from the disease, and chance of recurrence episodes.
Conclusions:
There are several variations techniques for robotic sigmoidectomy outlined in this article, and familiarity with all can help depending on the logistics of the case. Minimally invasive colectomy provides superior patient satisfaction and outcomes.
Introduction
Diverticulitis accounts for several hundred thousand hospital admissions and billions of dollars in healthcare spending every year. 1 Despite being a well-defined disease process, the optimal management for diverticulitis continues to pose a challenge to clinicians. In recent years, individualized approaches have replaced standard protocols. Surgical intervention remains a mainstay in the treatment algorithm, but the widespread adoption of robotic surgery is redefining the operative technique. This review outlines how to approach surgical intervention in the modern day and discusses which patients should be considered for elective sigmoidectomy. In addition, the technical steps of a robotic sigmoid resection is presented including different anastomotic techniques, and outcomes related to these approaches.
Indications for surgical intervention
In 2020, both the American Society of Colon and Rectal Surgeons and the World Society for Emergency Surgery released updated guidelines for managing diverticulitis in both the emergency and elective setting.2,3
Urgent operative intervention remains the recommended course for patients with peritonitis or recalcitrant acute diverticulitis. The decision for open versus minimally invasive surgery in the urgent or emergent setting should be considered based on resource availability and surgeon skill.2,3
Regardless of approach to emergent or urgent sigmoidectomy, the decision to perform a Hartmann’s procedure or resection with primary anastomosis with or without a diverting stoma is determined by patient comorbidities. Recent data from randomized controlled trials demonstrate relative safety with similar postoperative morbidity and mortality for either approach in patients with few comorbidities. There is a trend for better stoma reversal in the primary anastomosis group with a diverting colostomy compared with the Hartmann’s procedure as well.2,4,5
For patients with less severe disease who have recovered with nonoperative management, the decision for elective sigmoid colectomy is more nuanced and should be considered on an individual basis. There are several factors that increase future morbidity attributable to diverticulitis which should be considered when discussing elective operative intervention. These include the number of episodes of recurrent diverticulitis; presence of a diverticular abscess; complex cases to include presence of a fistula, obstruction, or stricture; patient age; and immunocompromised status. 3
Following resolution of an uncomplicated episode of diverticulitis, the recurrence rate may range from approximately 10%–30%. 3 While it is unlikely that subsequent recurrences are more severe than the index episode, a patient’s risk of recurrence increases with each subsequent episode of diverticulitis. In addition, subclinical abdominal and gastrointestinal symptoms in patients with recurrent disease improve with elective resection. 6 In this setting, it is reasonable to offer elective sigmoid resection.
Patients who recover with nonoperative management for a diverticular abscess are at a significant risk of recurrence, and it is more likely that the recurrence will be complicated. Recurrence rate increases with abscess size, necessity of percutaneous drainage, and location within the pelvis.2,3 In the appropriate surgical candidate, interval elective sigmoidectomy should be considered for diverticular abscesses.
Diverticulitis complicated by enteric fistula, obstruction, or stricture should also be considered for surgical intervention to achieve symptomatic relief and reduce the recurrence risk. These patients are at higher risk for having complicated recurrent attacks of diverticular disease. These patients also exhibit subclinical symptoms related to the smoldering pathology that does not typically improve with nonoperative management. Elective sigmoid resection reduces the risk of recurrence and subclinical symptoms.3,7
Young age at initial presentation for diverticulitis is also an indication for elective sigmoidectomy due to the lifetime risk of recurrence. While these patients are likely to incur recurrent disease requiring hospitalization, there is less clear evidence regarding the severity of complicated disease. However, they are more likely to be hospitalized with recurrent disease. Elective sigmoidectomy may still be offered as an option to decrease long-term recurrence and morbidity. 3
Previously, there was a low threshold for elective sigmoidectomy for immunocompromised patients with diverticulitis. More recently, data shows similar rates of recurrence and severity of recurrence in immunocompromised patients compared with immunocompetent individuals. Additionally, for patients undergoing elective sigmoidectomy, there are higher rates of postoperative morbidity and wound complications for immunocompromised patients, though there is no recognized difference in overall mortality. 3 When discussing elective sigmoidectomy with an immunocompromised patient, the increased operative risks should be considered.
In the elective setting, a minimally invasive technique should be employed given a multitude of improved outcomes including shorter hospitalization, fewer short and long-term complications, better pain control, and better cost effectiveness when compared with outcomes with an open approach. 8
Technique
Prior to elective sigmoidectomy, preoperative interventions including bowel preparation and ureteral stenting should be considered. There are multiple large database studies and meta-analyses that documented a trend toward lower postoperative complications with combined mechanical and antibiotic bowel preparation.9,10 In the setting of distorted anatomy with recurrent or complicated diverticulitis, the ureter may not be easily identified, or it may be displaced from its normal anatomical position. 11 While ureteral stenting does not prevent ureteral injury, it permits earlier identification of the injury.
For a robotic sigmoidectomy, the patient is positioned in lithotomy with both arms tucked. A Foley catheter and either orogastric or nasogastric tube is placed to decompress the bladder and stomach respectively.
Access to the abdomen is achieved using a Veress needle at Palmer’s point or a Hasson technique at the umbilicus. Once the abdomen is insufflated, four trocar positions are marked with a horizontal orientation along a supraumbilical line or diagonally oriented line between Palmer’s point and the right anterior superior iliac spine (ASIS) ensuring at least 2 cm clearance from the costal margin and ASIS. The Veress entry site is converted into a robotic trocar site. Additionally, the diagonal orientation enables splenic flexure mobilization for a tension free anastomosis. Trocars are spaced approximately 6–8 cm apart. The inferolateral port adjacent to the right ASIS should accommodate a 12 mm port for robotic stapling. An assistant port is placed in the right upper quadrant triangulated between the working ports to ensure sufficient reach into the pelvis. Figure 1 describes port placement.
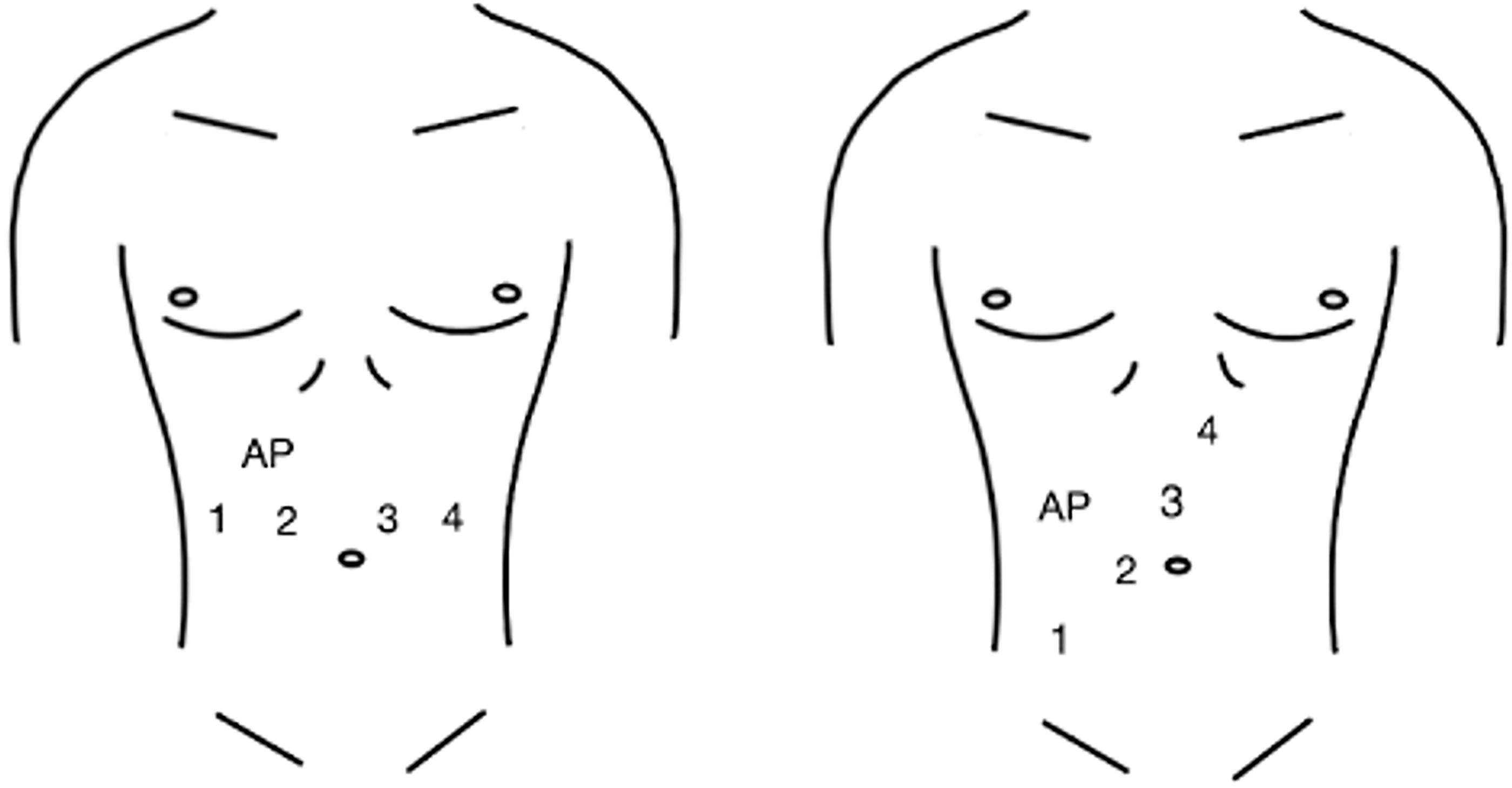
Horizontal and diagonal port placement configurations. Port 1 = 12 mm port for dissection and stapler. Port 2 = 8 mm camera port. Port 3 and 4 = 8 mm port for retractors. AP = 5 mm laparoscopic assistant port.
Prior to docking the robotic platform, the patient is placed in Trendelenburg with left side up and a laparoscopic grasper retracts any omentum or small bowel from the pelvis into the upper abdomen. Once docked, initial robotic instrumentation includes two graspers in ports of the non-dominant hand, and a dissecting instrument with electrocautery capability in the port of the dominant hand.
There are two traditional approaches to minimally invasive sigmoidectomy dissection: medial-to-lateral or lateral-to-medial. Comfort with both approaches is vital as normal anatomy may be often obscured by chronic inflammatory changes in the setting of diverticular disease.
For the medial to lateral approach, the sigmoid colon is grasped and lifted anteriorly. The entire sigmoid colon is inspected for diverticular disease and the proximal healthy portion of colon and proximal rectum are identified as proximal and distal margins of resection, respectively. Adhesiolysis may be necessary to identify normal anatomy. Once the sigmoid colon and its mesentery are free, the inferior mesenteric artery (IMA) is identified, circumferentially dissected and ligated. It is not necessary to perform a high ligation of the vessel given as this is not an oncologic procedure. After the IMA is ligated, the colonic mesentery is divided towards the proximal and distal margins. During this dissection, the ureter is identified and protected. Division of the mesentery proceeds to ensure resection of the diseased colon to normal, healthy colon proximally and to the upper rectum distally, as evidenced by the splaying of the taenia. The lateral attachments are divided to complete the dissection.
Commonly, the medial to lateral approach is not feasible due to extensive adhesive disease or diverticular fistulae that cause the mesentery to fold onto itself. In these cases, the lateral to medial approach should be employed to avoid enterotomies or other inadvertent injuries. The lateral attachments of the colon, and fistula if present, are taken down sharply and the colon is retracted anteriorly and to the right. The ureter and gonadal vessels are identified within this tissue plane. While dissecting a fistula, the surgeon may err on the colonic side to avoid further injury to the remaining side of the fistula. After the lateral mobilization is completed and the ureter is protected, the colon and its mesentery are inspected for healthy sites of colon and rectum to transect. The IMA is identified and ligated similarly to the medial approach and the mesentery is divided in a similar manner until the proximal and distal resection margins are reached.
Further mobilization of the left colon, splenic flexure, or inferior mesenteric vein may be necessary to achieve adequate length and a tension-free anastomosis. Additionally, indocyanine green (ICG) fluorescence may be utilized to ensure adequate perfusion to the margins.
Anastomotic technique
After dissection is completed, the method for transection of the specimen and extraction depends on the anastomotic technique. While all anastomoses are technically intracorporeal, the approaches may be divided broadly into extracorporeal or intracorporeal techniques, with intracorporeal techniques divided between incisional extraction sites or natural orifice extractions.12–14
For an extracorporeal technique, after completion of dissection, the colon is transected distally with a stapler. The robot is then undocked, a Pfannenstiel or lower midline incision is created, and a wound protector placed. The colon is extracted through the incision. The proximal margin is transected, and an EEA circular stapler anvil is secured within the proximal lumen with a purse string suture. The colon is then returned to the abdomen wherein the EEA anvil is coupled to the stapling device. The mesentery and colonic orientation are inspected for twists and perfusion ensured with ICG, then the stapler is fired, and a leak test is performed. 12
The main technical considerations for intracorporeal techniques pertain to which site the surgeon uses for specimen extraction and whether to perform a stapled or handsewn anastomosis. Incisional extraction sites entail a small Pfannenstiel, lower midline, or extension of the right lower quadrant port site incision. 13 If utilizing the right lower quadrant port site, the surgeon extends the incision at the index port and places a capped wound protector to accommodate the robotic trocar. This eliminates the need for an additional incision at the midline. A transrectal natural orifice extraction can even further reduce incisional burden. A natural orifice site does not require an abdominal wall extraction incision and the surgeon may consider reducing the 12 mm trocar to an 8 mm as this technique does not necessitate a stapler. Once the extraction site is determined, a stapled or handsewn anastomosis may be performed.14,15
For stapled anastomoses, if utilizing an incisional extraction site, the distal margin is first transected with a stapler. Next, an appropriately sized EEA anvil is introduced through the extraction incision. A colotomy is created 3–4 cm distal to the proximal transection margin on the specimen side. It should be large enough to pass the EEA stapler anvil. The EEA stapling anvil is introduced through the colotomy, and milked proximally until it is upstream of the proximal transection margin. The colotomy is then closed with a running suture or a sequential firing of the stapler. Following closure of the specimen at the proximal margin, the specimen is removed via the chosen extraction incision. The anvil is brought to the proximal transection margin, and a small colotomy is created to allow for the anvil shaft to exit the lumen. The shaft is then mated with the stapling device in the rectum, and after excluding mesenteric twists and adequate perfusion with ICG, the EEA stapler is fired, and a leak test performed.14,16
If using a transrectal extraction, rather than using a dividing stapler for margin transection, the proximal and distal margins are transected sharply to leave the lumen patent, then the specimen is extracted transrectally. A flexible small wound protector may be passed transanally to facilitate extraction as well. Following specimen extraction, the EEA stapler anvil is then passed into the abdomen transrectally and secured into the proximal transection margin with either an endoloop or purse-string suture placed robotically. 14 The remaining EEA stapling technique is the same as described above.
A robotic intracorporeal handsewn anastomosis may also be performed with any extraction site. For this technique, both transection margins are divided sharply to leave the lumens patent. Once the specimen is extracted, the sutures for the anastomosis are passed through the chosen extraction site. There are multiple techniques described for robotic intracorporeal handsewn anastomoses. In general, barbed, absorbable sutures are utilized in a running fashion to imbricate the bowel edges ensuring a tension free anastomosis with good perfusion and a negative leak test.14,17,18
Outcomes
Overall, minimally invasive colectomy in the elective setting is superior to open cases in terms of overall patient satisfaction, hospital length of stay, and short- and long-term complications. 8 With the introduction of robotic-assisted sigmoidectomies for diverticular disease, there are fewer conversions to open, a lower rate of postoperative ileus, and faster discharge from the hospital when compared with both laparoscopic and open approaches. However, there is a significantly longer operative time for robotic-assisted sigmoidectomy. 19
When comparing extracorporeal versus intracorporeal anastomotic techniques, intracorporeal approaches require longer operative times but result with fewer postoperative complications, quicker return of bowel function, and shorter hospitalizations. 20 One major source of postoperative morbidity are incisional hernias. There is a significantly higher risk of incisional hernia with an extracorporeal technique compared with an intracorporeal approach due to a larger midline extraction site. 21 In addition to requiring smaller extraction sites, intracorporeal techniques reduce the risk of incisional hernia by relocating the extraction port from the midline, or completely with a transrectal extraction.20,21 With the larger extraction incision necessary for extracorporeal techniques, there is also a higher risk of surgical site infection. 22 Extracorporeal approaches also necessitate greater mobilization of the colon to facilitate exteriorization. There is some evidence of an increased risk of conversion to open with this approach to achieve sufficient mobilization, particularly in obese patients. 20 The extensive mobilization may also contribute to slower return of bowel function and time to first oral intake with the extracorporeal approach, with subsequent longer hospitalization.22,23 Extracorporeal approaches are faster than intracorporeal techniques.22,23
Conclusion
Diverticular disease remains a large burden to health care. As treatment strategies become more nuanced, so do surgical techniques. As the approach toward sigmoidectomy continues to evolve, familiarity with minimally invasive robotic sigmoidectomy and the various anastomotic techniques are vital to optimize patient outcomes.
Footnotes
Author Disclosure Statement
The authors have no financial or personal interests to disclose.
Funding Information
No funding was received for this article.