
Abstract
Background:
We tried to demonstrate the use and benefits of hybrid-video-assisted thoracic surgery (VATS) in Pancoast tumors by comparing it with open surgical approaches.
Methods:
Between January 2022 and January 2024, 29 patients operated for Pancoast tumor were retrospectively evaluated. Hybrid-VATS approach was used in 14 cases, while open surgery was used in 15 cases. The two groups were compared regarding demographic characteristics, preoperative and postoperative findings. Preoperative thoracic computed tomography findings were analyzed by an experienced radiologist to guide the choice of surgical approach.
Results:
The hybrid-VATS technique was statistically significantly superior to the thoracotomy group in terms of operative time and preoperative bleeding amount (P: .027, .012, respectively). There were statistically significantly fewer postoperative complications in the hybrid-VATS group (66.6% versus 21.4%, P:. 04). In preoperative thorax CT evaluation, the longest distance (>77 mm) at which the tumor invaded the chest wall was found to be statistically predictive in the choice of surgical approach (odds ratio: 7.3, P:. 01).
Conclusions:
Hybrid-VATS can be used in Pancoast tumor surgery in experienced centers with shorter operation time, less preoperative bleeding, and low postoperative complication rates compared with open surgery without compromising oncological principles. Preoperative thoracic CT may guide the choice of surgical approach.
Introduction
Approximately 30% of nonsmall cell lung cancers are detected as locally advanced diseases and about 5% of these cases originate from the superior sulcus, showing chest wall/vertebral invasion. 1 The term Pancoast tumor was defined for the first time by Henry Pancoast for tumors located in the superior sulcus. 2 In the following years, Detterbeck stated that a tumor should have involvement above the second costal level to be considered as Pancoast, and this definition is still valid today. 3 According to current guidelines, the accepted treatment modality in resectable cases without N2 is anatomical resections with unblock removal of the invaded chest wall after neoadjuvant concomitant chemotherapy (CTx) and radiotherapy (RT). 4 Many extended surgical methods have been described for surgical approach in superior sulcus tumors. 5 While posterolateral (Shaw-Paulson) incision is used in posterior localized tumors, transmanubrial (Grunewald) or transclavicular (Dartevelle), and their modifications and hemi-clamshell incision are preferred in anteriorly localized tumors. 5 As a result of developing experience in minimally invasive surgery, the video-assisted thoracic surgery (VATS) combined approach with open surgery (hybrid approach) has started to be preferred by experienced surgeons in experienced centers in superior sulcus tumors. 6
In this study, we compared the perioperative and early postoperative outcomes of hybrid-VATS surgery with open surgery in superior sulcus tumors. We investigated whether the minimally invasive approach is sufficient in terms of oncological principles. In addition, we aimed to determine the CT radiological markers that may guide the decision of surgical approach in the preoperative period.
Materials and Methods
Between January 2022 and January 2024, 31 patients who were planned to be operated for Pancoast tumor were retrospectively evaluated. Two cases with N2 in preoperative mediastinal staging were excluded from the study. Hybrid-VATS approach (VATS group) was used in 14 cases, while open surgery (thoracotomy group) was used in 15 cases. Since the hybrid-VATS technique has been used in Pancoast tumor surgery in our center for the last 2 years, the study interval was limited to the last 2 years to ensure homogeneity between the groups.
Thoracoscopic extended surgical procedures have increased in recent years with our clinical experience. VATS Pancoast surgery has been performed in our clinic for the last 2 years. We state that while the thoracotomy selection was higher in the first period, the VATS selection has been higher recently. No clear criteria were selected for the hybrid versus open approach before the surgery.
All cases were evaluated radiologically with positron emission tomography-computed tomography (PET-CT) in the preoperative period. Tumors were diagnosed by transthoracic fine needle aspiration biopsy. Mediastinal staging was performed by endobronchial ultrasonography (EBUS) or mediastinoscopy in patients with suspicious pathological lymph nodes (LNs) for metastasis in the mediastinal area on thorax CT and PET-CT evaluation. In potentially operable patients with clinical absence of N2 and no evidence of distant metastasis, concurrent three cycles of platinum-based CTx and 60 Gray RT for 30 days were routinely applied except for one salvage surgery patient. After induction treatment, the cases were operated within 4–6 weeks. Only one case was operated on in the fifth month after definitive treatment because it was operated for salvage.
Thoracic CT was performed in all patients preoperatively to evaluate the response to induction treatment in the early preoperative period. Mediastinal staging was performed by EBUS or mediastinoscopy in patients with suspicious pathological LNs for metastasis in the mediastinal area on thorax CT and PET-CT evaluation. Preoperative mediastinoscopy was performed in patients with suspected mediastinal LN positivity, suspected N1, or no invasive mediastinal staging before induction therapy. If PET-CT uptake is higher than 2.5, we perform mediastinoscopy if the first applied sampling method is EBUS. If the first applied method is mediastinoscopy, EBUS is preferred.
The primary aim of the study was to determine whether the hybrid-VATS procedure was adequate in terms of the procedure’s reliability from an oncological viewpoint compared with open surgery. The secondary aim of the study was the safety of the hybrid-VATS approach versus open surgery in terms of early morbidity, mortality, operative time, hospitalization stay, drainage times, and perioperative bleeding. While the primary outcomes were oncological results, secondary outcomes were complications and mortality between the two groups.
Finally, the third aim of the study was whether preoperative thorax CT findings after induction therapy affected the choice of hybrid-VATS or open surgery. For this purpose, thorax CT images taken in the preoperative period were re-evaluated by an expert radiologist. The longest radiological diameter of the tumor, the mean diameter of the tumor (arithmetic mean of the longest diameter and the longest diameter on the axis perpendicular to the longest diameter), the volume of the tumor (arithmetic mean of the tumor circumferences in each section) and the thoracic wall invasion surface area in the largest area on a single axis were calculated (Fig. 1).

Preoperative thorax computed tomography findings.
Surgical technique of hybrid-VATS
All patients were placed in the lateral decubitus position after double lumen intubation. In contrast to the standard position, patients were tilted approximately 10°−20° anteriorly due to the posterior utility incision. A patient with an anterior localization and planned trans manubrial (Grunenwald Spaggiari) approach was placed in the supine position. In one of the hybrid-VATS cases, because of the anterior localization of the tumor, the additional utility incision was made from the axillary line and this patient was also placed in the standard lateral decubitus position (Fig. 2).
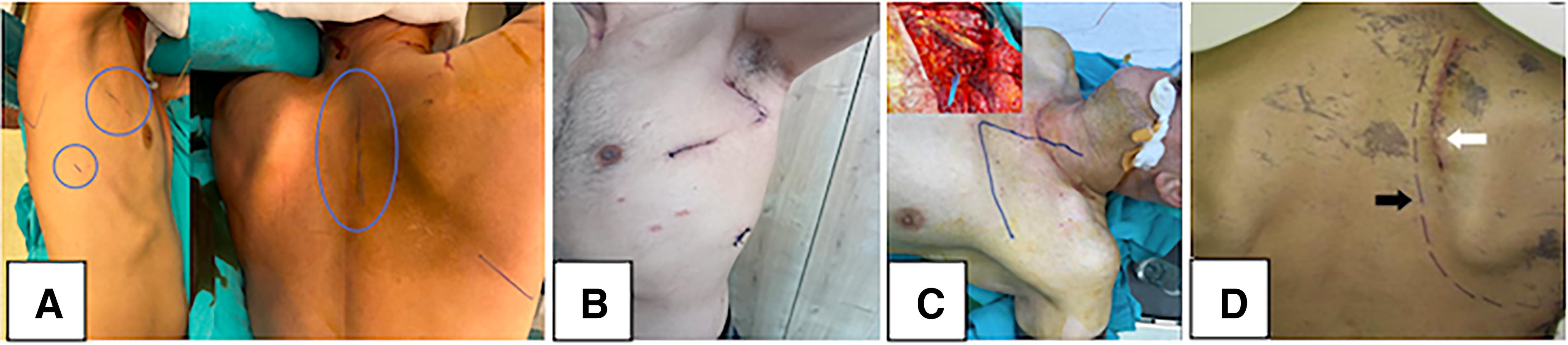
Type of incisions.
The thorax is then entered uniportally (3 cm utility incision through the fourth or fifth intercostal space midaxillary line) or biportally (camera port through the seventh intercostal space posterior axillary line) according to the surgeon’s preference. The thorax is explored with a 30° video thoracoscopic camera. Once the invaded area in the chest wall is identified, standard anatomical resection is started. Pneumolysis is not performed in the area where the lung invades the chest wall. In the first nine cases, standard lobectomy and subsequent chest wall resection were performed consecutively by the same surgical team, whereas in the last five cases, 2 separate surgeons operated simultaneously through the posterior and anterior utility incisions.
To determine the level and length of the posterior incision, a transthoracic needle is inserted through the intercostal space either from the inside of the thorax to the outside of the thorax or from the outside of the thorax to the inside of the thorax under the endoscope camera visualization. In this way, the last rib at which the chest wall is invaded is determined.
Superiorly, the incision is made approximately 6–8 cm up to the level of the T1-C7 vertebra (Fig. 2, posterior utility incision). This incision can be extended if necessary. With the posterior utility incision, a simple rib spreader is used at the level of skin, subcutaneous, and muscular tissues, while a complex rib spreader is used when the costovertebral junction is reached, providing a wide angle of view. One part of the retractor is placed on the medial part of the scapula and the other part is placed over the paraspinal muscles. Then, the muscular structures on the rib toward the medial edge of the scapula are scraped with blunt dissection. The scalene muscles are excised with cautery.
With the help of a 30° video thoracoscopic camera, the pulmonary arteries and veins leading to the upper lobe are divided and then the bronchus and, if incomplete, the fissure are divided. During all these procedures, the upper lobe is not separated from the area where it invades the chest wall. The standard upper lobectomy procedure is completed and the specimen is left isolated and invaded in the chest wall.
The posterior parts of the ribs planned to be resected are resected with a rib cutter through the posterior utility incision or, if necessary, disarticulated with the help of a rugine tool. Both incisions can be used to cut the anterior parts of the invaded ribs. In positions where anterior utility is used, the area where the upper lobe invades the thorax is determined with energy devices under the guidance of an endo camera. After the rib area to be resected is liberalized with energy devices, the rib is rotated with an endo dissector and cut using an endo rib cutter. We recommend total excision and removal of 0.5–1 cm rib segments when resecting the ribs to leave the surgical margins intact and to mobilize the perioperative specimen.
As the operation progresses, the excised part of the chest wall is separated from the posterior musculature and scalene muscles. At this time, the chest wall area to be manually excised from the posterior area is pushed into the thorax with force, while the surgeon in the anterior area divides the remaining connections with energy devices and assists in traction with endo-instruments.
Disarticulation of the first rib and cutting the anterior border is more difficult than the other ribs. T1 plexus is seen at the posterior border of the first rib and T1 plexus is cut in case of invasion. No invasion of the subclavian vein or artery was observed in any of our hybrid-VATS cases. The mass is dissected from these areas, taking care not to damage the vascular structures. After en-bloc resection, the specimen was then removed en-bloc from the pleural cavity via posterior utility incision. The radical dissection of all mediastinal LNs was routinely carried out in the standard fashion.
Prostatic material or prolene mesh was not required for the closure of the chest wall defect in any patient who underwent the hybrid-VATS method. Chest drains were placed on suction through the trocar ports.
Postoperative process
Postoperatively, all patients were extubated in the operating room and taken to the postanesthesia care unit. Patient-controlled analgesia was used as standard in all cases. Patients who were cardiac and respiratory stable at 16–24 hours of follow-up were then transferred to the thoracic surgery service. Drains were terminated in patients whose daily drainage amount fell below 300 ml and who had no parenchymal air leakage. Patients who were stable in terms of laboratory, clinical, and radiological findings were called for outpatient clinic control on the 10th day and discharged.
Statistical analysis
While the data were analyzed retrospectively through patient files, there were no missing data since the patients in the study belonged to the last 2 years. The Windows Office Excel 2020 and Word 2019 versions were used to create the database. THE IBM SPSS Statistics Version 26 program was used for statistical calculations. Patients were divided into two groups as thoracotomy and hybrid-VATS groups. The descriptive results of the study are presented together with the corresponding percentages in the case of nominal or ordinal variables. Continuous variables are presented with mean and standard deviation values. Pearson-chi-square test and Fisher’s exact test were used for categorical variables and the Mann–Whitney U test was used for noncategorical variables. P value below .05 was considered significant.
Results
The mean age of the patients was 59.6 ± 7.3 (R: 47–78) years and 29 patients were included in the study. While 26 (89.7%) of the patients were male, 3 (10.3%) were female. Thoracotomy (thoracotomy group) was used in 15 cases and hybrid-VATS (VATS group) technique was used in 14 cases.
When demographic characteristics were examined between the groups, no statistically significant difference was observed in terms of age, gender, smoking, Charlson Comorbidity Index values, tumor lateralization (right versus left), and tumor localization (anterior versus posterior). (P:. 973, .584, .914, .983, .617, .741, respectively).
When evaluated in terms of the reliability of the hybrid-VATS procedure, a statistically significant difference was found between the groups in terms of operative time (thoracotomy group: 330 ± 66 minutes VATS group: 276 ± 48 minutes), perioperative bleeding amount (606 ± 265 mL versus 417 ± 179 mL) in favor of the hybrid-VATS approach. (respectively, P:. 027, .012). No significant difference was found between the groups in terms of drainage time (6.2 ± 2.5 versus 4.7 ± 2.1 days) and hospitalization stay (6 ± 2.4 days versus 5.4 ± 2 days) (P:. 085, .186, respectively).
Demographic characteristics, and perioperative and postoperative process details of the patients are summarized in Table 1.
Demographic Characteristics of the Patients, Peroperative and Postoperative Details
When evaluated in terms of surgical and oncological principles, no significant difference was observed between the groups in terms of the number of ribs resected, invasion rates of the T1 branch of the plexus brachialis, resection types, number of LN stations sampled, and histological types of tumors (respectively, P:. 561, .542, .348, .290, .861). In one case in the thoracotomy group, subclavian artery invasion was observed and repaired without the need for a graft. In one case, the neurosurgery team was involved due to vertebral invasion and a partial vertebrectomy was performed. In the thoracotomy group, prolene mesh was used to close the chest wall defect in four cases and this ratio was statistically significant between the groups (P:. 037). When evaluated in terms of oncological principles, no significant difference was observed between the groups in R0, R1, and R2 resection rates (P:. 571). In the case approached transmanubrially in the thoracotomy group, advanced invasion was observed in the mediastinal area and resection was performed as a wedge and the surgical margins were left as R2. In the VATS group, the patient who was left R2 was the patient who underwent surgery in the fifth month after definitive CT and RT for salvage surgery. Since the tumor could not be completely removed from the junction of the aortic arch, subclavian artery, and vertebra, the resection was completed as R2.
Postoperative pathological examination revealed no N2 in any case. No significant difference was observed between the groups in terms of N status (P:. 224). Although the proportion of patients with complete response was higher in the thoracotomy group, there was no significant difference between the groups in terms of postoperative stages (P:. 116). Oncological details and pathological results are summarized in Table 2.
Oncological Details and Pathological Results
Postoperative complications were graded according to the extended Clavien–Dindo classification of surgical complications established by the Japan Clinical Oncology Group. 7 Accordingly, Grade I, conditions requiring clinical observation only; Grade II, conditions requiring medical management; Grade IIIa, conditions requiring medical intervention under local anesthesia; Grade IIIb, conditions requiring surgical intervention; Grade IVa, life-threatening complications requiring intensive-care-unit management; Grade IVb, life-threatening complications involving multiple organ failure; and Grade V, death.
In the early postoperative period, complications were seen in nine cases (66.6%) in the thoracotomy group and three cases (21.4%) in the hybrid-VATS group. Statistically significantly fewer complications were observed in the hybrid-VATS group (P:. 04). In the thoracotomy group, secretion retention was observed in two cases, pneumonia in two cases, wound site infection in three cases, cerebrospinal fluid leak in one case, and atrial fibrillation (AF) in one case. One patient with wound infection was revised under general anesthesia after three sessions of vacuum-assisted closure (VAC) device application, while the infection was controlled with a sterile dressing and empirical antibiotherapy in two cases. One patient who developed pneumonia died as a result of respiratory failure and subsequent multiorgan failure. In two cases with secretion retention, treatment was performed by fiberoptic bronchoscopy in the intensive care unit on postoperative day 1. In the case of cerebrospinal fluid leak, no treatment was applied and drainage was discontinued on day 6. The patient with AF was followed up in the intensive care unit for 24 hours and the rhythm recovered with antiarrhythmic treatment. In the hybrid-VATS group, wound infection was seen in one patient, and hemorrhage/hematoma was seen in one patient on postoperative day 1. This case was revised under general anesthesia on postoperative day 1. The patient who developed a wound infection in the posterior utility incision was revised after three sessions of VAC application and the wound was revised and primary closure was performed under general anesthesia. One patient developed prolonged air leakage and subsequent pneumonia. With medical follow-up, air leaks disappeared on the seventh day and the drain was terminated. Postoperative 30-day mortality and morbidity are summarized in Table 3.
Postoperative Morbidity and 30-Day Mortality
In preoperative thorax CT evaluation, the mean longest tumor diameter, longest tumor diameter, total volume of the tumor, and chest wall invasion width were numerically lower in the hybrid-VATS group, but no statistical difference was observed (respectively, P: .217, .591, .847, .194).
According to the ROC (Receiver Operating Characteristic) analysis, the threshold value was determined as 77 mm according to the specificity (67%) and sensitivity (78%) values for preoperative chest wall invasion width assessment. This value and a higher odds ratio indicate that 7.3 times more thoracotomies were performed. This ratio was found to be statistically significant (P: .014). Preoperative thorax CT radiological analyses are summarized in Table 4.
Preoperative Thorax Computed Tomography Analyzes
Discussion
To date, many approaches have been described for the surgical approach to Pancoast tumors. While the prominent approaches are the posterolateral (Shaw-Paulson) incision in the posterior localization, in anterior localization, transmanubrial (Grunewald) or transclavicular (Dartevelle) approaches have been frequently preferred. For long-term survival, different surgical approaches did not influence the 5-year survival rate. 8 In recent years, as a result of increasing experience in minimally invasive surgery, the hybrid-VATS method in superior sulcus tumors has become feasible in experienced centers by experienced surgeons by adhering to oncological principles. 9
In early publications, the use of VATS in superior sulcus tumors was limited to obtaining the diagnosis by biopsy, for intraoperative staging and assessment of resectability. 10 In the following years, Koshiko et al. 11 reported a case of video-assisted en-bloc resection of a Pancoast tumor. In the following years, larger series were published and the details of the hybrid-VATS method were tried to be described. 6
In tumors invading the chest wall, it may be possible to approach completely by VATS. 12 However, in cases with vertebral invasion or invasion at the costovertebral junction requiring disarticulation, a hybrid approach with an additional incision is required. While VATS provides an excellent field of view in lung cancer surgery, the hybrid approach allows direct access to the tumor through an additional incision. In this way, en-bloc resections can be performed with smaller incisions than open surgery.
Caronia et al. 13 reported a comparative analysis of Pancoast tumor resection performed via VATS versus standard open approaches and in the cases in which VATS was performed it was observed less pain, better recovery of forced vital capacity and forced expiratory volume in 1 second, and a reduction in opioid and analgesic consumption. In the long-term follow-up of the patients, there was no difference between the thoracotomy group and the VATS group in terms of local recurrence.
Hybrid-VATS approaches can also be applied in uniportal approaches where the camera port is not used. 14 We approached one of our cases in a uniportal manner. Today, in addition to the hybrid-VATS approach, robotic approaches are also used by experienced centers. 15
Koshiko et al. 11 described en-bloc resection with the transcervical approach in addition to the thoracoscopic approach in the case of an anteriorly localized Pancoast. In one case in our case series, the tumor was partially anteriorly localized. In this case, we performed chest wall resection with an axillary 5 cm incision in addition to the utility incision without changing the position of the patient. We have not seen a case with a similar incision in the literature.
Caronia et al. 6 reported the mean operation time as 200 minutes (range: 185–280 minutes), mean blood loss as 325 mL (range: 250–1200 mL), and mean hospital stay as 9 days (range: 8–30 days) in their series of 10 cases. In one case in the case series, the subclavian artery was involved by the tumor and was replaced by a polytetrafluoroethylene graft. In two patients, there was tumor involvement of the subclavian vein. The veins were resected without reconstruction. We did not have any case of vascular invasion in our series of patients who underwent hybrid-VATS.
Hireche et al. 16 reported the operation times as 315.5 minutes (range: 250–375 minutes). The average blood loss was 665 mL (range: 100–2500 mL). The average hospitalization stay was 14 days (range: 6–50 days) in their hybrid-VATS Pancoast series of 10 cases with vertebral invasion. In six cases, hemivertebrectomy was performed and in four cases wedge corpectomy was performed.
In the present study, operation time (276 ± 48 minutes) and preoperative bleeding (417 ± 179 mL) were compatible with the literature. Since our center is a high-volume hospital, patient circulation is high. Therefore, our mean hospitalization stay (5.4 ± 2 days; range 3–11 days) is shorter than the times mentioned in the literature. In our hybrid-VATS series, we have a case of vertebral invasion whose resection was R2. A significant difference between the two groups in terms of postoperative complications was noteworthy in our study.
The multimodal treatment approach accepted by the guidelines is R0 resection after induction chemoradiotherapy in non-N2 patients. High rates of R0 resection have been reported in a large series of studies using a minimally invasive approach. In our case series, our R0 resection rate is compatible with the literature. Our only R2 case is a case of salvage surgery performed 5 months after a good response in an inoperable patient.
There is no clear guidance on how to choose the surgical approach based on preoperative radiological findings. The choice of surgical approach for Pancoast tumors depends on the experience of the center and the surgeon. For larger tumors (>7 cm), the value of the minimally invasive technique may be questionable due to limited visualization of tumor infiltration within the thoracic cavity caused by tumor size and overall reduced overview. 14 In addition, removal of the tumor en-bloc leads to a certain enlargement of the incision with the need for rib spreading, losing some of the benefits of the minimally invasive approach. Reconstruction of very large thoracic wall defects is also shown to be unsuitable for VATS techniques. 14 When we investigated whether the radiological analysis of the mass in the thorax CT evaluation in the preoperative period could be effective in the choice of the surgical method, we observed that thoracotomy was preferred at a statistically significant rate when the longest axis distance of the tumor invading the chest wall was over 77 mm. We believe that the need for mesh application to the chest wall after extensive resection limits the hybrid-VATS approach.
Although our study is retrospective, it is a recent study with a larger series compared with the studies in the literature comparing hybrid-VATS and thoracotomy. The pain scale, which is the most important parameter in the comparison of open and minimally invasive surgeries, was not analyzed in our study. On the other hand, the compliance of the hybrid-VATS technique with oncological principles has been demonstrated by perioperative findings and pathological data. No criteria have been defined for the selection of the surgical approach as open or VATS in Pancoast cases. The strongest aspect of the present study is the determination of the role of radiological findings in the choice of surgical method. Another parameter that stands out in the present study is the comparison of postoperative complications between both techniques, which is not seen in the studies in the literature. The prepared video is not a single case video, it is the result of editing many cases made in our center. We think that it is a detailed visual presentation for centers and teams who want to implement the hybrid-VATS technique.
Conclusion
Although the study limitation is the low number of cases, as a result of the developing experience in the field of minimally invasive surgery, hybrid-VATS has been successfully applied in superior sulcus tumors in inexperienced teams and centers. It is superior to an open approach with shorter operative time, less perioperative bleeding, and lower postoperative complication rates without compromising oncological principles.
Increasing the number of cases or conducting a meta-analysis with the results of other centers will create clear evaluations. We observed that open surgery was preferred only in cases of subclavian artery invasion, vertebral resection, and mesh use. Therefore, these criteria may be selection criteria for open surgery. The longest distance of the chest wall invasion area on preoperative thorax CT can be used as a criterion for the selection of thoracotomy or the hybrid-VATS method as a surgical approach in Pancoast tumors.
Footnotes
Authors’ Contributions
Conception and design: V.E., M.Ü., M.E.F., and E.Y.D. Administrative support: A.Ç., C.B.S., Y.S., and A.S.A. Provision of study materials or patients: V.E., Ö.İ., and M.M. Collection and assembly of data: M.Ü., E.Y.D., A.Ç., and C.B.S. Data analysis and interpretation: Y.S., A.S.A., Ö.İ., and M.M. Article writing: V.E. and M.Ü. Final approval of article: V.E., M.E.F., A.Ç., and E.Y.D.
Ethics Committee Approval
The study was approved by the ethics/scientific committee of Yedikule Chest and Thoracic Surgery Training and Research Hospital and was conducted in accordance with the principles of the Declaration of Helsinki; 2023-46028.12.2023.
Consent for Publication
A written informed consent was obtained from each patient.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
This research did not receive any specific grant from any funding agencies.