
Abstract
Background:
This study aims to compare the early outcomes of the surgeon-powered robotic uniportal subxiphoid resection technique with conventional uniportal techniques.
Methods:
A retrospective analysis was conducted on patients operated on for lung cancer between January 2022 and December 2023, comparing those who underwent uniportal lung resection with those who received the uniportal subxiphoid surgical technique.
Results:
Out of 90 patients in the study, 31 underwent subxiphoid resection while 59 underwent the uniportal surgical technique. When comparing the average lengths of hospital stay, the subxiphoid group had an average stay of 3.8 ± 1.2 days while the uniportal surgery group had an average stay of 4.8 ± 1.9 days (P = .004). At the 1-hour postoperative evaluation, the visual analog scale score for the subxiphoid group averaged 2.2 ± 1, while the uniportal surgery group averaged 3.2 ± 1.6 (P = .002). Complications were observed in four patients (12.9%) in the subxiphoid group and eight patients (13.5%) in the uniportal surgery group (P = .927).
Conclusion
: Uniportal subxiphoid video-assisted thoracoscopic surgery resections are safe and provide advantages such as less postoperative pain and shorter hospital stays for patients.
Introduction
With the advancement of technology, lung resections are increasingly performed with smaller incisions and minimally invasive methods. While video-assisted thoracoscopic surgery (VATS) lobectomy was first described in 1992, uniportal lobectomy was introduced in 2011. In comparison to thoracotomy, these contemporary methods have been demonstrated to improve the quality of life of patients and minimize early complications.1–3
Robotic technologies facilitate surgery by providing surgeons with almost limitless movement capabilities in confined spaces. 4 However, despite rapid advancements in robotic technology, many centers cannot utilize these tools due to costs. This situation has led to increased use of more accessible and cost-effective technologies. The introduction of multi-joint wristed instruments in thoracic surgery in 2020 marks a significant development. In the first study published on this topic, Trevis et al. 5 defined the technique as “surgeon-powered robotic surgery (sPRS)” due to the similar movements of these instruments. In our initial publication regarding these instruments, we noted that their lack of movement restrictions made them suitable for use in uniportal surgery by oncological principles. 6
All these technological advancements are progressively increasing thoracic surgeons’ interest in the uniportal approach. The lung resection technique described by Dr. Diego in 2011, 2 is now routinely used in many centers. However, even in video-assisted thoracoscopic or robot-assisted thoracoscopic surgical procedures performed from the intercostal space, patients may experience more pain. The subxiphoid resection technique was developed to prevent intercostal nerve damage. Although this technique does not damage the intercostal nerves, its technical challenges, the need for specific instruments, and difficulties in adhering to oncological principles are still discussed in the literature.
The aim of this article is to evaluate the early outcomes of the uniportal subxiphoid resection technique using Multi-Joint Wristed Instruments in comparison to conventional uniportal techniques, supported by literature.
Materials and Methods
Our study includes patients who underwent uniportal lung resection due to non-small cell lung cancer (NSCLC). Patients who underwent surgery for NSCLC from January 2022 to December 2023 were assessed retrospectively. Group A consists of patients who underwent uniportal lung resection while Group B includes patients who received the uniportal subxiphoid surgery supported by multi-joint wristed instruments. In our hospital, the subxiphoid resection technique has been applied by a single surgeon since 2021 for early-stage patients with tumor diameters of 4 cm or less. Uniportal surgery has been routinely preferred for patients undergoing VATS since 2018.
In the study, patients with neoadjuvant therapy and uniportal sleeve resection were not included. The study excluded eight patients who underwent multiportal VATS due to extensive adhesions in uniportal surgery and four patients who were converted to thoracotomy due to bleeding. In our study, subxiphoid resection was performed by a single surgeon. Subxiphoid resections are primarily preferred for early-stage tumors with a body mass index (BMI) of 30 and below. In our center, uniportal surgery is tried in all patients scheduled for VATS regardless of BMI, including locally advanced tumors. The surgeon performing the subxiphoid has experience with approximately more than 300 video-thoracoscopic lung resections.
Preoperative evaluation
Thoracic contrast-enhanced computed tomography (CT) was requested for all patients during preoperative evaluation. Patients with undiagnosed tumors of one cm or more underwent cranial magnetic resonance imaging with positive emission tomography-CT (PET-CT) to better evaluate distant metastases and mediastinal clinical staging. These tests provide an important basis for determining the spread of tumors and the stage of the disease.
Mediastinal lymph nodes are of great importance in the evaluation of malignancy. Therefore, invasive staging methods such as endobronchial ultrasonography and/or mediastinoscopy are applied to patients with mediastinal lymph nodes of 1 cm or more or positive findings in hilar or mediastinal lymph nodes on PET-CT and adenocarcinoma patients with tumor diameter of 3 cm or more. Pulmonary function tests and the diffusing capacity of the lungs for carbon monoxide tests were requested from the patients during preoperative evaluation. An electrocardiogram is performed for cardiac evaluation and echocardiography is performed when necessary.
The modified Charlson Comorbidity Index was used to evaluate the comorbidity of the patients. In all patients, surgical decisions were taken by the oncology council, a multidisciplinary team.
Surgical technique
In the conventional VATS technique, after a double-lumen endobronchial tube, patients are operated in the lateral decubitus position through a 5 cm utility incision. This incision is made anterior to the latissimus dorsi muscle through the 4th or 5th intercostal space. A 10 mm thoracoscope (Logic HD, Storz, Germany) was used to evaluate the pathology, adhesions, and diaphragmatic level within the thorax. Ultrasonic energy devices (Harmonic, Ethicon, USA) are used to resolve pleural adhesions. Lung resection was performed with thoracoscopic instruments, and endoscopic vascular and parenchymal staplers (EndoGIA, Covidien plc, Norwalk, USA) were used for resection.
In subxiphoid resections, patients are operated in a lateral position between 60 and 70 degrees. A 4 to 5-cm midline incision is made in the infrasternal space. After the adhesion of the rectus abdominis muscle in the subxiphoid region is separated, the infrasternal area is advanced with finger dissection. The right mediastinal pleura is opened and the thorax is accessed. Lung traction is provided with customized subxiphoid ovarian clamps and aspirators during resection. Wristed articulated instruments (ARTISENTIAL®, LivsMed) are used for the dissection of vascular structures. While the camera is placed on the top in subxiphoid resection, it is used with wristed articulated instruments by creating a pivot point for the instrument with an aspirator or subxiphoid over to provide a more controlled use (Fig. 1).
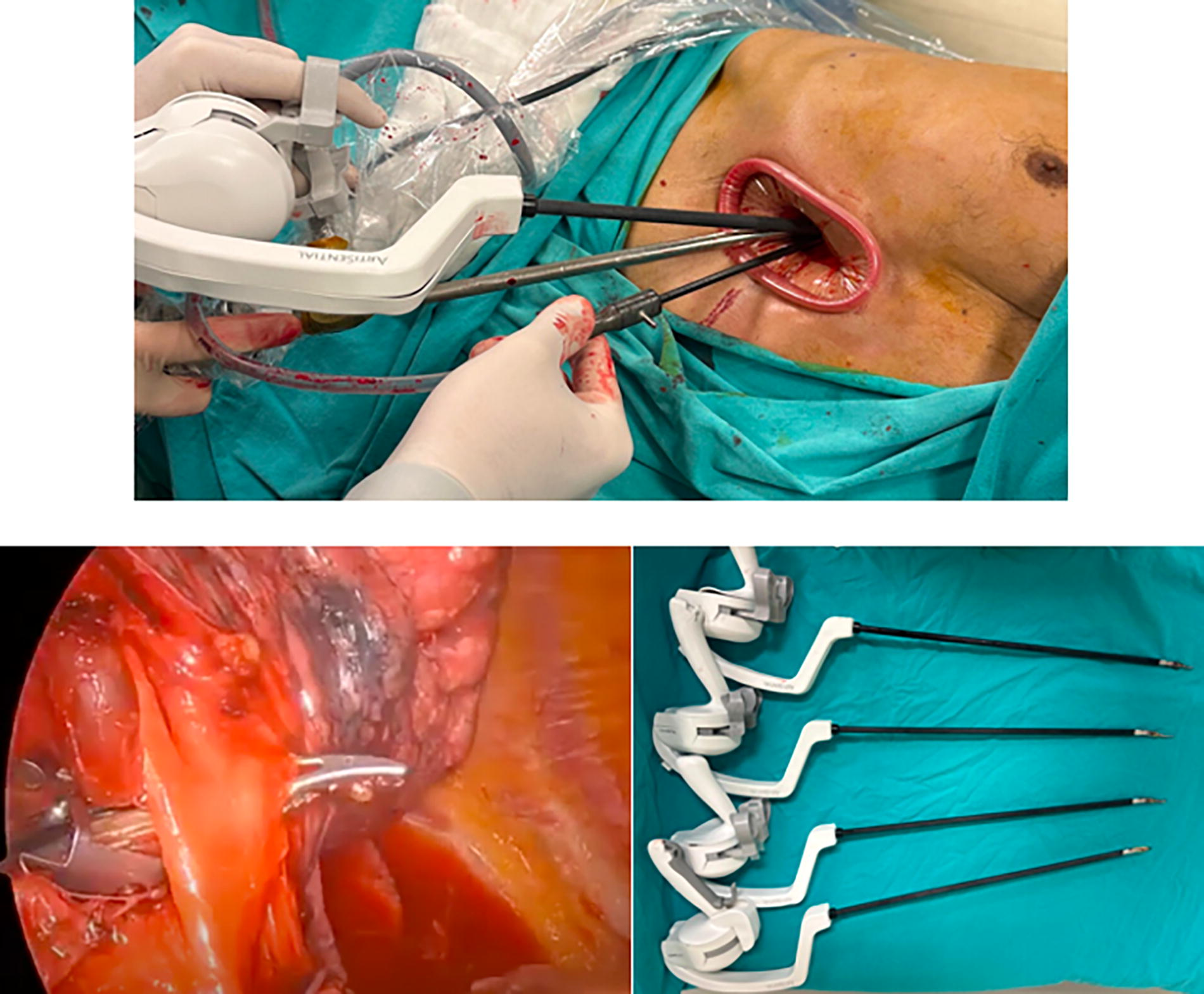
Perioperative images of subxiphoid resection and wristed articulated instruments.
Postoperative follow-up
Morbidities were considered as complications that occurred during hospitalization. Morbidities included pneumonia, respiratory failure, pneumothorax after drain removal, prolonged air leak (>7 days), infections requiring wound site revision, and postoperative hemorrhage.
In our study, a visual analog scale (VAS) routinely applied by nurses was used for postoperative pain assessment. It is routinely administered to all patients at the first hour in postoperative extubated patients. Patients were asked to give a score between 0 and 5. On the scale, a score of 0 represents no pain and a score of 5 represents the most severe pain.
Statistical method
Numerical variables were evaluated with mean ± standard deviation and median (min-max) and categorical variables were evaluated with number and percentage. Parametric test assumptions (normality and homogeneity of variances) were checked before comparing the groups in terms of numerical variables. Mann–Whitney U test was used to compare continuous variables. Survival analysis was performed using the Kaplan–Meier test. Statistical analyses were performed using IBM SPSS Windows 26.0. The significance level was taken as P < .05.
Results
Of the 90 patients included in the study, 31 underwent subxiphoid resection and 59 underwent uniportal surgery, the characteristics of the cases are detailed in Table 1. There were 26 (83.9%) males in the subxiphoid group and 41 (69.5%) males in the uniportal group; there was no statistical difference in the gender distribution between the groups (P = .104). The mean age was 61.7 ± 8.4 years in the subxiphoid group and 67.1 ± 8.1 years in the uniportal group, with a statistical difference in mean age between the groups (P = .010).
Characteristics of the Cases
CCI, Charlson Comorbidity Index; R, range; VAS, visual analog scale.
The bold parts in the table indicate that the p value is less than 0.05 and is statistically significant.
The mean BMI was 24.9 (range = 18–29) in the subxiphoid group and 27.1 (range 19–35) in the uniportal surgery group (P = .032). There was no statistical difference in smoking (box/year), FEV1 liter, and FEV1 percentage between groups (P = .500, .964, and .172, respectively). In the comorbidity evaluation, 14 (45.2%) patients in the subxiphoid group had comorbidities compared to 30 (51.7%) in the uniportal group (P = .881).
In the subxiphoid group, 28 (90.3%) patients underwent right-sided resection while 36 (61%) patients in the uniportal group underwent right-sided resection (P = .002). The mean operative time was 123 (range = 95–165) minutes in the subxiphoid group and 105 (range = 85–205) minutes in the uniportal surgery group (P < .001). When the mean length of hospitalization of the patients was compared, the mean length of hospitalization was 3.8 ± 1.2 days in the subxiphoid group and 4.8 ± 1.9 days in patients who underwent uniportal surgery (P = .004). When the pain in the first postoperative hour was evaluated, the mean VAS score was 2.1 ± 1 in patients undergoing subxiphoid surgery and 3.2 ± 1.6 in patients undergoing uniportal surgery (P = .002).
Twenty-five (80.6%) patients underwent lobectomy via the subxiphoid approach while 41 (69.5%) underwent lobectomy via the uniportal approach. Six (19.4%) patients underwent segmentectomy via the subxiphoid approach while 18 (30.5%) patients underwent segmentectomy via the uniportal approach (P = .211). The most common resection in the subxiphoid group was right upper lobectomy (n = 15, 48.4%) and the most common resection in the uniportal group was RUL (n = 14, 23.7%). Table 2 shows the resections performed in detail.
Forms of Resection
The mean number of lymph nodes removed was 10.1 ± 6.2. The mean lymph node station removed was 4.3 ± 1.4 The mean number of lymph nodes removed in subxiphoid resection was 10.1 ± 5.4 while the mean number of lymph nodes removed in uniportal surgery was 11.3 ± 6.5 (P = .446). Of the operated patients, 59 (65.6%) had adenocarcinoma, 21 (23.3%) had squamous cell carcinoma and 10 (11.1%) had other carcinomas. No statistical difference was found when the groups were compared (P = .130). When tumor diameters were compared, the mean tumor diameter was 2.8 ± 1.1 cm in patients undergoing subxiphoid surgery and 2.4 ± 1.5 in patients undergoing uniportal surgery (P = .050). The results of the pathology evaluation are shown in detail in Table 3.
Pathology Evaluation
The bold parts in the table indicate that the p value is less than 0.05 and is statistically significant.
According to survival analysis, 12-month and 24-month survival rates were 96.8% and 96.8% in the subxiphoid group, while 98.3% and 94.1% in the uniportal group (P = .788, Fig. 2).

Survival analyses in the subxiphoid group and uniportal group.
Complications were observed in 4 (12.9%) patients in the subxiphoid group compared to 8 (13.5%) patients who underwent uniportal surgery (P = .927). In two of the patients who underwent subxiphoid resection, blood pleurodesis was performed because the prolonged air leak did not resolve spontaneously. One patient had a wound infection. Antibiotic treatment was also administered in one patient due to postoperative pneumonia.
Prolonged air leaks occurred in six patients who underwent uniportal surgery. Two of these patients had spontaneous leakage cessation while three patients underwent blood pleurodesis. In one patient, re-operation was performed because the leaks did not improve. Upon detection of leakage from the stapler lines, it was sutured and revised. Vacuum-assisted closure was applied to the patient due to postoperative wound infection. In addition, atrial fibrillation requiring medical treatment occurred in one patient who underwent uniportal surgery and pneumonia occurred in the early postoperative period in one patient. No postoperative mortality occurred in any patient.
Discussion
In the literature, there are limited publications on sPRS in the field of thoracic surgery. Most of the publications on this technique exist only in the form of case reports. In our first published series, sPRS was compared with conventional VATS techniques in NSCLC. Since no difference was observed in terms of early complications and hospitalization times, it was concluded that this technique is appropriate in oncological aspects and can be applied effectively due to the absence of mobility limitation. 6
The biggest difficulty in the subxiphoid approach is the compression of the instruments and very little mobility. In subxiphoid resections, posterior resections such as posterior segment and lower lobe superior are performed more difficult than the uniportal approach. 7 Because of these technical difficulties, Pfeuty et al. 8 described multiportal subxiphoid techniques in the literature due to the rigidity of subxiphoid instruments. In our study, most of the resections were on the right side. The most important reason for this is that the technique becomes more difficult to perform in left-sided resections due to the greater limitation of movement of the instruments and the higher risk of cardiac compression and arrhythmia. 9 Multi-joint wristed ınstruments facilitate the operation in right-sided resections due to the elimination of movement restriction but do not eliminate compression in left-sided resections. Therefore, right-sided resections were observed more frequently in our study.
In a meta-analysis study conducted by Mei et al. in 2022, it was reported that the subxiphoid approach could be applied in 44.1% of cases. 10 In the meta-analysis study conducted by Song et al., which had a high number of patients, it was observed that the average operation time was 164 minutes in the subxiphoid group. In our study, similarly, the operation time was longer in the subxiphoid group, averaging 123 minutes. In terms of the pain scale, in the study of Song et al., 11 significantly less pain was observed in the subxiphoid group at the 8 hours and on the first, second, and third postoperative days. Similarly, less pain was found in the subxiphoid group in our study. In terms of hospitalization duration, no difference was found in the study of Song et al., whereas in our study, the hospitalization duration of the subxiphoid group was found to be significantly shorter.
In their study on subxiphoid segmentectomy, Abdellateef et al. 12 stated that this approach provided faster recovery and improved the quality of life of patients compared to the conventional technique. It has also been reported that complications decrease with increasing experience in the subxiphoid approach and the number of dissected lymph nodes will increase after 150 cases. Cai et al. 13 reported a complication rate of 14.8% in the subxiphoid approach and 9.3% in intercostal surgical approaches (P = .37). In our study, similar to the literature, 12.9% complications were observed in patients undergoing subxiphoid resection and 13.5% in patients undergoing uniportal surgery. Moreover, early pain scores showed better results in patients who underwent subxiphoid resection. However, the biggest challenge in subxiphoid resections is the management of major bleeding. Bleeding cannot be controlled as easily as with the intercostal technique. In cases where bleeding cannot be controlled by suturation or compression, secondary intercostal port opening or conversion to thoracotomy may be necessary. Because even if intercostal ports are opened, the control of the area may not be sufficient.12,13
Liu et al. mentioned that systemic lymph node dissection was difficult with subxiphoid incision and stated that they performed only mediastinal lymph node sampling in the case they presented. 14 Song et al. performed mediastinal lymph node sampling or dissection in 77 patients with primary lung carcinoma. No lymph node sampling or dissection was performed in the group with benign or in situ frozen results. While 8.04 ± 3.68 lymph nodes were sampled in the subxiphoid group, 7.87 ± 3.5 lymph nodes were sampled in the intercostal group and there was no significant difference between the groups in terms of lymph node dissection (P = .420). Although there were initial difficulties in mediastinal sampling, they stated that with the technique becoming established, they improved in lymph node dissection to the same level as the uniportal technique. 11 In our study, 10.1 lymph nodes were removed in the subxiphoid group and 11.3 lymph nodes were removed in the uniportal group with no difference between the groups (P = .662). As mentioned in the study by Song and colleagues, as progress is made with the subxiphoid technique, mediastinal lymph node dissection can be performed more optimally.
The subxiphoid approach provides more optimal conditions for right-sided localization. When we retrospectively evaluated cases, we preferred the right approach in 90.3% of subxiphoid cases. Similarly, the increase in BMI makes the subxiphoid approach difficult. Although we did not have any definite preoperative selection indications, we observed that we preferred lower BMI in the subxiphoid group in the retrospective review. While the BMI in the subxiphoid group was 24.9, it was 27.1 in the uniportal group, and there was a statistical difference between the groups.
Multi-joint wristed instruments are also used by other departments due to their ease of use. They are also used in gynecology and general surgery.15,16 It is obvious that the results will be analyzed better with increasing studies.
Limitations
The retrospective nature of our study brings certain limitations. In addition, the small sample size makes it difficult to generalize the results and reduces the power of statistical analyses. Moreover, the fact that the subxiphoid resection procedures were performed by only a single surgeon introduces potential bias in the study.
Conclusion
Subxiphoid uniportal VATS lobectomy is safe and there is an opportunity to perform surgery by oncologic principles. It provides patients with less postoperative pain and a shorter hospitalization period.
Footnotes
Authors’ Contributions
C.B.S. and M.Ü.: Conception and design, data analysis and interpretation, article writing. Ö.S. and M.M.: Administrative support. C.B.S. and M.V.D.: Provision of study materials or patients. O.B. and D.K.: Collection and assembly of data. C.B.S., C.A., and M.M.: Final approval of article.
Ethics Committee Approval
The study was approved by the ethics/scientific committee of Yedikule Chest and Thoracic Surgery Training and Research Hospital and was conducted in accordance with the principles of the Declaration of Helsinki.
Consent for Publication
A written informed consent was obtained from each patient.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
This research did not receive any specific grant from any funding agencies.