
Abstract
Background:
Percutaneous cholecystostomy (PC) rates have substantially increased in England over the past two decades. However, its utilization and clinical outcomes at a local level are not well documented or understood. This study aimed to characterize the cohort of patients who underwent PC and resulting clinical outcomes at a tertiary center for hepatobiliary and emergency general surgery.
Methods:
This is a retrospective cohort study of patients treated between 2012 and 2020 at a single center. A subgroup analysis was conducted to compare outcomes between Tokyo grade 2 and Tokyo grade 3 patients.
Results:
In the 73-patient cohort, a 57.1% increase in PC was observed between 2012 and 2020. Compared to the gold-standard Tokyo guidelines, 36 patients (49.3%) met the criteria for PC. Postprocedural complications occurred in 50 patients (68.5%), including PC tube dysfunction (27.4%), intra-abdominal abscess (20.5%), external bile leak (8.2%), and biloma (5.5%). Recurrent biliary infection developed in 30 patients (41.1%). Twenty-seven patients (37%) underwent emergency reinterventions due to acute cholecystitis recurrence. Twenty patients (27.4%) required radiological reintervention. Seven patients (9.6%) required emergency cholecystectomy, and ten patients (13.7%) underwent an elective cholecystectomy. Overall, 36 patients (49.3%) died during the follow-up period. Five patients (6.8%) died during index admission. Subgroup analysis demonstrated a higher rate of complications in the Tokyo grade 3 subgroup of 82.8% vs. 59.1% (P = .04). Patients from this subgroup were also more likely to require emergency additional abscess drainage (17.2% vs. 2.3%, P = .034). There was no significant difference in the number of emergency cholecystectomies performed between groups. Patients from the Tokyo grade 2 subgroup were more likely to have an elective cholecystectomy in the future (20.5% vs. 3.4%, P = .044).
Conclusions:
PC was overperformed in our patient cohort, and was associated with high postprocedure morbidity and mortality. Clinicians should be discerning in patient selection criteria for PC.
Introduction
Percutaneous cholecystostomy (PC) is an increasingly common alternative to cholecystectomy in managing acute cholecystitis. This procedure involves the external drainage of infected biliary contents from the gallbladder under radiographical guidance. PC is indicated for patients at high risk of perioperative death due to poor physiological reserve or septic shock. 1 In cases of prolonged cholecystitis, the decision between surgical intervention versus conservative management with antibiotics and subsequent elective cholecystectomy is controversial, with immediate surgery in these cases carrying an increased risk of postoperative complications due to a greater likelihood of hazardous dissection of the severely inflamed hepatocystic triangle.
Acute cholecystectomy remains the gold standard treatment for most cases of acute cholecystitis due to the increased risk of recurrence of acute cholecystitis with conservative treatment2–5 and the favorable safety and cost of cholecystectomy when compared with cholecystostomy.6,7 However, the rationale, applicability, and use of PC have come under renewed discussion following the 2018 Tokyo Guidelines and several recent studies.2,8–10 The Tokyo guidelines11,12 provide more specific guidance on acute cholecystitis severity, and which “high-risk” patients should be considered for PC. PC is indicated in patients with severe Tokyo grade III cholecystitis who have a Charlson Comorbidity Index (CCI) of ≥4 and an American Society of Anesthesiologists (ASA) score of ≥3. It may also be considered in patients with a Tokyo grade II cholecystitis with a CCI of ≥6 and ASA of ≥3, and where timely cholecystectomy is not practical. Theoretically, other patient groups not meeting these criteria should instead be considered for emergency or elective total laparoscopic cholecystectomy, or in higher risk patients, a subtotal cholecystectomy.
Despite guidance on these selective indications for PC, it has recently been reported that PC annual counts and rates in England are rapidly and disproportionally increasing, with a national database study reporting a steady 723% increase in cholecystostomy procedures between 2000 and 2019. 13 This significant increase may represent a guideline adherent increase in PC procedures due to increasing awareness of the utility of the procedure as well as increasing limitations on resources. In the U.K. context, resource limitations mean only one in seven patients admitted with acute gallstone disease undergo a cholecystectomy within 2 weeks of admission 14 ; PC may be increasingly utilized to address this gap. Conversely, this increase may be due to subjective interpretation of the term “high-risk patient,” 15 resulting in increased use of PC in patients not meeting criteria. This has implications on mortality, morbidity, and health care costs.
This retrospective clinical study at a tertiary center for hepatobiliary surgery aims to evaluate the clinic outcomes and characteristics of 73 patients who underwent PC for acute cholecystitis from 2012 to 2020. Study objectives are to assess the trends in the number of PC procedures performed, compare outcomes between different severity grades of acute cholecystitis, and assess the impact of patient characteristics on morbidity and mortality.
Materials and Methods
Registration and reporting adherence
The Institutional Clinical Audit Management Board reviewed, approved, and registered the project (registration number 11008). As shown in Supplementary Table S1, the study is reported according to the preferred reporting of case series in surgery (PROCESS) guidelines. 16
Identification of PC cases
To identify patients, we used the Office of Population Censuses and Surveys Classification of Interventions and Procedures (OPCS) Fourth Revision OPCS-4 codes J21.4 (drainage of the gallbladder) and J24.1 (percutaneous drainage of the gallbladder), and ICD-10 codes K80.0 (calculus of gallbladder with acute cholecystitis) and K81.0 (acute cholecystitis, without cholelithiasis) for each calendar year from 2012 to 2020. 17 Patients with malignant biliary disease or who underwent open or laparoscopic drainage of the gallbladder were excluded. Of note, patients treated in 2020 were free of coronavirus disease 2019 (COVID-19) during PC. In all cases, PC was performed by consultant interventional radiologists, and the technique utilized was placement of a 10-French locking pigtail multipurpose catheter into the gallbladder under ultrasound guidance with local anesthetic.
Data collection process and systemization
Data were collected from electronic medical record systems between 2012 and 2020. Data points included patient baseline demographics, comorbidities, admission physiology parameters, examination findings, imaging findings, laboratory results, and ASA status. Surgical parameters included complications during and after the cholecystostomy procedure, the length of hospital stay, the recurrence of symptoms, the type and timing of reintervention, and mortality. Mortality was classified into four categories—overall, index admission, 30-day, and >30 days. Causes of death were summarized as biliary, nonbiliary, and unknown. The postoperative follow-up was longitudinal until August 1, 2022.
The data collected were input into a standard Microsoft Excel (Microsoft Corporation, 2020) spreadsheet with patient identification data removed for confidentiality and anonymity. The data were used to calculate the Tokyo severity grade, CCI (https://www.mdcalc.com/calc/3917/charlson-comorbidity-index-cci), and the National Emergency Laparotomy Audit (NELA) mortality and morbidity scores for hypothetical scenario of emergency laparotomy (https://data.nela.org.uk/riskcalculator/).
Statistical methods
Data were validated and edited before being analyzed using SPSS for Windows v29.0.2 (IBM Corp., Armonk, NY, USA) and GraphPad Prism version 10.2.3 (347) for macOS (GraphPad Software, Inc., San Diego, CA, USA). The computing packages for conventional and advanced statistics were used.
Continuous variables were summarized using median and interquartile range (IQR). Ordinal (e.g., ASA class) and binary variables (e.g., postoperative complications) were presented as counts and percentages, with 95% confidence intervals (CIs) calculated using the Wilson–Brown method. Using GraphPad Prism Software, a contingency table was constructed to perform a binary logistic regression comparing Tokyo grade 2 and Tokyo grade 3 patients. The odds ratio (OR) and 95% CIs were computed using the Baptista–Pike method. The P value was computed using a two-sided Fisher’s exact test. The Mann–Whitney U test was used to assess the associations in continuous variables between Tokyo grade 2 and Tokyo grade 3 patients. The associations were considered statistically significant at an α level of 5% (0.05).
Kaplan–Meier analysis was conducted to compare post-PC survival between Tokyo grade 2 and Tokyo grade 3 subgroups of patients using the log-rank (Mantel–Cox) test. Patients alive at the end of the data collection period were censored. Life tables indicate the number of patients alive at each time interval.
Results
Number of cholecystostomy procedures performed
Seventy-three patients underwent PC for acute cholecystitis between 2012 and 2022. Table 1 displays the number of PCs performed each year during this time and the ratio of cholecystectomy to PC. The number performed each year ranged from 1 in 2013 to 12 in 2015 and 2016, and the ratio of cholecystectomy to PC varied from 24:1 in 2020 to 335:1 in 2013, with the summary ratio for the period 2012–2020 of 48:1. There was an overall 57.1% increase in PC from 2012 to 2020. When emergency cholecystectomies and PC were considered, the summary ratio between these two surgical procedures was 8:1. Notably, it was 4:1 (20%) in 2015 and 5:1 (16.7%) in 2014 and 2020.
Acute Cholecystitis Cases, Percutaneous Cholecystostomy Frequency, Rates, and Cholecystectomy to Cholecystostomy Ratios by Year (2012–2020)
PC, percutaneous cholecystostomy.
General characterization of the patient cohort
Table 2 summarizes the patient cohort characteristics described in the following sections. Supplementary Table S2 provides more detailed information.
Summary of Baseline Demographic Information and Preoperative Characteristics of 73 Patients for whom Percutaneous Cholecystostomy was Performed
ASA, American society of anaesthesiologists; IQR, interquartile range; NELA, National Emergency Laparotomy Audit; WBC, white blood cell.
Baseline demographics and patient-related characteristics
The median age for this cohort was 70 years (IQR 24). Thirty-nine patients (53.4%) were female. The median BMI was 30 kg/m2 (IQR 10.5 kg/m2). Sixty-one patients (83.6%) had a CCI ≥3, and 54 patients (74.0%) had an ASA grade ≥3. Hypertension (57.5%), dyspnea/chronic obstructive pulmonary disease (54.8%), diabetes mellitus (34.2%), and heart disease (ischemic or chronic heart failure, 27.4%) were the most prevalent comorbidities.
Tokyo severity grade
Twenty-four patients (33%) had an elevated white blood cell count >18,000/mm³, while 52 (71%) presented with a palpable tender mass in the right upper abdominal quadrant. In addition, 48 (66%) patients reported symptoms lasting >72 hours. Notably, 72 (99%) patients exhibited marked local inflammation, including gangrenous cholecystitis, pericholecystic abscess, hepatic abscess, biliary peritonitis, or emphysematous cholecystitis on imaging.
Seven patients (10%) experienced cardiovascular dysfunction, characterized by hypotension requiring treatment with dopamine ≥5 μg/kg per min or any dose of norepinephrine. Neurological dysfunction, indicated by a decreased level of consciousness (GCS <15), was observed in 11 patients (15%). Respiratory dysfunction, defined by a PaO2/FiO2 ratio <300, was present in 11 cases (15%). In addition, eight patients (11%) had renal dysfunction, evidenced by oliguria or creatinine levels >2.0 mg/dL. Hepatic dysfunction, with an international normalised ratio (INR) >1.5, was noted in five patients (7%), and hematological dysfunction, defined by a platelet count <100,000/mm³, was seen in one case (1%).
Consequently, Tokyo grade 2 acute cholecystitis was diagnosed in 44 patients (60.3%), and Tokyo grade 3 cholecystitis in 29 patients (39.7%). The median mortality risk and morbidity NELA values were 4.4% (IQR 5.7) and 77.0% (IQR 17.9), respectively.
Compared to the gold-standard Tokyo guidelines, 36 patients (49.3%) met the criteria for PC. This group consisted of 27 patients (37.0%) who were Tokyo grade 3, with ASA grade ≥3 and CCI ≥4; and 9 patients (12.3%) who were Tokyo grade 2, with ASA grade ≥3 and CCI ≥6.
Perioperative and long-term clinical outcomes
Gallbladder perforation occurred in one patient (1.4%). Significant PC-related bleeding requiring blood transfusion occurred in two patients (2.7%). Fifty patients (68.5%) experienced postprocedural complications. Among them were PC tube dysfunction (27.4%), external bile leak (8.2%), biloma (5.5%), and intra-abdominal abscess (20.5%). Other perioperative complications included pneumonia (13.7%) and ileus (2.7%).
The median length of initial hospital stay was 12 days (IQR 8), with a median stay of nine days (IQR 9) following PC. After discharge, 12 patients (16.4%) were readmitted within 30 days. The median duration of the cholecystostomy remaining in situ was 42 days (IQR 42). Thirty patients (41.1%) experienced a recurrent attack of biliary infection; 13 (17.8%) while the PC tube was in situ and 17 (23.3%) after PC removal.
Twenty-seven patients (37.0%) underwent emergency reinterventions due to cholecystitis recurrence. Twenty patients (27.4%) required radiological reintervention, including repeated PC (12.3%) or additional drainage of biloma or abscess (13.7%). Seven patients (9.6%) required emergency total (n = 3) or subtotal (n = 4) cholecystectomy. Ten patients (13.7%) underwent an elective cholecystectomy. The median interval between PC and elective cholecystectomy was 62.5 days (IQR 182). Elective endoscopic retrograde cholangiopancreatography was performed in 10 patients (13.7%). Table 3 displays further descriptive statistics by the operative approach and the number of gallbladder resections following PC.
Perioperative and Long-Term Clinical Outcomes Following Percutaneous Cholecystostomy in 73 Patients
IQR, interquartile range; PC, percutaneous cholecystostomy.
Mortality
Overall, 36 patients (49.3%) died during the follow-up period. Five patients (6.8%) died during their index admission, and four (5.5%) died within 30 days of the initial PC procedure. Of the 17 patients who later went on to have a cholecystectomy, there were 3 deaths (17.6%) during the study period. This contrasts with 33 deaths in the 56 patients who did not have a cholecystectomy following the primary PC procedure (58.9%, OR 6.7, 95% CI 1.8–23.3, P = .0047).
Univariable Analyses and Statistical Associations
General characterization of subgroups by Tokyo grade 2 and 3
Table 4 shows that no significant associations were identified by age, sex, BMI, and CCI. More granular information is provided in Supplementary Table S3.
Comparison of Baseline Demographics and Preoperative Factors by Severity of Acute Cholecystitis: Tokyo Grade 2 versus Tokyo Grade 3
∞, infinity; * the significance of the level for the difference between two subgroups.
minimal.
moderate.
high.
maximal.
ASA, American Society of Anaesthesiologists; CI, confidence interval; IQR, interquartile range; NELA, National Emergency Laparotomy Audit; OR, odds ratio; WBC, white blood cell.
Baseline characteristics of disease and preoperative risk grading
When clinical features at presentation were compared, there was a significant difference in neurological function between groups. All Tokyo grade 2 patients were GCS 15 compared with only 69% of Tokyo grade 3 patients (P = .0001). Tokyo grade 3 patients were more likely to have heart failure on chest x-ray (OR .2; 95% CI 1–0.7, P = .01); they also had a lower platelet count (218 versus 292, P = .04) and evidence of clotting derangement with a higher prothrombin time (12.7 versus 11.5, P = .02). There were no significant differences between subgroups in preprocedural abdominal imaging findings. Patients with Tokyo grade 3 cholecystitis had a higher ASA grade overall (93.1% versus 61.4% with ASA grade ≥3, P < .0001) and a higher NELA mortality risk (8.5% versus 4.8%, p = 0.01), as shown in Table 4. Supplementary Table S3 provides a more detailed comparison of baseline demographics and preoperative factors by severity of acute cholecystitis; Tokyo grade 2 versus Tokyo grade 3.
Perioperative and long-term clinical outcomes
Table 5 demonstrates a higher rate of complications in the Tokyo grade 3 subgroup, with 82.8% of patients versus 59.1% of patients developing at least one major postoperative complication (P = .04), specifically intra-abdominal abscess (37.9% versus 9.1%, P = .006). Patients from the Tokyo grade 3 subgroup were also more likely to require an emergency reintervention, specifically additional abscess drainage (17.2% versus 2.3%, P = .034).
Perioperative and Long-Term Clinical Outcomes by Severity of Acute Cholecystitis: Tokyo Grade 2 Versus Tokyo Grade 3
∞, infinity; *the significance of the level for the difference between two subgroups.
minimal.
moderate.
maximal.
CI, confidence interval; ERCP, endoscopic retrograde cholangiopancreatography; IQR, interquartile range; PC, percutaneous cholecystostomy.
There was no significant difference in the number of emergency cholecystectomies performed between subgroups. However, patients from the Tokyo grade 2 subgroup were more likely to have an elective cholecystectomy in the future (20.5% versus 3.4%, P = .044).
Mortality by subgroup
There was no significant difference in mortality between the Tokyo grade 2 and Tokyo grade 3 subgroups of patients who underwent PC. Figure 1 displays Kaplan-Meier survival curves for each group.
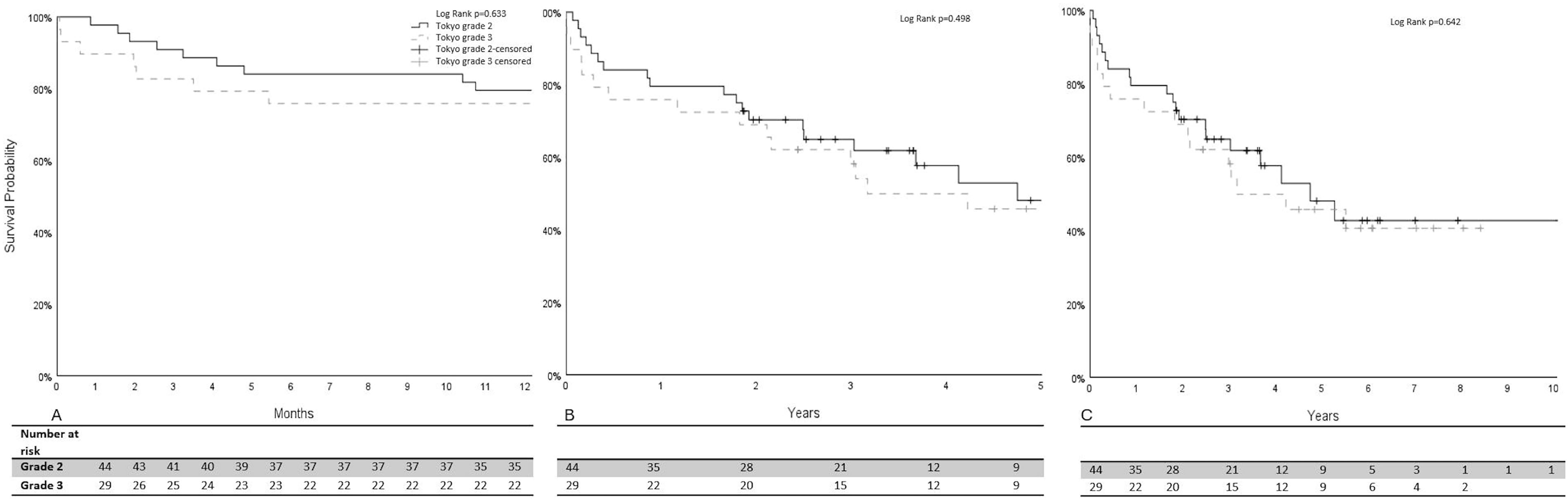
Kaplan–Meier survival curves for patients with acute cholecystitis treated with percutaneous cholecystostomy (PC), comparing Tokyo grade 2 (solid line) and Tokyo grade 3 (dashed line) patients.
Discussion
This study examined 73 adult patients who underwent PC at a tertiary teaching hospital from 2012 to 2020, evaluating clinical outcomes based on Tokyo grade to inform future patient selection. These findings emphasize the need to address the high frequency of PC in acute cholecystitis and advocate for using local data to discourage its use in moderate or severe cases without other indications. This study reveals no decrease in PC usage over time in emergency settings and highlights the importance of evaluating and stratifying patients with acute cholecystitis to guide treatment, as recommended by the Tokyo guidelines.
We found that PC was overperformed in our cohort compared with the gold standard Tokyo Guidelines.11,12,18 Overall, 36 patients (49.3%) were indicated for PC as the primary procedure; this consisted of 27 patients (37.0%) who were Tokyo Grade 3 with CCI ≥4 and ASA grade ≥3, and a further 9 patients (12.3%) who were Tokyo Grade 2 with CCI ≥6 and ASA ≥3. These findings suggest that 50.7% of patients may have been more appropriately managed by either initial laparoscopic cholecystectomy or a conservative approach in line with the Tokyo recommendations; this may have resulted in better outcomes for such patients. Possible reasons for the overuse of PC in our cohort include lack of access to theatre space and resources, meaning cholecystectomy could not be performed in a timely manner, and Tokyo guidelines not being utilized by clinicians when determining management.
Overall, clinical outcomes were poor with a high frequency of readmissions, repeat procedures, and emergency cholecystectomies. Notably, 23% of patients had recurrence of acute cholecystitis after PC drain removal, and 37% of patients required some form of emergency reintervention. These results are in line with similar previous studies. Horn et al. 5 demonstrated an acute cholecystitis recurrence rate of 23.5% following PC over a median period of 5 years, and de Mestral et al. 19 reported recurrent biliary complications in 12%–29% of patients following PC. These figures reinforce that PC does not preclude further biliary disease and should not be employed routinely as a definitive management strategy for acute cholecystitis. Mestral et al. also reported overperforming PC compared with the Tokyo Guidelines, as 41 patients (60%) were in the ASA 2 and 3 categories and may have been managed more appropriately by cholecystectomy rather than PC as the primary intervention.
A multicenter randomized controlled trial by Loozen et al. (the CHOCOLATE study) sought to compare outcomes of PC to laparoscopic cholecystectomy as a treatment for moderate-to-severe acute calculous cholecystitis. 2 They reported an increased rate of major complications following PC compared with cholecystectomy of 65% versus 12%. However, only 18% of patients assessed were included in the study, and patients with an APACHE 2 score of 15 or more were excluded as a cholecystectomy was considered strongly contraindicated. The results are therefore not directly comparable to our study, which included all patients who underwent PC at our center. Despite this, results in the PC group were similar, with complications reported in 65% of patients who had PC, which is in line with 68.5% in our study.
Hall et al. 6 also compared outcomes of PC and cholecystectomy for patients with acute calculous cholecystitis. They analyzed outcomes of 9,561 patients who received treatment for acute cholecystitis, 20% of whom received PC, and reported that emergent cholecystectomy for cholecystitis in high-risk patients is both safer and more cost-effective than PC. However, these procedures are not directly comparable, as PC is only indicated when a cholecystectomy is not considered appropriate due to extensive comorbidities, frailty, or acute systemic illness. It is therefore difficult to situate these results in clinical practice.
When results between Tokyo grade 2 and 3 subgroups in our cohort were compared, there was a higher rate of complications in the Tokyo grade 3 group (82% vs. 59%), with more requiring emergency intervention. Unfortunately, options are limited for patients with Tokyo grade 3 cholecystitis, and previous studies have shown poor outcomes in patients who have emergency cholecystectomy in this group.20,21 However, despite the higher rate of complications and reinterventions in the Tokyo grade 3 subgroup in our study, no overall difference in mortality was identified.
Of 73 patients who underwent PC in our cohort, 23% proceeded to have a cholecystectomy. This figure is slightly lower than that of previous studies.2,3 Patients who went on to have a cholecystectomy as a definitive procedure performed significantly better overall, with lower (17.6% vs. 58.9%) mortality during the follow-up period (OR 0.1, 95% CI 0.04–0.6). This supports PC as a temporary measure to bridge to cholecystectomy. Patients who did not have a cholecystectomy had worse outcomes, which is likely to be related to their baseline frailty, as patients who were frailer with more comorbidities would not have been considered for a definitive surgical procedure.
The limitations of our study stem from its retrospective design. We lacked detailed data on mortality causes and had a small sample size, limiting the generalizability of outcomes. In addition, PC was not compared with other management approaches, so we cannot determine if alternative treatments would have yielded better outcomes. As with other similar studies, our findings should be interpreted cautiously. Although previous research has compared PC outcomes with emergent laparoscopic cholecystectomy, it is important to note that PC is not a definitive treatment for acute calculous cholecystitis; it serves as a temporary measure when cholecystectomy is not feasible or practical. Future studies should compare complications and outcomes of high-risk surgical patients undergoing PC versus conservative management.
Conclusion
PC was a frequent surgical procedure in patients with acute cholecystitis. It was overperformed in our patient cohort and was associated with high postprocedure morbidity and mortality. Clinicians should be discerning in patient selection criteria for PC.
Footnotes
Authors’ Contributions
E.M.R.B. and C.H.B.: Contributed equally to the paper and should be considered joint first authors. E.M.R.B.: Methodology, data curation, formal analysis, writing—original draft, writing—review, and editing. C.H.B.: Methodology, data curation, data validation, formal analysis, writing—original draft, writing—review, and editing. B.C.: Data curation and writing—review and editing. A.C.: Data curation and writing—review and editing. A.G.: Data curation and writing—review and editing. R.L.: Conceptualization, methodology, data curation, formal analysis, supervision, writing—original draft, writing—review, and editing.
Disclosure Statement
E.M.R.B., C.H.B., B.C., A.C., A.G., and R.L. have no conflicts of interest to declare.
Funding Information
No funding was received.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.