
Abstract
Background:
The research on laparoscopic proximal gastrectomy has focused on effective methods of preventing reflux, few studies have focused on controlling the blood supply to the anastomosis site. Therefore, we introduced a modified approach to the vascular arch of the tubular stomach (TS) and conducted a preliminary examination of its safety and feasibility.
Methods:
Retrospective analysis of clinical data from 37 patients who underwent laparoscopic proximal gastrectomy at our center from March 2021 to June 2023, and comparison of clinical and pathological data, as well as intraoperative and short-term postoperative outcomes, between the modified TS group (n = 16) and the TS group (n = 21).
Results:
Compared with the TS, the modified TS had relatively longer operative times (170.63 ± 29.88 minutes versus 166.14 ± 27.49 minutes, P = .64) and anastomosis times (40.44 ± 6.60 minutes versus 36.14 ± 6.72 minutes, P = .06), and there was no significant difference in bleeding volume between the two groups (94.38 ± 75.19 mL versus 67.62 ± 44.15 mL, P = .14). There were 2 cases of postoperative anastomotic-related complications ((both of which were anastomotic bleeding) in the TS. No anastomotic-related complications were observed in the modified TS. There were a total of 6 cases in the postoperative gastroscopy modified TS, including 5 cases of LA-A and 1 case of LA-B; There are 10 cases of TS, including 7 cases of LA-A and 3 cases of LA-B.
Conclusions:
The modified TS during laparoscopic procedures is safe and feasible, decreasing to the maximal degree the potential blood supply disorders and bleeding risks at the anastomosis site while preventing reflux.
Background
The incidence of adenocarcinoma of the esophagogastric junction is increasing.1,2 The Siewert classification, which categorizes adenocarcinoma of the esophagogastric junction based on the tumor location, is widely accepted. 3 However, there is ongoing debate concerning whether proximal gastric resection or total gastrectomy should be performed for Siewert type II adenocarcinoma of the esophagogastric junction because of its unique anatomical features. 4 Retrospective and prospective studies of adenocarcinoma of the esophagogastric junction and lymph node metastasis conducted by the Japan Gastric Cancer Association have indicated the optimal regions for lymph node dissection and revealed that the incidence of lymph node metastasis near the right gastric and right gastroepiploic arteries is exceptionally low or, in some cases, non-existent.5–9 Therefore, exploration of proximal gastrectomy is worth considering. Previously, proximal gastric resection was hindered by postoperative reflux, which significantly impacted the patient’s quality of life and limited its widespread use. However, with the gradual improvement of laparoscopic techniques, more research has suggested that preserving the gastric function as much as possible to effectively prevent postoperative reflux is the most favorable option, especially for patients with early gastric cancer.4,10,11 There is no standardized approach for gastrointestinal reconstruction during laparoscopic proximal gastrectomy. Most studies have focused on preventing reflux, and few have considered the blood supply at the anastomotic site.12–16 During our clinical experience with the sideoverlap technique, we have observed potential issues with the blood supply at the anastomotic site. Therefore, we made modifications to the sideoverlap anastomosis of the vascular arch of the tubular stomach (TS) and explored the safety and practicality of this technique during laparoscopic gastrointestinal reconstruction.
Methods
We collected data from a total of 50 patients who underwent laparoscopic proximal gastrectomy at the Gastrointestinal Surgery Ward 2 of the Affiliated Tumor Hospital of Harbin Medical University from March 2021 to June 2023. Among them, 13 patients who underwent circular stapler anastomosis were excluded. The remaining 37 patients underwent laparoscopic sideoverlap anastomosis and met the following criteria: preoperative gastroscopy was utilized to identify or mark the lesion location; the cTNM staging for all patients was either cStage I or cStage IIA; a pathological examination confirmed the presence of adenocarcinoma; none of the patients had a history of gastric surgery; ASA grade ≤ II; no history of preoperative radiotherapy or chemotherapy; and no concurrent malignancies. According to the different handling methods for TSs, patients were divided into the modified TS group (n = 16) and the TS group (n = 21). All patients underwent gastroscopy, CT scans, and upper gastrointestinal angiography (UGI) contrast examinations, and signed informed consent forms.
Surgical technique
After confirming the absence of distant metastasis through laparoscopic examination, proximal gastrectomy and lymph node dissection were performed. The vascular and neural tissues around the remaining esophageal stump are fully dissociated, and the esophagus is transected under laparoscopy using a 60 mm linear stapler.
Preparation of TS
Extend the incision of the laparoscopic port by approximately 5 cm and the gastric wall was dissected on the distal side of the lesion. The lesion location was observed, and the distance from the lesion to the lower margin was measured. The proposed cutting line is from the junction of the gastric fundus and the gastric body at the greater curvature to the gastric angle Figure 1a, relatively parallel to the greater curvature and 3.0–4.0 cm away from the greater curvature, a linear stapler was used to transect the specimen Figure 1b. After the specimen was transected, an intraoperative frozen pathology examination of the upper and lower margins was performed. The ends were intermittently sutured to reinforce them.

Vascular dissection of the anastomosis area
Approximately 3 cm from the apex of the TS, the blood vessels on the portion of the greater curvature side near the gastric wall were dissected (length of approximately 3–4 cm). The proximal vascular arch of the TS was preserved Figure 2.
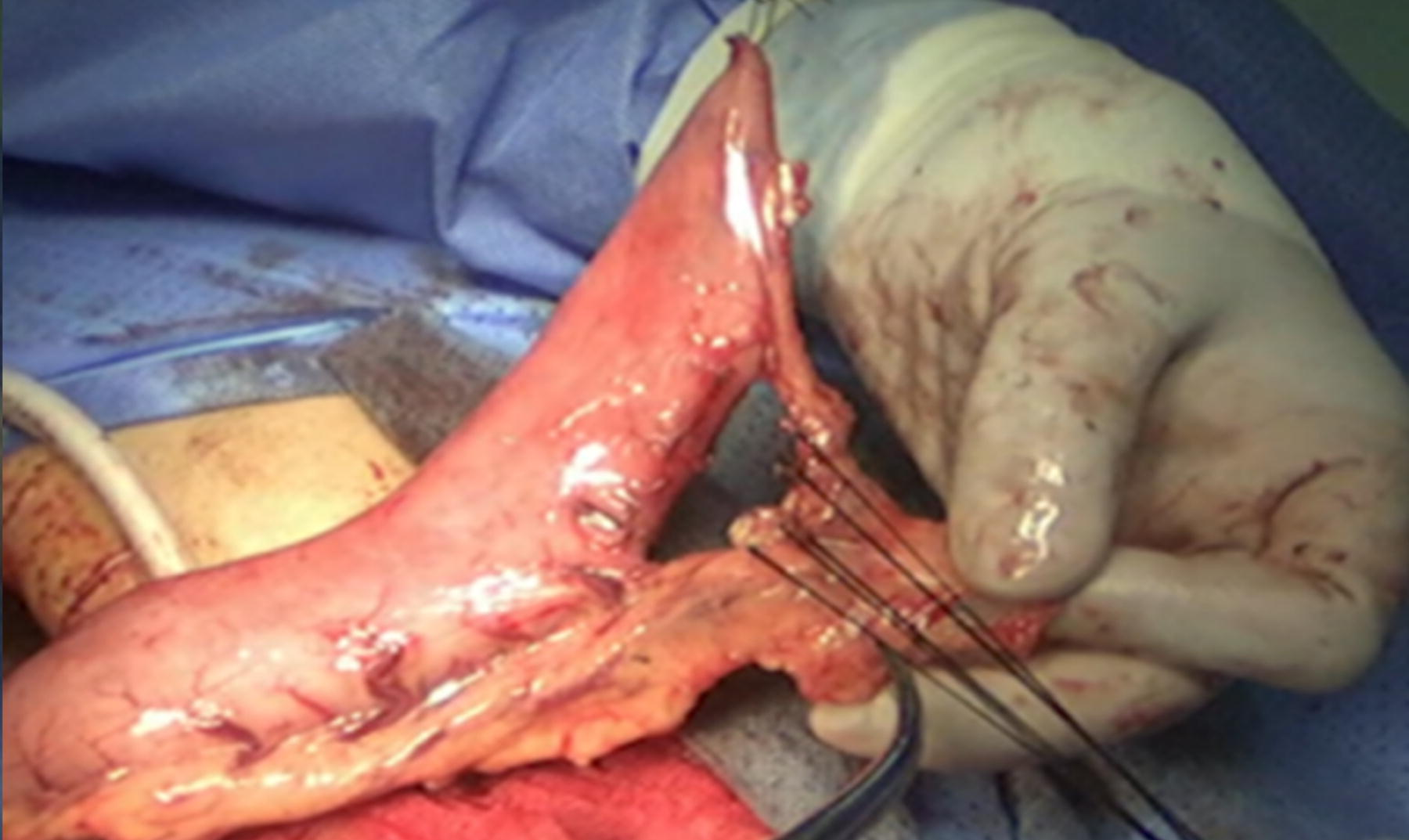
Preserving the proximal vascular arch of the TS and dissecting vascular in the intended anastomosis area. TS, tubular stomach.
Laparoscopic esophagogastric anastomosis
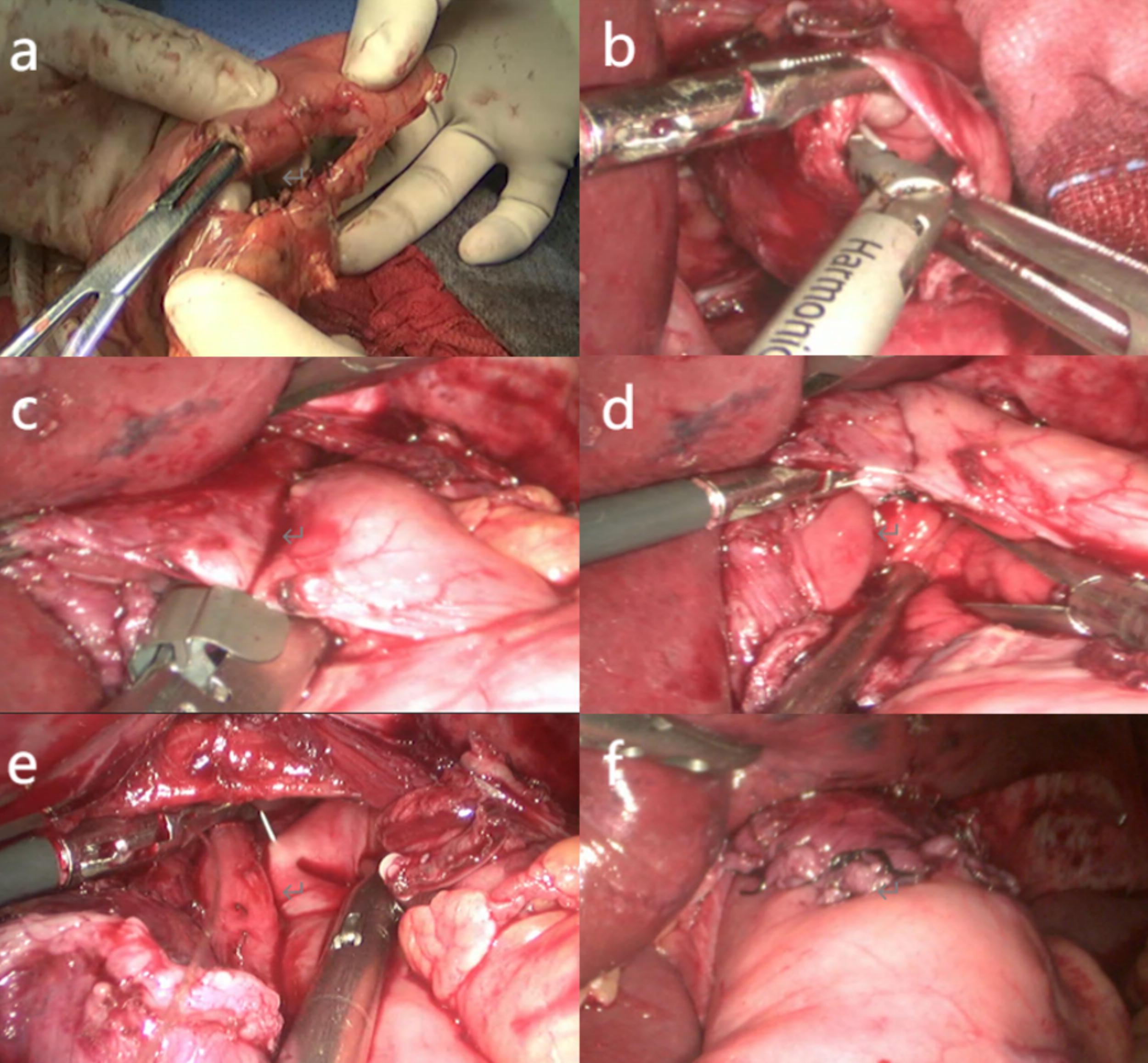
Perform esophagogastric anastomosis after negative intraoperative pathological report. Gas insufflation was established, and openings were made on the left wall of the esophagus and in the intended anastomosis area of the TS Figure 3a and b. A 45-mm linear stapler was used to dock the TS, which was then advanced to the esophageal hiatus. On the non-docking side, under the guidance of the gastric tube, it was inserted in the esophagus, and the angle was adjusted. The stapler was fired Figure 3c and the anastomotic site was examined to determine the presence or absence of bleeding Figure 3d. Double-barbed sutures were used to close the common opening Figure 3e. The right wall of the residual esophagus was sutured to the anterior wall of the TS to create overlap Figure 3f.
Postoperative management
The gastric tube was removed on the first day after surgery. Patients were allowed to consume water. After they passed gas, they were able to consume nutritional powder. On day 5 after surgery, abdominal computed tomography and Upper gastrointestinal (GI) series were performed. If the results were normal, then the patients were discharged. Subsequent follow-up included phone consultations every 3 months to monitor eating and reflux and a 1-year postoperative follow-up examination including gastroscopy and gastrointestinal contrast studies.
Statistical analysis
Statistical analysis was performed using IBM SPSS STATISTICS 22.0 software. The measurement data conforming to normal distribution are expressed as mean ± standard deviation (x ± s), and the independent sample t test was used for comparison between groups. Categorical variables were compared using the chi-squared or Fisher test. Statistical significance was defined when P < .05.
Results
General clinical and pathological data
The clinical and pathological data of two groups of patients are shown in Table 1, with 16 cases of modified TS and 21 cases of TS. There were 12 cases of Siewert II type and 4 cases of Siewert III type in the modified TS group, 18 cases of Siewert II type and 3 cases of Siewert III type in the TS group. In the modified TS group, there were 1 case of esophageal invasion length ≥1 cm, 2 cases <1 cm, and 13 cases without invasion. In the TS group, there were 1 case of esophageal invasion length ≥1 cm, 1 case <1 cm, and 19 cases without invasion. Postoperative pathology showed that in the modified TS group, there were 5 cases of stage IA, 3 cases of stage IB, 3 cases of stage IIA, 3 cases of stage IIIA, and 2 cases of stage IIIB. In the TS group, there were 3 cases of stage IA, 4 cases of stage IB, 4 cases of stage IIA, 5 cases of stage IIB, 2 cases of stage IIIA, and 3 cases of stage IIIB. The median follow-up time for patients in the modified TS group was 6 months, while in the TS group it was 8 months. There was no statistically significant difference in clinical basic information between the two groups of patients. Pathological staging was based on the eighth edition of the American Joint Committee on Cancer staging manual.
Clinical and Pathological Data
Data are expressed as mean ± standard deviation or n (%).
ASA, American Society of Anesthesiologists score; BMI, body mass index; TNM stage (tumor, node, metaphysis); TS, tubular stomach.
Intraoperative and postoperative outcomes
The intraoperative and postoperative results are shown in Table 2. Compared with the TS, the modified TS group had a relatively longer operative time (170.63 ± 29.88 minutes versus 166.14 ± 27.49 minutes, P = .64) and anastomosis time (40.44 ± 6.60 minutes versus 36.14 ± 6.72 minutes, P = .06). There was no significant difference in bleeding volume between the two groups (94.38 ± 75.19 mL versus 67.62 ± 44.15 mL, P = .14).
Intraoperative and Postoperative Outcomes
Data are expressed as mean ± standard deviation or n (%).
LA: The Los Angeles grading system was proposed at the 10th World Congress of Gastrointestinal Diseases in Los Angeles in 1994. The grading system defines esophageal mucosal damage as white moss or erythema with clear boundaries with surrounding mucosa, and divides RE into four levels based on the degree of mucosal damage: A∼D. LA-A: The lesion is limited to the esophageal mucosal folds, with a diameter of <.5 cm. LA-B: The lesion is still limited to the esophageal mucosal folds, not fused with each other, but with a diameter greater than .5 cm. LA-C: The lesion fuses at the top of the mucosa, but does not surround the entire esophageal wall. LA-D: Lesions fuse with each other, and the range is greater than 75% of the esophageal wall.
Short-term results were similar between the modified TS and TS groups, and included the time of the first passage of gas postoperatively, (3.25 ± .68 days versus 3.28 ± .64 days, P = .98), the time until starting a liquid diet (4.31 ± .79 days versus 4.38 ± .86 days, respectively; P = .81), and length of the hospital stay (6.68 ± 1.70 days versus 8.76 ± 1.67 days, respectively; P = .80).
There were no anastomotic complications in the modified TS group, while there were 4 cases of non-anastomotic complications, all of which were pulmonary related complications. The patient underwent UGI series before discharge, and all anastomoses were unobstructed. The patient reported no symptoms of choking or reflux after eating. In the TS group, there were two cases of anastomotic complications, both of which involved anastomotic bleeding. One case occurred on the second postoperative day. After fasting and receiving acid suppression therapy, hemostatic drugs were administered, leading to recovery on the third postoperative day. Blood tests and gastric tube examination indicated no active bleeding. Another case occurred on the fourth postoperative day, and recovery was achieved through endoscopic hemostasis treatment. There were seven cases of non-anastomotic complications, all of which were pulmonary complications.
Follow up gastroscopy examination after surgery: There were a total of 6 cases in the modified TS group, including 5 cases of LA-A and 1 case of LA-B; There are 10 cases of TS, including LA-A7 and LA-B3. The 16 patients showed no apparent symptoms of reflux esophagitis preoperatively, and upon reviewing the preoperative gastroscopic reports, none of them exhibited reflux esophagitis.
Discussion
Recent evidence has suggested that less extensive surgery for adenocarcinoma of the esophagogastric junction, such as proximal gastrectomy, that ensures oncological adequacy can help avoid postgastrectomy syndrome associated with total gastrectomy.17–21 Consequently, there is a growing interest in finding a safe and effective anastomosis technique to prevent reflux within the context of laparoscopic proximal gastrectomy reconstruction. Researchers have explored various anastomotic techniques, each with its own advantages and disadvantages; however, a unified standard has not yet been established.4,7,22–24
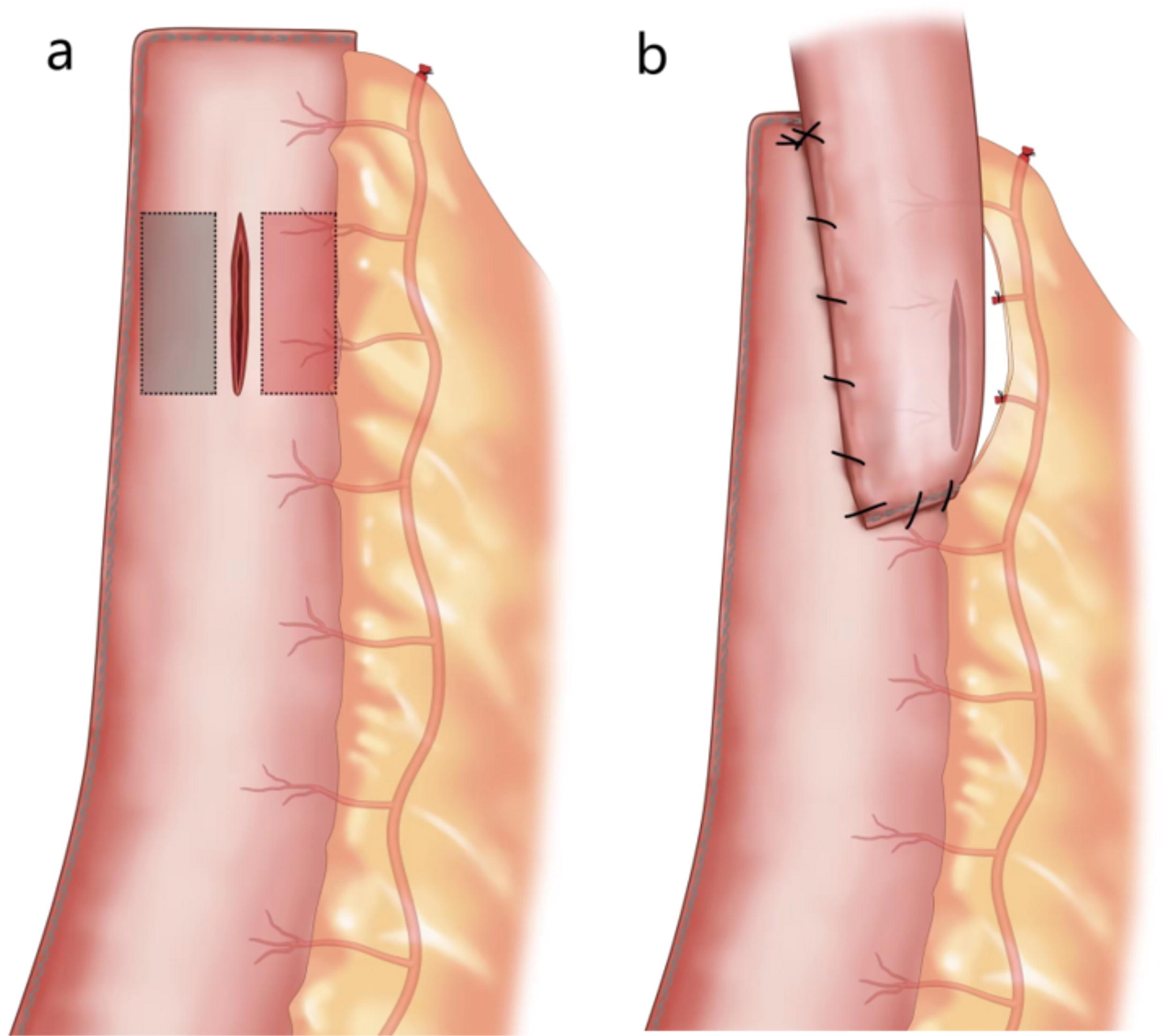
During our clinical experience with the sideoverlap technique, we observed that 2 cases of postoperative patients developed complications of anastomotic bleeding within 3 days after surgery. The sutures were accurately sutured during the surgery, and there was no fresh blood in the gastric tube. Therefore, we consider whether there is a potential issue of excessive or impaired blood supply at the anastomotic site in the treatment of the existing TS vascular arch. Specifically, We assume that after the production of a TS, the area near the lesser curvature (gray area) is a potential area of relative blood flow obstruction, while the area near the greater curvature (red area) is relatively too rich in blood flow, such as Figure 4a, which will increase the risk of anastomotic complications, such as anastomotic leakage or bleeding. Therefore, we modified the vascular arch of the TS and placed the anastomosis on the greater curvature side while preserving the proximal vascular arch of the greater curvature. Additionally, we exposed the blood vessels of the gastric wall in the intended anastomotic area before performing the sideoverlap anastomosis Figure 4b. This modification theoretically places the anastomotic site in an area with relatively even blood supply while preventing backflow, thereby improving safety.
Our preliminary data confirm the feasibility and safety of the modified anastomosis technique. Compared with the TS group, the modified TS group had slightly longer operative and anastomosis times, but the differences were not statistically significant. Vascular handling did not significantly extend the anastomosis time, supporting its feasibility. No anastomotic complications occurred in the modified TS group, and all patients recovered well, indicating its safety. In the TS group, two cases of anastomotic bleeding were reported: one resolved with conservative management and the other with endoscopic hemostasis. The bleeding was likely due to the rich blood supply at the anastomotic site, as intraoperative inspection confirmed secure suturing with no active bleeding or related comorbidities.
During follow-up, neither group showed significant reflux. Symptoms were effectively managed with dietary adjustments or intermittent Proton Pump Inhibitors (PPIs) use, without requiring long-term medication. Postoperative endoscopy revealed LA classifications similar to the TS group, indicating good short-term anti-reflux efficacy. To eliminate bias from preexisting reflux esophagitis, we compared pre- and postoperative endoscopy in 16 patients, none of whom had reflux esophagitis or significant reflux symptoms preoperatively.
We believe the primary advantage of this modified anastomosis lies in the improved vascular distribution to the anastomotic site. By positioning the anastomosis near the vascularized greater curvature, the risk of leakage due to inadequate blood supply is reduced. Additionally, selective ligation of certain gastric branches may mitigate the risk of bleeding from excessive vascularity, potentially achieving a balanced blood supply to the anastomotic site.
This study focused on addressing potential vascular issues related to the sideoverlap anastomosis during laparoscopic proximal gastric resection. As described, modifications were made to overcome these issues, and the initial observations have indicated promising results. However, the sample size of this study is relatively small and is still in the preliminary exploration stage. To obtain more accurate evidence, it is necessary to confirm the blood supply of the TS through indocyanine green or other evaluation tools. In the future, larger clinical trials and effective testing methods will be conducted to improve the data for maintaining the blood supply of the TS anastomosis.
This study hypothesizes potential vascular challenges in TS anastomosis and introduces a modification that has been preliminarily confirmed as feasible and safe. However, more definitive evidence is needed, which could be obtained using tools like indocyanine green or other vascular assessment methods to evaluate the blood supply of the TS. Future research with larger clinical samples and advanced diagnostic techniques will be necessary to further refine and validate data on maintaining optimal blood supply at the anastomotic site.
Conclusion
The modified TS anastomosis is safe, easy to perform, effectively prevents reflux, and ensures the anastomotic blood supply, thus making it an effective choice for digestive reconstruction during laparoscopic proximal gastrectomy.
Footnotes
Authors’ Contributions
Study concepts, study design, and article review: K.W. Data acquisition: Y.M.J. and P.C.S. Quality control of data and algorithms: Z.W. and G.Z. Data analysis and interpretation: Z.W., Q.W., and Y.W. Statistical analysis: Z.W. and S.Y.J. Article preparation and article editing: Z.W.
Ethics Approval and Consent to Participate
All programs followed were in accordance with the ethical standards of the Human Subjects Responsibility Committee (institutions and countries), as well as the 1964 Helsinki Declaration and subsequent editions. This research was approved by the Ethics Committee of the Harbin Medical University Cancer Hospital (approval number: 2023-200-QX). Informed consent to be included in the study, or the equivalent, was obtained from all patients.
Availability of Data and Materials
The database gathering all data used for this article is available for the Editor of this article for review
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This work was supported by the horizontal research project of Harbin Medical University (0401-22012180039).