
Abstract
Background:
The Da Vinci single-port (SP) platform is being used more frequently in radical prostatectomy (RP). In this study we aimed to compare the complications and oncological outcomes of the Da Vinci SP platform in robotic-assisted radical prostatectomy (SP-RARP) between elderly and young age-groups and to further examine differences between young-old and old-old patients.
Materials and Methods:
Data from 193 patients who underwent SP-RARP between December 2018 and June 2024 were analyzed. Patients were categorized into two age-groups: young (18–64 years) and elderly (65+ years). The elderly group was further divided into young-old (65–69 years) and old-old (70+ years) subgroups. The analysis considered variables related to patient characteristics, intraoperative outcomes, complications, and postoperative oncological outcomes.
Results:
The median age of the patients at the time of surgery was 64 (9.5) years. The intraoperative complication rate of 1.6%, with no cases requiring conversion to open surgery. The overall incidence of postoperative adverse events was 24.4%, and the 30-day readmission rate was 11.4%. Intraoperative complications and 30-day readmission rates were similar between groups (P = .593 and P = .821, respectively), while the postoperative complication rate was significantly higher in the younger patient group (P = .012). The median length of hospital stay (LOS) was 7 (22) hours and 110 (57%) patients were discharged on the same day (SDD). LOS and SDD rates were similar between groups (P = .389 and P = .529, respectively). The 3-year and 5-year biochemical recurrence (BCR)-free survival rates were 80.5% and 75.1%, respectively. The BCR-free survival rates were similar between both young and elderly patients and between the young-old and old-old groups (P = .751, P = .765, respectively).
Conclusion:
SP-RARP is a feasible option for elderly patients, delivering acceptable oncological outcomes with a low incidence of postoperative complications.
Introduction
Prostate cancer (PCa) is one of the most common cancers in adult males, with a rising global incidence.1,2 The widespread use of prostate-specific antigen (PSA) screening and increased life expectancy are considered contributing factors to this rise. Nonetheless, the vast majority of cases are detected at a localized stage. 3
Minimally invasive surgery is becoming more widespread globally, gradually replacing the open approach in radical prostatectomy (RP) with robotic-assisted surgery. 4 Among robotic platforms, the Da Vinci single-port (SP) (Intuitive Surgical Inc., Sunnyvale, CA) system has gained popularity, and SP robotic-assisted radical prostatectomy (SP-RARP) has become increasingly practiced by urologists. The SP system features several unique characteristics, including a slim design, articulating robotic instruments operated through a multichannel SP and a confined surgical workspace accessed through a single incision.
It is known that advancing age is a significant risk factor for postoperative complications and mortality. 5 While studies have compared outcomes of multi-port RARP (MP-RARP) between elderly and younger patients, no published studies exist for SP-RARP.6,7 In this study, our objectives were to compare SP-RARP outcomes between elderly and younger patient groups and to further explore the differences between young-old and old-old patients. To the best of our knowledge, this is one of the largest series reported by a single surgeon for this age-group.
Materials and Methods
An electronic database of hospital records (Epic system®) for individuals who had RP was retrospectively evaluated. The study included all consecutive patients undergoing SP-RARP at our institution between December 2018 and June 2024. The surgical technique applied for SP-RARP has been previously described by us. 8 The choice between transperitoneal and extraperitoneal approaches was based on surgeon preference. Patients who had salvage prostatectomy or additional surgical procedures in the same session were excluded due to differing postoperative courses compared with those who only underwent SP-RARP. This study adhered to the ethical principles outlined in the Declaration of Helsinki for medical research involving human subjects. Approval from the Institutional Review Board was obtained (IRB: STUDY2017–0152).
The patients were divided into three groups according to the D’Amico risk classification: low, intermediate, and high. 9 The Clavien–Dindo classification was utilized to evaluate 30-day postoperative complications and were categorized as major (Clavien–Dindo grades 3–5) and minor (Clavien–Dindo grades 1–2). 10 The American Society of Anesthesiologists (ASA) score was used to assess the general health status of patients in the preoperative period. Patients with ASA scores of 3–4 were categorized as high risk, while those with scores of 1–2 were classified as low risk. The International Society of Urological Pathology (ISUP) grade group system was used in the evaluation of biopsy and final pathology results. In the definition of biochemical recurrence (BCR), a serum PSA level of ≥0.2 ng/mL on two consecutive measurements during the follow-up period was accepted.11,12 Patients who were initiated on adjuvant therapy were not considered to have a BCR.
The patients were divided into two groups based on age: the young (18–64 years) and the elderly (65+ years). Those older than 65 years were further categorized into two subgroups: young-old (65–69 years) and old-old (70+ years). Age-groups were compared in terms of race, body mass index (BMI), ASA score, preoperative PSA level, biopsy ISUP cancer grade, D’Amico risk classification system, surgical approach (transperitoneal or extraperitoneal), operative time including in-room and procedure time (minutes), estimated blood loss (EBL), complications including intraoperative, postoperative and major postoperative complication rates, pathological outcomes, same-day discharge (SDD), length of hospital stay (LOS) (hours), readmission rates, BCR, and BCR-free survival.
Statistical analysis
All statistical analyses were performed using the SPSS 24.0 (IBM Corp., Chicago, IL) software for Windows. P < .05 was considered the statistical significance level. The distribution was assessed using the Kolmogorov–Smirnov test. Categorical data were reported as percentages, nonparametric variables as medians and interquartile ranges, and parametric variables as means ± standard deviation. For univariate analysis, the Chi-square test was used for nominal data. Parametric variables were analyzed using the t-test, while nonparametric variables were analyzed using the Mann–Whitney U test. The Kaplan–Meier method was used for BCR-free survival analysis, while the log-rank test was used to assess significance in the univariate analysis.
Results
Baseline features/demographics
The clinical and surgical data of 193 consecutive patients who underwent SP-RARP at our institution were collected and analyzed retrospectively. The median age of the patients at the time of surgery was 64 (9.5) years. It was determined that 48 patients (24.9%) had previously undergone abdominal surgery. According to the D’Amico risk classification, the number of patients in low, intermediate, and high-risk groups were 23 (11.9%), 110 (57%), and 60 (31.1%), respectively. All demographics and preoperative characteristics are presented in Table 1.
Comparison of the Demographics and Preoperative Characteristics of Patients According to Age
Mann–Whitney U test.
Chi-square test.
ASA, American Society of Anesthesiologists; BMI, body mass index; IQR, interquartile range; PSA, prostate-specific antigen.
Bold data signifies statistical significance.
BMI, ASA, race, D’Amico risk classification, and biopsy ISUP cancer grade were similar between the elderly and young patients (P = .340, P = .923, P = .261, P = .363, P = .512, respectively). It was determined that preoperative PSA level and previous abdominal surgery history were significantly higher in the elderly age-group (P = .042, P = .017, respectively). When the elderly group was evaluated, BMI, ASA, race, previous abdominal surgery history, preoperative PSA level, D’Amico risk classification, and biopsy ISUP cancer grade were similar between the young-old and old-old groups (P = .707, P = .094, P = .373, P = .942, P = .432, P = .650, P = .574, respectively) (Table 1).
Perioperative outcomes
Of these patients, 54 (28%) underwent the transperitoneal approach, while 139 (72%) had the extraperitoneal approach. Lymph node dissection was performed in 114 (59.1%) patients. The median total in-room time was 298 (68) minutes, while the procedure time was 244 (66) minutes. The intraoperative complications rate was 1.6%, with no conversions to open surgery in either group. The median LOS was 7 (22) hours, and 110 (57%) patients were discharged on the same day.
Surgical approach, lymph node dissection, intraoperative complications rate, nerve-sparing rate, total in-room time, procedure time, EBL, SDD rate, and LOS were similar between the elderly and young patients (P = .841, P = .764, P = .593, P = .272, P = .103, P = .103, P = .245, P = .529, P = .389, respectively). Within the elderly group surgical approach, lymph node dissection and intraoperative complications rate, nerve-sparing rate, total in-room time, procedure time, EBL, SDD rate, and LOS were similar between the young-old and old-old groups (P = .089, P = .572, P = .948, P = .680, P = .825, P = .907, P = .990, P = .212, P = .512, respectively) (Table 2).
Comparison of the Perioperative Outcomes in Groups
Chi-square test.
Mann–Whitney U test.
EBL, estimated blood loss; IQR, interquartile range; LOS, length of stay; SDD, same-day discharge.
Postoperative and oncological outcomes
We had an overall incidence of 24.4% of postoperative adverse events. The number of patients with Clavien Grade 1, 2, 3, and 4 complications were 3 (1.6%), 29 (15%), 12 (6.2%), and 3 (1.6%), respectively. The 30-days readmission rate was 11.4%. From an oncological outcome perspective, it was determined that 28 (14.5%) patients experienced BCR, and adjuvant therapy was initiated in 9 (4.7%) patients. The 3-years and 5-years BCR-free survival rates were 80.5% and 75.1%, respectively. The median follow-up time after surgery was 16 (29) months.
Major postoperative complications and readmission rates were similar between the elderly and young patients (P = .125, P = .821, respectively). It was determined that postoperative complication rate was significantly higher in the young patient group (P = .012). Within the elderly group, postoperative complications, major postoperative complications, and readmission rates were similar between the young-old and old-old groups (P = .442, P = .070, P = .835, respectively). Pathological outcomes were similar between age groups (Table 3). The BCR-free survival rates were similar between both young and elderly patients and between the young-old and old-old groups (P = .751, P = .765, respectively) (Fig. 1).
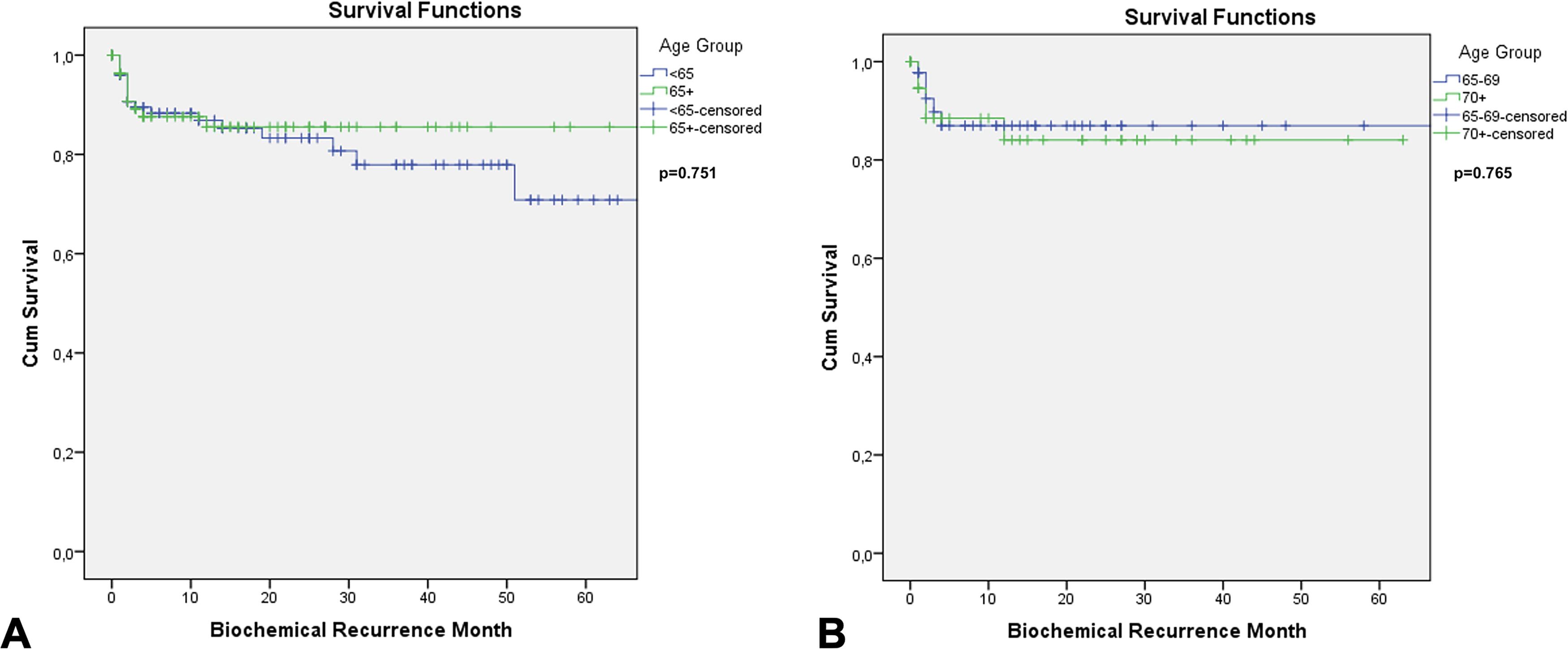
Kaplan–Meier analysis showing the effects of age groups on biochemical recurrence (BCR)-free survival.
Comparison of the Postoperative and Oncological Outcomes in Groups
Chi-square test.
Discussion
The global increase in life expectancy and widespread PSA testing in clinical practice have led to a rise in RP performed in both young and elderly populations. Since the introduction of the Da Vinci SP platform in 2018, experience with SP-RARP has steadily increased. This study aimed to share our experience with SP-RARP in elderly patients. Our findings demonstrated acceptable oncological outcomes and a low risk of complications after SP-RARP in elderly patients. We aspire to offer significant new perspectives to the existing literature concerning elderly patients with PCa.
It is known that, in the context of surgical morbidity and mortality, several risk factors increase with age; furthermore, advancing age itself remains a significant risk factor for these complications. 5 It has been shown that the pneumoperitoneum and steep Trendelenburg positioning required for MP-RALP can result in elevated intracranial pressure and may mildly affect postoperative cognitive function in elderly patients in the short term. 13 Furthermore, this positioning can limit diaphragmatic and chest wall movement, potentially having a negative impact on respiratory gas exchange. 14 In addition to the effects of positioning in MP-RALP, it has been demonstrated that SP-RALP offers shorter LOS and a higher rate of SDD compared with MP-RALP.15–18 For these reasons, the extraperitoneal approach provided by SP-RALP eliminates the necessity for a steep Trendelenburg position and pneumoperitoneum, which is especially beneficial for elderly patients with potentially limited respiratory reserves. Additionally, the possibility of SDD and shorter LOS can further help prevent potential hospital-acquired complications.
Our intraoperative complication rate was determined to be 1.6%, with no significant difference observed between age-groups. This rate is comparable with that reported in the literature. 18 None of these patients required open conversion. In the multicentric study by Soputro et al., the intraoperative complication rate after SP-RALP was reported as 0.4%, with all incidents occurring during the transperitoneal approach. 19 This situation highlights the safety of the extraperitoneal approach, which can be more easily implemented during SP-RALP.
In our study, the postoperative overall (any Clavien–Dindo) complication rate was determined to be 24.4%. Our complication rate was found to be like the studies in the literature. 18 It was found to be statistically significantly lower in the elderly age-group compared with the young patient group. No significant difference was found between the two groups in terms of major complications. It was speculated that the noticeably higher rate of stage 5 chronic kidney disease in the young patient group (12.4% vs. 6.8%) could have contributed to the increased incidence of minor complications. Since the aim of this study was to evaluate postoperative outcomes across age-groups, a multivariate analysis of the factors predicting complications was not conducted. Despite the significantly higher rate of previous intra-abdominal surgery and the higher proportion of high-risk patients according to the D’Amico risk classification in the elderly patient group, this difference suggests that SP-RARP is a safe option for the elderly patient group. Nowadays, with the increasing age of patients, the rate of history of intra-abdominal surgery is gradually rising. Here, the advantage of SP-RARP providing an extraperitoneal option becomes evident. The oncological and functional advantages provided by SP-RARP in patients with a hostile abdomen have been demonstrated in the literature. 8 Considering that the likelihood of a hostile abdomen is higher in the elderly age-group, our study supports this observation and demonstrates that SP-RARP is a safe option for elderly patients.
One of the most important stages of the follow-up process after RP is BCR. In our study, the 3-year and 5-year BCR-free survival rates were determined to be 80.5% and 75.1%, respectively. When evaluating these results, it is important to note that there are differences in the definition of BCR across studies. 20 In our study, we followed the recommendation of the American Urological Association and the European Association of Urology, which defines BCR as a serum PSA level of ≥0.2 ng/mL, confirmed by a second test.11,12 In our series, no significant difference was observed in this regard between the elderly and young patient groups. Despite the higher percentage of high-risk patients according to the D’Amico risk classification, the lack of difference between the two groups suggests that SP-RARP can be used safely from an oncological standpoint in the elderly patient group.
In our study, the rate of positive surgical margins was 45.5% in the younger group and 45.7% in the elderly group, both slightly exceeding the figures reported in the current literature on SP-RARP.18,21,22 The high rate of pathological T3 and patients with high-risk PCa in our series might have contributed to this outcome. Nonetheless, the proportion of patients who received adjuvant therapy remains quite low in our study (3.8% in the younger group and 5.7% in the elderly group). At present, there are limited data available on SP-RALP in the literature, but as more research emerges, our understanding of this outcome will expand accordingly.
Our study had several limitations. The primary and most significant limitation was its retrospective design. Another limitation is the lack of evaluation of functional outcomes following SP-RARP. However, it is well known that patients’ age is important in post-RP functional outcomes. 23 In our study, functional outcomes were not assessed due to the consideration of the age difference between patients. Another point to consider is the extensive experience at our center due to the long-term use of the Da Vinci SP platform. Therefore, this should be considered when interpreting the results of our study. Besides that, we included all patients who underwent SP-RARP since its introduction at our center, which means that the learning curve associated with SP may have impacted our results.
Aside from the limitations, we believe that the results of this study make a significant contribution to the literature, as it is one of the studies with the largest number of patients underwent SP-RALP reflecting single surgeon experience for this patient group.
Conclusion
In the young-old and old-old age-groups, SP-RARP seems to be the preferred treatment method due to its low postoperative complication rates and comparable oncological outcomes to those of younger patients. As the population ages, a patient’s age alone may no longer be a deciding factor in choosing SP-RARP during clinical decision-making. Additional multicenter studies with extended follow-up are needed to further evaluate our initial oncological outcomes in this patient group.
Footnotes
Authors’ Contributions
H.B.H.: Conception and design, data analysis and interpretation, drafting the article, and statistical analysis. L.L.: Conception and design, data acquisition, and statistical analysis. G.A.: Data analysis and interpretation. G.P.: Data analysis and interpretation. M.P.: Data analysis and interpretation. F.M.V.: Data acquisition and drafting the article. M.A.: Data acquisition and drafting the article. R.C.S.: Data acquisition and statistical analysis. J.R.T.-A.: Critical revision of the article for scientific and factual content. S.C.: Conception and design and critical revision of the article for scientific and factual content.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Disclosure Statement
S.C. is a consultant for Intuitive Surgical. The remaining authors have nothing to disclose.
Funding Information
No funding was received for this article.