
Abstract
Background:
Extrathoracic congenital lung lesions (CLLs) are a rare anomaly of lung development. Management and surgical approach are variable. We present our institutional experience with extrathoracic CLLs for the past 18 years.
Methods:
We retrospectively reviewed all patients younger than 18 years diagnosed with a CLL from January 2005 to June 2023. Only patients with suspected extrathoracic CLLs on prenatal imaging were included.
Results:
A CLL was identified in 381 patients and was extrathoracic in 25 patients (6.6%). Six patients (24%) with other congenital anomalies were excluded, and 3 were lost to follow-up. The prenatal course and delivery of the 16 study patients were unremarkable and all were asymptomatic. Larger lesions, both prenatally and postnatally, were more likely to undergo surgical resection (11.8 ± 8.2 cm3 versus 3.9 ± 3.3 cm3, P = .05; 6.1 ± 5.1 cm3 versus 2.5 ± 2.5 cm3, P = .10, respectively). Seven patients (7/16; 44%) underwent resection—5 thoracoscopic and 2 laparoscopic. Thoracoscopic transdiaphragmatic approach was favored for lesions extending >50% above the diaphragm. Five lesions were intradiaphragmatic, one infradiaphragmatic, and one intrathoracic. Four lesions (4/7; 57%) were hybrid lesions on pathology. No malignancy was identified. Nine patients (9/16; 56%) underwent surveillance. Imaging modality for surveillance varied. Duration of follow-up ranged from 0.5 to 83 months.
Conclusions:
We provide the largest case series to date describing both operative and nonoperative management of extrathoracic CLLs. Surveillance appears to be appropriate for small lesions. If surgical excision is pursued, the thoracoscopic approach is safe and preferred if diaphragmatic involvement is suspected.
Introduction
Congenital lung lesions (CLLs) are a rare lung pathology with an estimated incidence of 4.15 in 10,000 births. 1 CLLs encompass various types of malformations, the most common being congenital pulmonary airway malformations (CPAMs), bronchopulmonary sequestration (BPS), congenital lobar emphysema, and bronchogenic cysts. The advancement and more ubiquitous use of prenatal imaging have led to increased antenatal identification of CLLs, including the even more uncommon extrathoracic CLL. 2 Extrathoracic CLLs are estimated to occur at an incidence of less than 2 in 1 million. 3 The paucity of data surrounding extrathoracic CLLs underscores the existing controversy for best management options of these mostly asymptomatic lesions. In addition, their intra- and infradiaphragmatic location presents a unique challenge when planning resection. We present our institutional experience with extrathoracic CLLs, including and evaluating both cases managed operatively and nonoperatively, with the goal to provide additional narrative on the guidance and management of these rare lesions.
Patients and Methods
Data collection
A single-institution retrospective review of all patients younger than 18 years diagnosed with a CLL from January 2005 to June 2023 was conducted at a quaternary care children’s hospital. Data were collected in accordance with the Declaration of Helsinki as revised in 2013 and following Institutional Review Board (IRB AAAR4058). Waiver of consent was obtained. All patients with suspected extrathoracic CLLs on prenatal ultrasound reports were evaluated. Any with associated congenital anomalies were excluded. Patient demographics, prenatal, postnatal, and operative course were obtained from clinical records. Postnatal data included Apgar scores at 1 and 5 minutes, need for ex-utero intrapartum (EXIT) procedure, or respiratory complications at birth (e.g., need for oxygen or ventilatory support). Prenatal lesion size was determined from 2D ultrasound reports, and the CPAM volume ratio (CVR) was calculated as described by Crombleholme et al. in 2002. 4 A board-certified pediatric radiologist with 11 years of experience (M.L.) reviewed and verified postnatal cross-sectional images regarding the size and location of the extrathoracic CLL. Diaphragmatic irregularity or bulging of the diaphragm was defined as a deviation of the outline of the diaphragm from its expected contour on imaging (Fig. 1). A retrospective assessment of all preoperative imaging was performed to quantify the extent of diaphragm bulging. Lesion was characterized as follows: >50% of the lesion above the level of diaphragm or >50% of the lesion below the level of diaphragm.
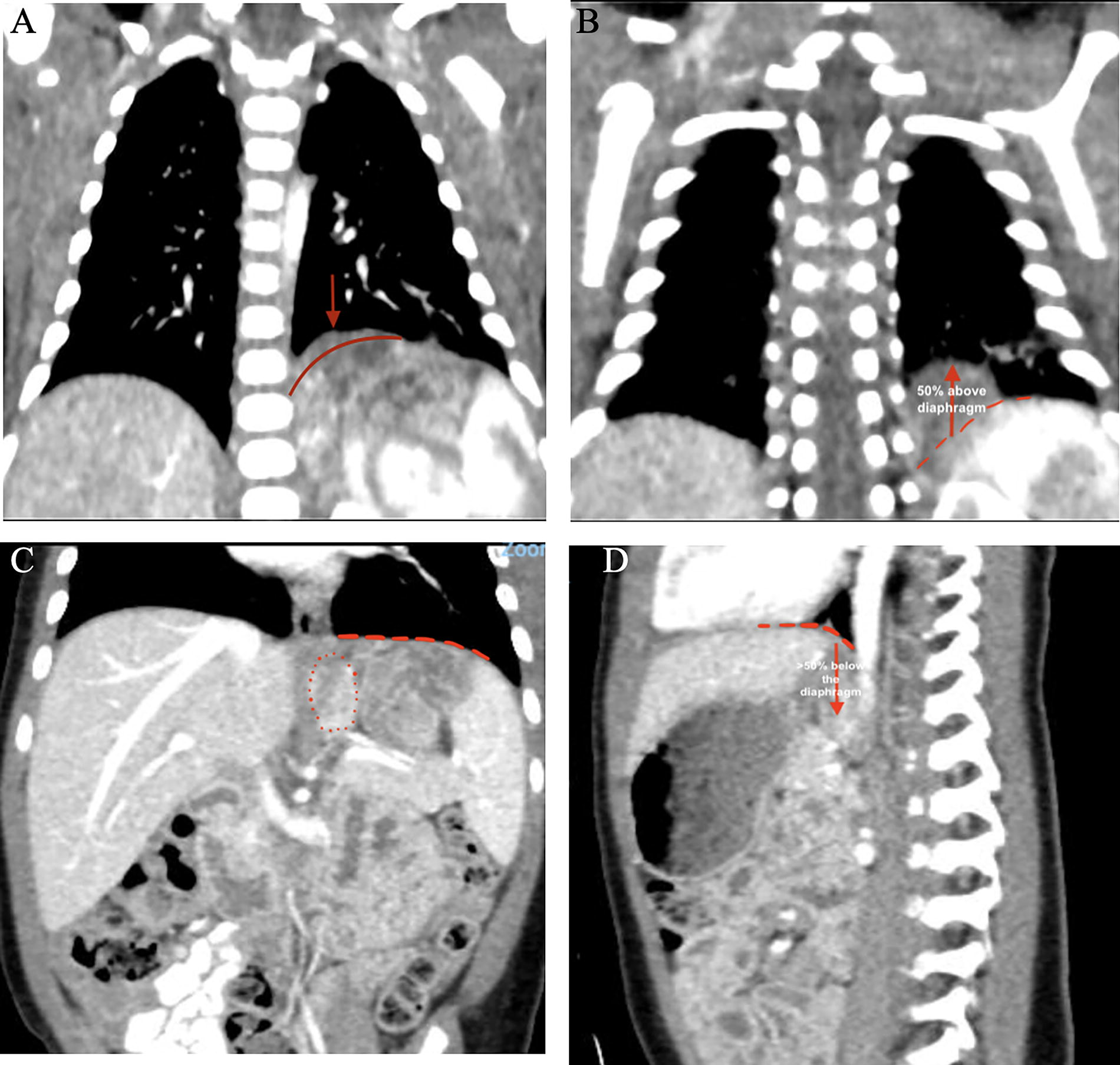
Computed tomography (CT) imaging of extrathoracic congenital lung lesions.
Operative methods
Based on preoperative evaluation, lesions that met the criteria underwent a thoracoscopic approach for resection. A standard 3-port technique was utilized, allowing for one 4 mm camera port, one 3 mm working port, and a third 3–5mm working port. Following entry into the thoracic cavity, the intrathoracic cavity and contents were examined. The intradiaphragmatic lesions were noted as a bulge within the diaphragm, most commonly in the posteromedial diaphragm. To access the mass, the diaphragm was incised just superior to the mass by incising the pleura and spreading the muscle fibers until the mass was revealed. The mass was then dissected circumferentially from surrounding structures and adhesive tissue using a combination of cautery (3 mm laparoscopic vessel sealer; CoolSealTM [previously JustRightTM]; Hologic®; Louisville, Colorado, United States) and blunt dissection. Feeding vessels were sealed or doubly clipped if they were too large to be sealed. Most diaphragmatic defects were not full thickness and were closed with interrupted 2–0 Ti-CronTM (Medtronic; South Africa) sutures. The mass was removed in a specimen bag through a port site that was extended if needed.
Data analysis
Data were summarized using descriptive statistics (Microsoft Excel 2023 and RStudio 2023). Average with standard deviation was used for normal data and median with range or interquartile range for non-normal data. The Kruskal–Wallis test was used for univariate analysis of non-normal continuous variables and Welch’s t-test or analysis of variance, as appropriate, for normal data. The Fisher’s exact test was used for analysis of categorical variables.
Results
We identified 381 patients diagnosed with a CLL over an 18-year span at our institution. The CLL was noted to be in an extrathoracic location in only 25 patients (6.6%). Six patients (6/25; 24%) were excluded due to other associated congenital anomalies, including congenital diaphragmatic hernia (5/25; 25%) and right diaphragm eventration with omphalocele and skeletal abnormalities (Fig. 2). One patient had a small ventricular septal defect on fetal echocardiogram, all others’ ECHOs were normal. Three additional patients were excluded due to loss to follow up after initial prenatal consultation and majority of clinical care taking place at an outside institution. All remaining patients included in the study had isolated extrathoracic CLLs (n = 16) except for one who had a concomitant intrathoracic CPAM that was resected and did not impact our clinical decision-making for the extrathoracic lesion.
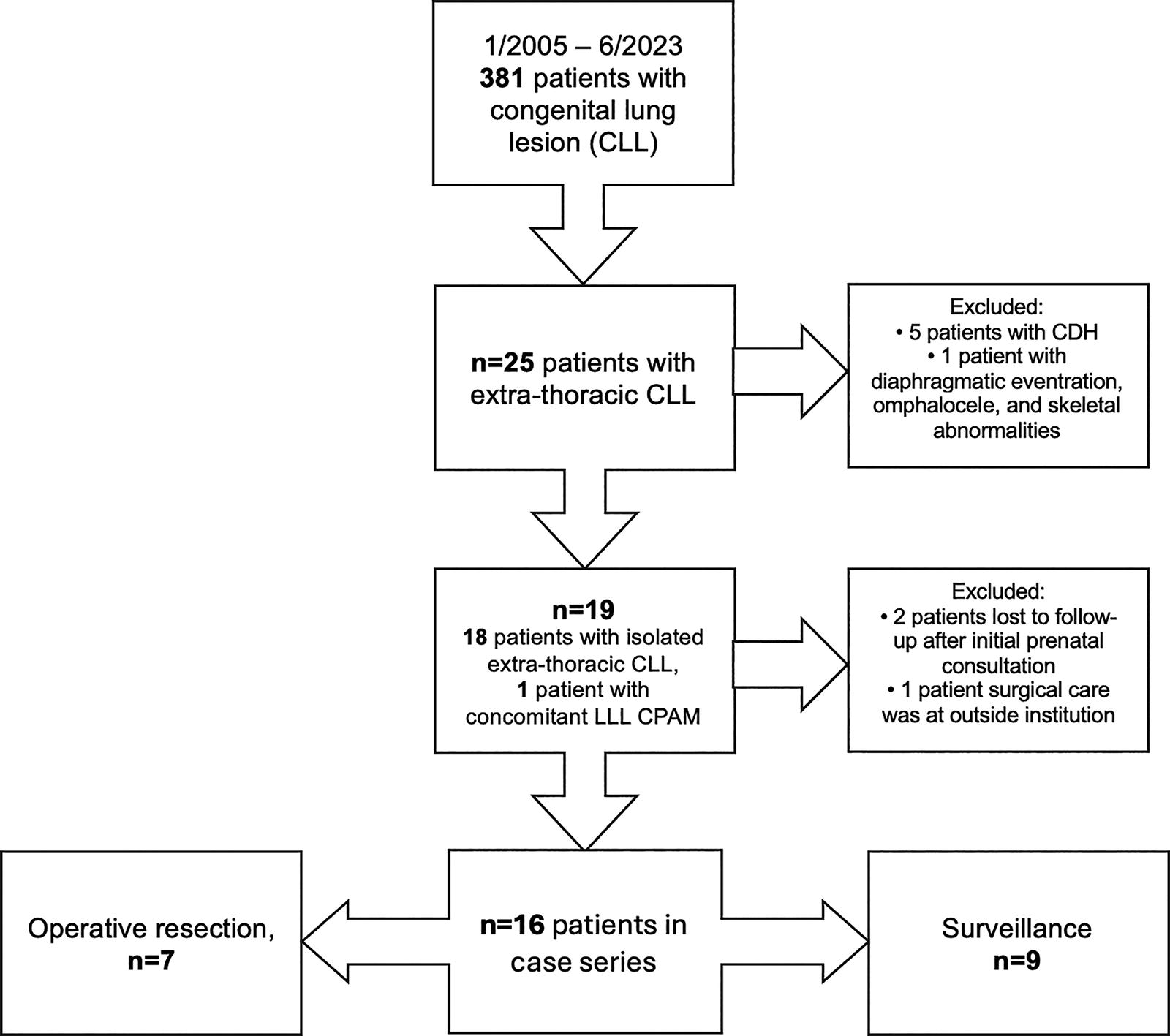
Flowchart of patients included in the study.
All extrathoracic CLLs were detected on prenatal ultrasound at a median gestational age (GA) of 22.4 weeks and in similar proportions of males and females (Table 1). There were no prenatal complications, including hydrops necessitating steroid administration or fetal intervention.
Baseline Patient Characteristics, N = 16
At birth, all were full term and of normal birth weight (BW) (median BW 3055 g [range: 2495–4190 g]. The majority of patients were inborn, however, no neonates required respiratory interventions. Although a majority of patients (56%) received chest X-rays at birth, only two demonstrated any findings that were subtle and nonspecific. All patients did undergo postnatal imaging with computed tomography (CT) scan, magnetic resonance imaging (MRI), or ultrasound. Table 2 compares differences in characteristics of lesions that were resected versus surveilled. Lesions that were surgically resected were larger, with higher prenatal maximum CVR and larger prenatal and postnatal size dimensions. The majority of these resected lesions also exhibited an overall growth in size from initial diagnosis.
Characteristics of Lesions Undergoing Operative Resection Versus Surveillance
SD = standard deviation.
IQR = interquartile range.
Inclusive of one ultrasound measurement.
Patients who underwent surveillance had more diagnostic certainty, despite the intra-abdominal location of the lesion. Most were noted to have a pathognomonic feeding vessel and either a mixed or solid, rather than cystic, appearance. Clear tissue plane between the lesion and kidney or adrenal on imaging was also suggestive of extrathoracic BPS rather than other types of abdominal masses such as adrenal hemorrhage, neuroblastoma, and diaphragmatic anomaly.
Seven patients (44%) underwent surgical resection (Table 3). All were approached through minimally invasive techniques—five patients underwent thoracoscopic resection (71%) and two patients underwent laparoscopic resection (29%). The majority of the lesions (71%) were noted to be intradiaphragmatic. Retrospective assessment of extent of bulging of the diaphragm and location of the majority of the lesion (>50% above or below diaphragm) correlated with operative approach in all but one patient. Lesions that caused bulging of the diaphragm prompted a thoracoscopic approach unless most of the lesion was felt to be below the level of the diaphragm. Median age at resection (7.2 months) was slightly older than the typical range of four to six months. No patients were symptomatic. The most common indications for surgical resection were to confirm diagnosis and prevent growth of the mass. The average operative time for thoracoscopic approach was shorter than that of laparoscopic. There were no postoperative complications.
Patients Who Underwent Operative Resection, n = 7
BPS, bronchopulmonary sequestration; Hybrid, hybrid lesion, combination of CPAM and BPS elements.
The final pathology of the resected CLLs indicated that four lesions (57%) were hybrid lesions with CPAM two elements. The other three lesions (43%) were BPS. No malignancy was noted in any of the resected lesions. Following resection, two patients required continued surveillance due to possible residual mass or diaphragm eventration on follow-up CT. Neither has had repeat surgery during the median follow-up time of 0.8 months [range: 0–61.2 months].
Surveillance without operative resection was pursued in nine patients (56%). This management strategy was based on the small size of extrathoracic CLL, absence of symptoms, collaborative decision-making with the parents (Table 4). Length of follow-up and imaging modality for surveillance was variable. On postnatal imaging, two extra-thoracic lesions spontaneously regressed within the first three months after birth and did not necessitate further imaging. Other patients underwent repeat imaging typically at yearly intervals. Three were eventually lost to follow-up, one of which had completed a malignancy workup with negative urine catecholamines before loss of follow-up. Three patients were still undergoing active surveillance, with further imaging pending. All lesions undergoing surveillance have either remained overall stable in size or decreased. No patients in the surveillance group became symptomatic or ended up undergoing surgical resection.
Patients Who Underwent Surveillance Without Operative Resection, n = 9
BPS = bronchopulmonary sequestration.
HVA/VMA = homovanillic acid/vanillylmandelic acid for workup of neuroblastoma.
Part of follow-up at outside institution.
CT abd = computed tomography scan of abdomen.
MRI = magnetic resonance imaging.
CXR or Abd XR = chest X-ray or abdominal X-ray.
Discussion
Extrathoracic CLLs are much rarer, and the usual reported risks of complications associated with intrathoracic CLLs do not necessarily apply. Consequently, there is notable variability in clinical management, and there remains a lack of clinical guidelines. 5 We present the largest, most contemporary study of extrathoracic CLLs and provide our institutional experience and management practices.6–8
All extrathoracic CLLs at our institution were diagnosed prenatally as early as 18 weeks and 5 days of GA. No patients developed any complications such as hydrops necessitating steroids, need for fetal intervention (e.g., shunt, fetal surgery, or EXIT procedure), or fetal death. The extrathoracic location of these CLLs and small CVRs—all <1.0—most likely play a role in these observations. 4 Similarly, no patients experienced respiratory complications at birth—all were delivered uneventfully at term with normal median BW and Apgar scores. These birth outcomes also include outborn patients. Following multidisciplinary discussion with MFM and pediatric surgery teams and family, our observations suggest the possibility of delivery at local community centers, for these extrathoracic lesions that do not have certain high-risk factors. 9
Advocates for the resection of asymptomatic CLLs state the following reasons for surgery: prevention of cyst rupture and pneumothorax, prevention of infection with pneumonia, prevention of malignant transformation, and contribution to compensatory lung growth by removing nonfunctional, space-occupying lung tissue.10–13 However, extrathoracic CLLs, unlike intrathoracic CLLs, do not place patients at risk of pneumothorax, nor do they occupy space in the chest to affect lung growth. Due to the lack of effect on lung growth, early resection of extrathoracic CLLs does not appear to play the same therapeutic role of allowing for compensatory lung growth. Their risk of infection is thought to be very low given the lack of airway communication and additional lack of contact of extrathoracic CLLs with adjacent lung tissue through the pores of Kohn, however, the incidence of infectious complications is not well documented. Only one study reported an infection rate of 16% for intradiaphragmatic CLLs, but this was on a pathology-based, and not clinical, definition and was unable to determine an infection rate for infradiaphragmatic lesions. 14 The risk of malignancy and malignant transformation of extrathoracic CLLs is also poorly described in the literature. Relevant reports include an esophageal duplication cyst with associated CPAM type 3 elements and BPS that was noted to harbor a benign teratoma and observations of rhabdomyomatous dysplasia or KRAS-mutated cells in intra- or peri-diaphragmatic lesions.8,15 The significance of rhabdomyomatous dysplasia or even the possible presence of KRAS-mutated cells is unclear.8,16,17 No malignancy was noted on the final histopathologic evaluation of resected lesions.
Prevention of these complications, along with the concern for growth, was also considered for the seven patients who underwent surgical resection. Resection to prevent growth would prevent compressive digestive and respiratory symptoms from extrinsic compression and/or vagal nerve irritation with parasympathetic dysfunction.7,14,18 This is an important consideration because operative lesions were more likely to exhibit overall growth from initial diagnosis and were also larger. This finding is in line with the literature on intrathoracic lesions correlating increased lesion size and higher prenatal CVR with eventual surgical resection, which at times were indicated due to the development of complications such as pneumonia.11,19 However, all patients in our study were asymptomatic and the main motivator for early resection appears to be for diagnostic purposes. This highlights the diagnostic uncertainty and difficulty in localizing these lesions.6,20
Cross-sectional imaging by either CT or MRI is typically performed postnatally to further evaluate the lesions and for potential operative planning. Imaging features pertinent to surgical planning were discussed during retrospective pediatric radiologist review to develop our proposed algorithm (Fig. 3). Localization of the lesion to mostly above or below the diaphragm and involvement of the diaphragm facilitated operative planning. Lesions that are >50% above the diaphragm and bulging, or irregular contour of the diaphragm suggesting an intradiaphragmatic component of the lesion, should prompt a thoracoscopic approach (Fig. 1A, B). With >50% of the lesion above the diaphragm, it is expected that a clear bulge of the diaphragm will be visualized during thoracoscopy, indicating the location of the mass. The diaphragm can be safely opened in this area to reveal the lesion, thus preventing a significant intra-abdominal dissection. Intrathoracic access for a transdiaphragmatic approach to resecting the lesion may be technically more straightforward than an intra-abdominal approach, which requires dissection around the hiatus and possibly posterior to the stomach along vital retroperitoneal structures. If there is no diaphragm irregularity or more than 50% of the lesion extends below the diaphragm, a laparoscopic approach may be advantageous (Fig. 1C, D). Our proposed framework for extrathoracic CLLs of determining diaphragmatic involvement on imaging to decide surgical approach correlates with our operative findings (Fig. 3 and Table 3). No resection required dual cavity exploration and no significant postoperative complications were observed.

Radiological considerations for determining surgical approach. Our proposed algorithm that takes into consideration the presence and extent of intradiaphragmatic involvement to facilitate surgical planning.
Both the absence of symptoms and low potential risks of complications should be taken into account when considering surgical resection versus surveillance. 21 Surveillance of these lesions takes into account the degree of diagnostic certainty and individual lesion characteristics and behavior—it is a case-by-case shared decision based on clinical presentation, radiological data, along with physician judgment and parental preference. The important role of radiological imaging is again emphasized, given the absence of histopathologic evaluation of lesions undergoing surveillance. Smaller lesions, usually less than 3 cm, with the presence of a feeding vessel and minimal cystic components as well as well-defined margins delineating separation from the ipsilateral kidney, adrenal, and other retroperitoneal or intra-abdominal structures, lend more diagnostic certainty.22–24 With the presence of a feeding vessel, pleuropulmonary blastoma can usually be ruled out, and surveillance of a likely small BPS appears to be appropriate.25,26 The average size of the extrathoracic CLLs undergoing surveillance was small (2.5 cm3), and a feeding vessel was identified in all lesions except for the right-sided extrathoracic CLL, for which its location made delineation of vasculature more challenging.
There is a lack of clinical recommendations and standardization in both the type of imaging and duration of surveillance for extrathoracic CLLs. CT has a higher spatial resolution, decreased respiratory motion artifact, and is superior for evaluating lung parenchyma and detecting associated vasculature. However, its value is offset by its exposure to ionizing radiation. MRI offers no ionizing radiation exposure, but it is associated with the need for sedation of younger children.27–29 The initial postnatal characterization of the lesion is most important as it is utilized in the decision-making to pursue surveillance versus operative resection. The use of CT is supported as the most definitive modality for diagnosis.30,31 The choice of follow-up imaging is variable as it can be tailored depending on lesion characteristics, the patient, parental, and clinician preference, and resource availability. If detectable on ultrasound, following initial postnatal CT, surveillance ultrasounds are preferred to avoid additional radiation exposure. Surveillance visits with repeat imaging are usually at 12-month intervals to monitor for clinical symptoms and lesion size. Expert review suggests that surveillance may be considered complete once lesions have spontaneously regressed or have decreased or remained stable in size for at least five years.32,33
Our study cohort is the largest to date, describing our experience managing extrathoracic CLLs both operatively and nonoperatively over a span of almost two decades. Although this is a long study period, there has not been a significant institutional change in our approach to care of these patients and there remains a lack of clinical management guidelines. Our single-institution findings are limited by a small sample size and limited follow-up data. However, our study and institutional experience provide important additional narrative to the limited literature. Larger, multicenter studies are needed to evaluate existing clinical practices and better understand the natural history of extrathoracic CLLs to establish evidence-based clinical management guidelines.
Conclusions
For larger extrathoracic lesions and those demonstrating growth, it may be prudent to resect them similar to the management of intrathoracic CLLs. Radiological imaging is integral for guiding operative approach. For lesions with >50% reported above the diaphragm and suspected intradiaphragmatic involvement, the thoracoscopic approach appears safe and preferable. Surveillance may be an appropriate approach to consider for smaller extrathoracic CLLs, especially if there are no symptoms and radiological data support a diagnosis of extrathoracic CLL.
Footnotes
Authors’ Contributions
Y.S.W.: Methodology, investigation, data curation, analysis, writing—original draft, and visualization. J.G.: Data curation, investigation, visualization, and analysis. N.S.: Data curation, analysis, and writing—original draft. C.N.: Data curation and writing—original draft. M.C.L.: Methodology, validation, supervision, and writing—review and editing. V.P.D.: Conceptualization, methodology, validation, investigation, visualization, supervision, and writing—review and editing.
Disclosure Statement
M.C.L. reports a relationship with GE Healthcare that includes consulting or advisory. M.C.L. reports a relationship with Carestream Health, Inc., that includes board membership.
Funding Information
This study was not supported by any sponsor or funder.