
Abstract
Renal cell carcinoma (RCC) is the most common renal cancer and constitutes a significant burden of disease. Tumor thrombus is present in approximately 10% of cases at initial diagnosis and impacts the morbidity and mortality of the disease. The primary treatment for RCC involves resection of the tumor. The presence of tumor thrombus, therefore, is not only important for prognosis but also for operative planning. Operative approach, including vascular control and caval closure are important consideration when resecting RCC with inferior vena cava (IVC) tumor thrombus and varies based on the patient presentation, extent of the tumor, and the surgeon’s experience. This article presents a patient with RCC with IVC thrombus who ultimately underwent surgical resection with general surgery, vascular surgery, and urology to showcase the multidisciplinary care, surgical considerations, and current management and treatment strategies for RCC with tumor thrombus.
Introduction
Renal cell carcinoma (RCC) is the most common renal cancer, accounting for 2.6% of all cancers in the United States. 1 It frequently presents with hematuria and flank pain and is diagnosed with urine analysis and imaging. 2 Given its late presenting symptoms, metastatic RCC is noted in nearly one-third of all newly diagnosed cases. 2 In addition, extension of the tumor into surrounding vasculature, a phenomenon known as tumor thrombus, is present in up to 10% of RCC cases. 3 RCC has low response rates to chemotherapy, and surgery remains the mainstay of treatment.1,4 This may include either partial or radical nephrectomy with en bloc resection of tumor and tumor thrombus. This article presents a case of RCC with inferior vena cava (IVC) thrombus that ultimately underwent radical nephrectomy with IVC reconstruction by a multidisciplinary team to include urology, general surgery, and vascular surgery. The article also reviews some operative considerations and clinical outcomes associated with this type of unique presentation.
Case Report
The patient is a 78-year-old male with a past medical history of prediabetes, hyperlipidemia, hypertension, and prior tobacco use who initially presented to the emergency department with 2 weeks of hematuria. He denied any flank pain, and no flank mass was appreciable on physical exam. His laboratory findings did not show elevated liver function tests with a normal hemoglobin of 12 g/dL and a baseline creatinine of 0.62 mg/dL. A computed tomography (CT) scan was obtained as a part of the workup and detected a 6.5-cm right lower pole renal mass with IVC thrombus (Fig. 1). He underwent preoperative workup with an MRI abdomen and pelvis, which demonstrated a large heterogeneously enhancing mass arising from the mid-lower pole of the right kidney measuring 6.8 × 5.7 × 8 cm with tumor extension into the right renal vein and IVC as well as right perinephric stranding (Fig. 2). No venous collaterals were identified, and the IVC was dilated at the thrombus site. A CT scan of the chest did not demonstrate any metastases.
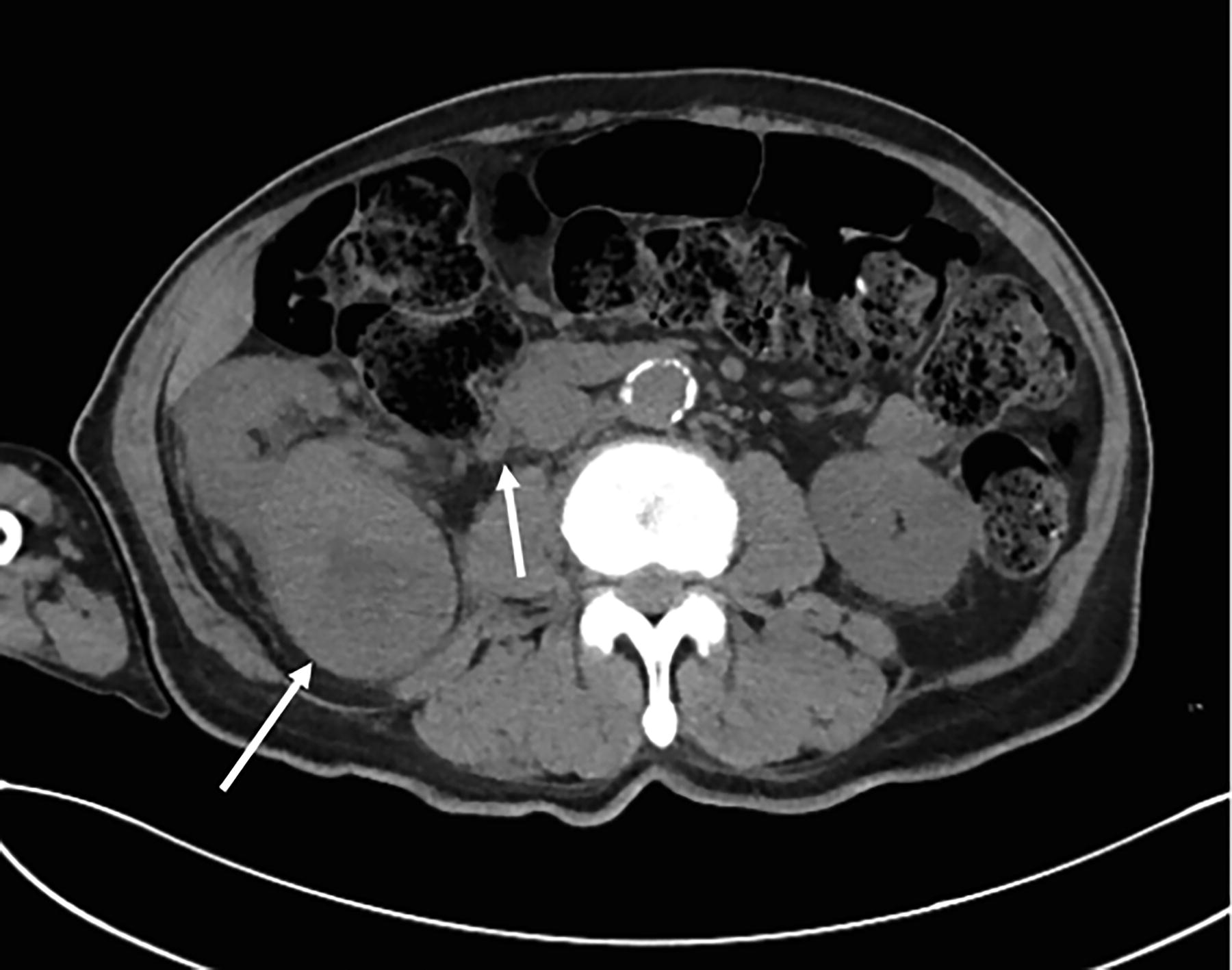
Computed tomography anterior/posterior demonstrating 6.5 cm right lower pole renal mass (white arrow on the left) with inferior vena cava (IVC) thrombus (IVC–renal vein junction noted with white arrow on the right).

MRI abdomen and pelvis demonstrating the extent of tumor extension into the right renal vein and inferior vena cava (white arrow).
He was ultimately scheduled for an open right nephrectomy. General surgery was involved and assisted with operative exposure (Figs. 3–6). Prior to operative intervention, a right common femoral artery angiogram was performed to embolize the right renal artery. The angiogram showed a filling defect in the left renal vein extending into the IVC 2 cm above the left renal vein. The renal artery was embolized with microspheres. The hepatic veins were widely patent with no evidence of tumor or filling defects.

Open approach to radical nephrectomy by general surgery via a Kocher incision.
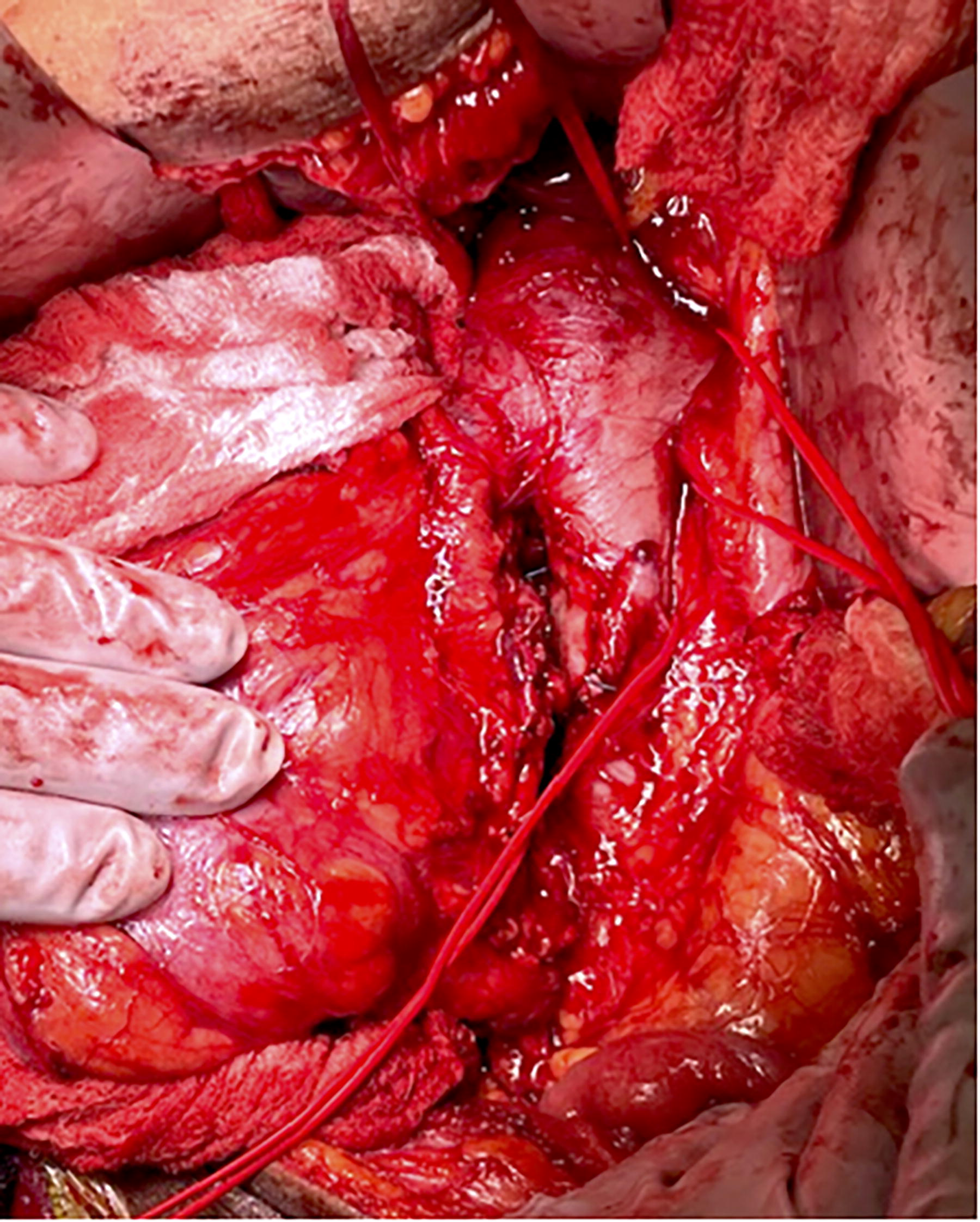
Tumor retracted to the patient’s right with vessel loops around the supra- and infrarenal vena cava and left renal vein.
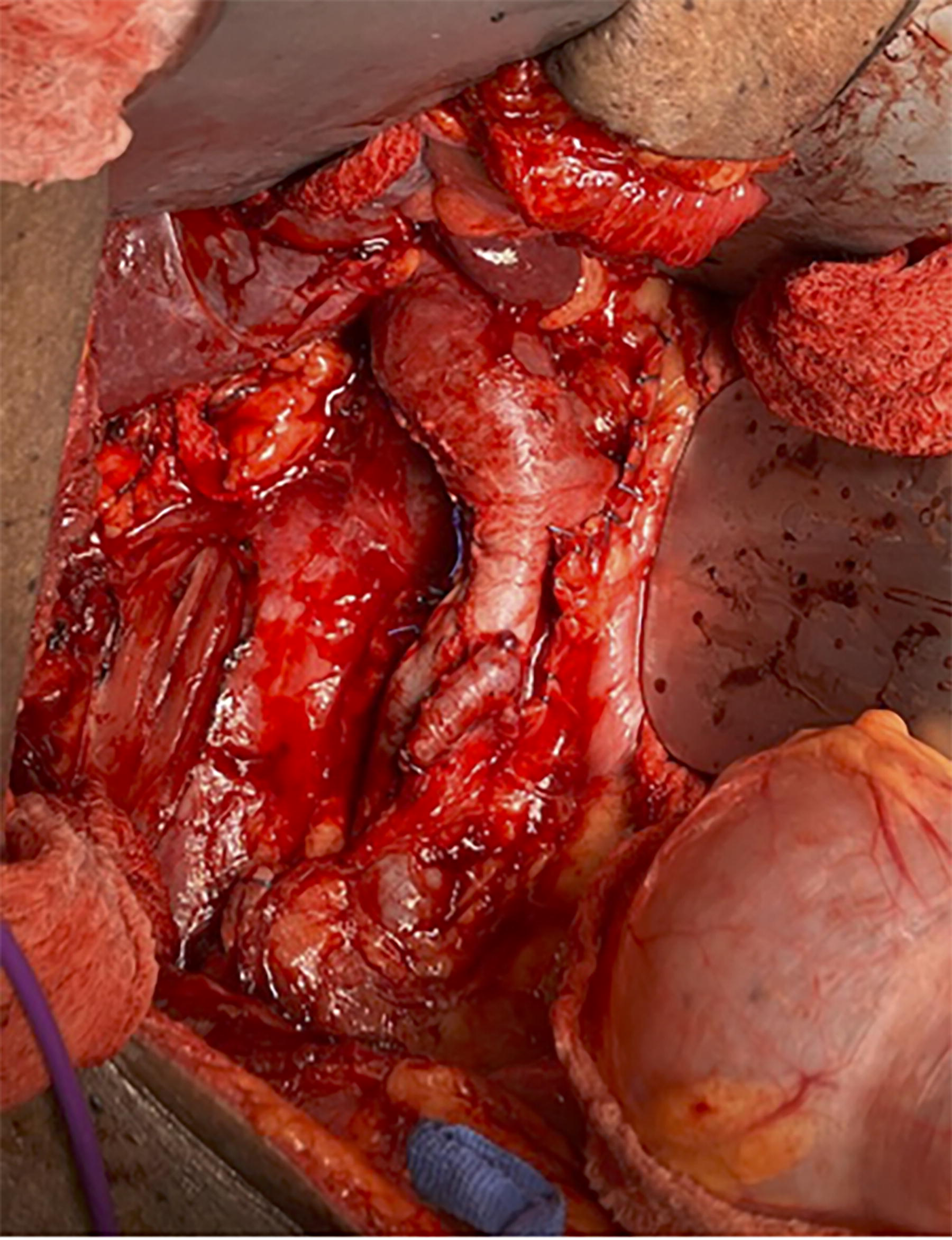
Reconstructed inferior vena cava after tumor resection.

Specimen following en bloc resection, asterisk denoting inferior vena cava.
Following induction, a transesophageal echocardiogram was performed, which confirmed the clot in the IVC. The endoscope was left in the esophagus to monitor for emboli during the operative portion of the case. A Chevron incision was then made across the upper abdomen, and the abdomen was explored. There was no evidence of metastatic disease. The right colon was medialized from the kidney by dividing the white line of Toldt. The duodenum was then Kocherized using sharp dissection, and the space between the ureter and lateral edge of the IVC was incised and dissected from the lower pole of the kidney and psoas muscle. The gonadal vein was divided distal to its insertion into the IVC.
The IVC was dissected anteriorly, extending superiorly from the insertion of the gonadal vein. The dissection continued superiorly on the IVC just caudal to the liver. The attachments of the right adrenal gland were divided from the retroperitoneum, and the right adrenal vein was divided between clips. The caudate lobe of the liver was released from the surface of the IVC, and a small lumbar vein was secured with a 3-0 prolene suture. Vessel loops were secured around the supra- and infrarenal IVC and the left and right renal vein. The lateral and posterior attachments of the right kidney were released. Heparin was administered, and then a lateral venotomy was performed exposing the tumor thrombus. The thrombus was extracted en bloc, and the IVC was repaired with two running 4-0 prolene sutures. The diameter of the IVC was reduced by 50%; however, the IVC was dilated preoperatively due to the tumor thrombus. Thrombin and gel foam were temporarily applied to the repair to ensure hemostasis. A few lymph nodes were identified posterior to the IVC, and these were freed from the IVC, and several branches of the cisternae chyli were secured with clips during this portion of the dissection. The abdomen was then closed.
The patient was admitted to the ICU postoperatively. His diet was slowly advanced with the return of bowel function. He remained hemodynamically stable and did not require blood transfusions in the immediate postoperative period. He had an expected rise in his creatinine on postoperative day (POD) 1 that eventually stabilized to a new baseline of 2.2 mg/dL. He continued to make adequate urine and did not require dialysis. He was started on 5,000 units of subcutaneous heparin every 8 hours for deep vein thrombosis prophylaxis.
The patient was ultimately discharged to a subacute rehabilitation facility on POD 15, tolerating a regular diet. He continued low-dose Eliquis (2.5 mg BID) for 30 days postoperatively given the IVC dissection and malignant disease (Caprini score 9, estimated 10.7% risk of venous thromboembolism [VTE]). 5 He had a follow-up CT on POD 20 that did not show evidence of an IVC thrombosis or significant postoperative pathology. He also had an abdominal ultrasound (US) of the IVC that was normal without concern for a flow-limiting stenosis or thrombosis. Final pathology demonstrated clear cell papillary renal cell carcinoma with renal vein and IVC tumor emboli and three lymph nodes negative for metastasis (T3bN0M0), consistent with a clinical stage III. The patient was a candidate for adjuvant treatment based on current pathology after a multidisciplinary discussion with urology and oncology. He was started on pembrolizumab for adjuvant therapy. He was scheduled for follow-up CT at 6 months to assess for any disease recurrence.
Discussion
Epidemiology
RCC is the most common type of renal cancer and constitutes a significant burden of disease, accounting for nearly 2.6% of all cancers worldwide. 1 It typically occurs in patients 60–80 years old, has a male predominance, and is associated with history of smoking, obesity, polycystic kidney disease, and occupational exposures to include cadmium, asbestos, or petroleum.2,6 Clear cell tumors are the most common variant of RCC, constituting approximately 75%–85% of cases. 2 Other variants include chromophilic, chromophobic, oncocytic, and collecting duct, although these variants occur less frequently. 2 Unfortunately, metastatic disease is present at the time of diagnosis in 23%–33% of cases and affects both overall prognosis and treatment strategies.2,7 Metastases typically occur in the lung, followed by lymphatics, bones, liver, adrenal glands, and brain. 8 Given the advanced stage at initial diagnosis, RCC remains one of the most lethal urological malignancies with a 5-year relative survival rate of 75%. 3
Diagnosis
Traditionally, the classical triad of symptoms associated with RCC are abdominal/flank pain, hematuria, and flank mass, although these occur in only 5%–10% of patients. 2 Workup for suspected RCC includes an urinalysis with cytology, complete blood cell count, liver function tests, calcium level, and a CT abdomen and pelvis. 2 Additional imaging studies that may be considered include a renal US or an magnetic resonance imaging (MRI) of the abdomen.2,9,10 Tumor thrombus is present in approximately 10% of cases and has a significant impact on the morbidity and mortality of the disease.11,12 Tumor thrombus is best characterized in the venous phase of a CT scan or MRI. MRI in particular is good at differentiating bland from tumor thrombus, as well as IVC wall invasion, which is reported in up to 51% of caval thrombus.9,13
Surgery
Surgery is the mainstay of treatment for patients with RCC. Radical nephrectomy is the standard of care for renal cell carcinoma and includes en bloc resection of the kidney, Gerota’s fascia, the ipsilateral adrenal gland, and lymph nodes with the goal of negative margins.1,14,15 A partial nephrectomy may be used as a nephron-sparing technique in tumors <4 cm in diameter or for patients with bilateral renal lesions, single kidney, underlying renal disease, or other patient-specific conditions that may increase the morbidity of a total nephrectomy.1,2,9,14,15 Metastasectomy is recommended for patients with resectable metastases, as it is associated with longer disease-free survival even when systemic therapy is not utilized.1,9,15
With regard to surgical approach, laparoscopic, robotic, and open techniques may be used. A laparoscopic radical nephrectomy is recommended in patients with smaller tumors (T1 or T2) in patients who are unable to undergo a partial nephrectomy. In patients undergoing a partial nephrectomy, robotic approaches are associated with lower estimated blood loss, shorter warm ischemia times, and comparable postoperative outcomes compared to laparoscopic partial nephrectomies. 15 For cases where IVC tumor thrombus is present, an open approach is typically used, although robotic IVC thrombectomy remains an option in select cases. 9
Regardless of approach, the general principles and steps for a radical nephrectomy and IVC thrombectomy remain the same, with the goal of an en bloc resection of both the kidney and tumor thrombus. The abdomen is opened, and adequate exposure is obtained. The extent of exposure is dictated by the level of tumor thrombus and the extent of thrombectomy the surgeon aims to perform. The Mayo classification is a grading system that signifies the extent of tumor thrombus from level 0 to level IV (Table 1). 16
Mayo Classification for Extent of Tumor Thrombus
IVC, inferior vena cava.
In our case and institution, the general surgery team was present to assist in adequate exposure of both the right kidney, adrenal, right renal vein, right renal artery, and IVC. The tumor thrombus was classified as Mayo Level I, and therefore, only juxta renal IVC exposure was required. Laterality is an important consideration. For a right nephrectomy, dissection of the right renal vein is typically free from major structures. On the left, lumbar veins draining into the left renal vein must be carefully dissected to avert hemorrhage. 10 Once the relevant structures are exposed, the renal artery is ligated, followed by vena caval control. 9 Again, IVC control is dependent upon the thrombus level. In our case, the juxta renal IVC, infrarenal IVC, contralateral renal vein, and suprarenal IVC were controlled with vessel loops and then vascular clamps. If a thrombectomy cannot be performed because of tumor involvement in the IVC wall, a partial or complete caval resection may be required.9,13 Following thrombectomy, the cava can either be closed primarily or closed with a patch or graft, depending on the defect. 13
Anticoagulation
The use of anticoagulation (AC) in the perioperative period is a delicate balance based on operative findings and pathology. Typically, the postoperative use of AC should be dictated by the patient’s thromboembolic risk. 9 For patients with known VTE, either secondary or independent of tumor thrombus, prophylactic heparin dosing on POD 0 and 1 with transition to a heparin drip on POD 2 is recommended. 9 Ultimately, these patients may be titrated to a therapeutic level if there are no clinical signs of bleeding.
The type of caval repair or reconstruction should also be considered when discussing prophylactic AC or antiplatelet use. For patients with polytetrafluoroethylene, low-dose AC or antiplatelet may be used. 9 In addition, if there is any concern for caval narrowing following repair, antiplatelet therapy should be considered. 9 Regardless of bland/tumor thrombus presence or reconstructive technique, all patients undergoing a nephrectomy for RCC should receive pharmacologic VTE prophylaxis for 28 days given their increased risk for VTE in the perioperative period. 17 In our case study, the patient was maintained on 30 days of low-dose Eliquis as VTE prophylaxis.
Medical therapy
Systemic chemotherapy is not effective in the treatment of RCC. Several randomized studies demonstrate that 5-FU, interferon alpha, and interleukin-2 produced no survival benefit and were associated with significant systemic toxicity, limiting their use. 15 In patients with high-risk features but no evidence of metastatic disease, adjuvant pembrolizumab for 1 year demonstrated a 37% reduction in disease recurrence following nephrectomy.18,19
Surveillance
In the United States, the 5-year survival rate for RCC is approximately 76%. 20 Recurrence rates range from 30% to 50% in the first 2–5 years following treatment, and approximately 10% of cases recur after 5 years. 21 Although it is well established that these patients benefit from surveillance based on recurrence rates, a formal surveillance protocol has not been established. Surveillance strategies may vary based on tumor size, stage, nuclear grade, and the presence of metastatic disease. 2
Conclusions
RCC is the most common renal cancer and accounts for a significant burden of disease in the United States. Despite advances in immunotherapy, surgery remains the mainstay for RCC treatment. Due to direct extension and vascular invasion, RCC may be complicated by tumor thrombus invading the renal vein or the IVC. Although the presence of tumor thrombus does impact tumor staging and prognosis, surgical intervention with radical nephrectomy and thrombectomy confers an overall and disease-free survival benefit compared with nonoperative management.9,22 Operative approach and surgical technique vary significantly based on patient-specific factors, the extent of tumor, and surgeon preference and experience. The involvement of vascular, cardiothoracic, and general surgery in conjunction with urology may be utilized to safely and successfully complete resection of the tumor and tumor thrombus.
Footnotes
Acknowledgment
The authors would like to thank all members of the team who provided the care detailed in our case report.
Authors’ Contributions
K.C.: Writing, reviewing, and editing. F.B.: Conceptualization, methodology, supervision, reviewing, and editing.
Ethical Approval
Institutional review board approval was obtained from the Washington DC Veterans Affairs Medical Center.
Disclosure Statement
F.B. is an editor for the Journal of Laparoendoscopic & Advanced Surgical Techniques.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.