
Abstract
Background:
Shortening the myotomy length during peroral endoscopic myotomy (POEM) for achalasia has been hypothesized to reduce gastroesophageal reflux disease (GERD) incidence while maintaining procedural efficacy. This meta-analysis compares the outcomes of short POEM (S-POEM) and long POEM (L-POEM).
Methods:
A systematic review adhering to PRISMA guidelines identified studies directly comparing S-POEM and L-POEM. Study quality was assessed using the Risk of Bias in Non-randomized Studies of Interventions and Revised Cochrane Risk of Bias for Randomized Trials tools. A pairwise meta-analysis was conducted using the random-effects model.
Results:
In perioperative outcomes, S-POEM significantly reduced operative time and required fewer clips compared with L-POEM, with no significant differences in adverse events or length of stay. Regarding GERD-related outcomes, S-POEM demonstrated a statistically significant reduction in abnormal esophageal acid exposure on 24-hour pH-impedance testing, with a number needed to treat of 10. While the reduction in symptomatic GERD did not reach statistical significance (P = .06), the P value was very close to the threshold for significance (.05), and all seven included studies reported decreased symptomatic GERD with S-POEM. This is therefore considered a noteworthy finding. The rates of esophagitis and lower esophageal sphincter pressure did not differ significantly between the groups. Efficacy-related outcomes, including clinical success, Eckardt score, and barium height at 5 minutes, were comparable between S-POEM and L-POEM. However, integrated relaxation pressure was significantly higher in the S-POEM group.
Conclusions:
This study suggests that shortening the myotomy length may reduce GERD incidence following POEM without compromising its efficacy in achalasia treatment. In addition, a shorter myotomy length decreases operative time, potentially reducing time-related costs and improving workflow.
Introduction
Achalasia is a rare esophageal motility disorder characterized by dysphagia, regurgitation, and chest pain, with an estimated annual incidence of approximately 1 in 100,000.1,2 Although significant progress has been made in understanding its pathophysiology, the precise etiology of achalasia remains elusive. 3 Current therapeutic approaches primarily target the disruption of the lower esophageal sphincter (LES), each with its own set of advantages and limitations.4,5 Endoscopic botulinum toxin injection, while safe and effective in the short term, provides symptom relief in only 29% of patients during intermediate follow-up. 6 Pneumatic dilation, another endoscopic treatment, achieves efficacy rates exceeding 90% but often requires multiple sessions and carries a perforation risk of 2%–5%.7–10 Laparoscopic Heller myotomy (LHM) offers a highly effective and complete disruption of the LES. However, this surgical approach is complex and is typically accompanied by an antireflux procedure due to the potential development of gastroesophageal reflux disease (GERD). 11 The advent of peroral endoscopic myotomy (POEM) has introduced a minimally invasive alternative to LHM that enables endoscopists to perform myotomy of the esophageal muscle fibers across the gastroesophageal junction (GEJ) and into the stomach via a submucosal tunnel. First demonstrated by Pasricha et al. in a pig model in 2007, 12 and later implemented clinically in humans by Inoue et al., 13 POEM has demonstrated high clinical efficacy, safety, and feasibility, with success rates generally reported above 90%.14,15 Despite its advantages, GERD remains a significant drawback of the POEM procedure. Unlike LHM, POEM does not facilitate fundoplication to prevent reflux. To address this issue, prior studies have explored potential associations between GERD incidence and various factors, including preoperative characteristics and technical aspects of the procedure, although no consensus has been reached.16–23 Recently, it has been hypothesized that reducing the myotomy length could mitigate GERD risk without compromising the effectiveness of the procedure. This study aims to compare short POEM (S-POEM) and long POEM (L-POEM) in terms of perioperative outcomes, GERD-related outcomes, and efficacy-related outcomes through a pairwise meta-analysis of comparative studies.
Materials and Methods
Study design and search strategy
We systematically conducted a literature search on PubMed and Google Scholar following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The search strategy included the keywords: “Achalasia,” “length,” “short,” “long,” and “peroral endoscopic myotomy.”
Eligibility criteria
Studies were included if they met the following criteria: 1 They were comparative in nature, 2 involved patients undergoing POEM, and 3 directly compared short POEM (S-POEM) with long POEM (L-POEM).
Data extraction
For each study that met the inclusion criteria, the following variables were extracted: The number of patients, gender distribution, mean age, country of origin, myotomy orientation or approach, extent and depth of myotomy, and myotomy length. In addition, data on perioperative outcomes (operative time, adverse events, number of clips used, and length of hospital stay), GERD-related outcomes (symptomatic GERD, abnormal esophageal acid exposure on 24-hour pH-impedance testing, esophagitis, and lower esophageal sphincter pressure), and efficacy-related outcomes (clinical success, Eckardt score, integrated relaxation pressure [IRP], and barium column height at 5 minutes) were collected.
Quality assessment of studies
The Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool 24 and the Revised Cochrane Risk of Bias for Randomized Trials (RoB 2) tool 25 were used to evaluate the quality of the included studies.
Data synthesis
Data analysis was performed using Review Manager (RevMan) 5.4.1 software. The random-effects model was employed for all analyses. Dichotomous data were analyzed using odds ratios (OR) as the effect size, while mean differences (MD) were used for continuous data. All results were reported with their corresponding 95% confidence intervals (CIs), and a P value of <.05 was considered statistically significant. Heterogeneity among studies was assessed using the I2 statistic. Subgroup analysis was performed by categorizing studies into randomized and nonrandomized groups. The OR and control event rate from individual studies were used to calculate the number needed to treat (NNT).26–29 All NNT values were presented along with their 95% CIs. NNTs and their corresponding 95% CIs were rounded up to the nearest whole number. 26
Results
Literature search results
PubMed and Google Scholar were systematically searched in accordance with PRISMA guidelines (Fig. 1). The initial search identified 974 records. Following a preliminary screening, 939 records were excluded as irrelevant. The remaining 35 reports were retrieved for detailed eligibility assessment. After thorough evaluation, 25 reports were excluded for the following reasons: studies assessing the impact of myotomy length on outcomes through regression analysis (n = 6), single-arm studies (n = 5), editorials (n = 4), case reports (n = 2), studies lacking meta-analyzable data (n = 2), abstracts with corresponding full articles available (n = 2), duplicate cohorts published more than once (n = 2), studies comparing mark-guided versus standard POEM (n = 1), and studies comparing single-scope versus double-scope POEM (n = 1). Ultimately, 10 studies met the inclusion criteria and were included in this meta-analysis.
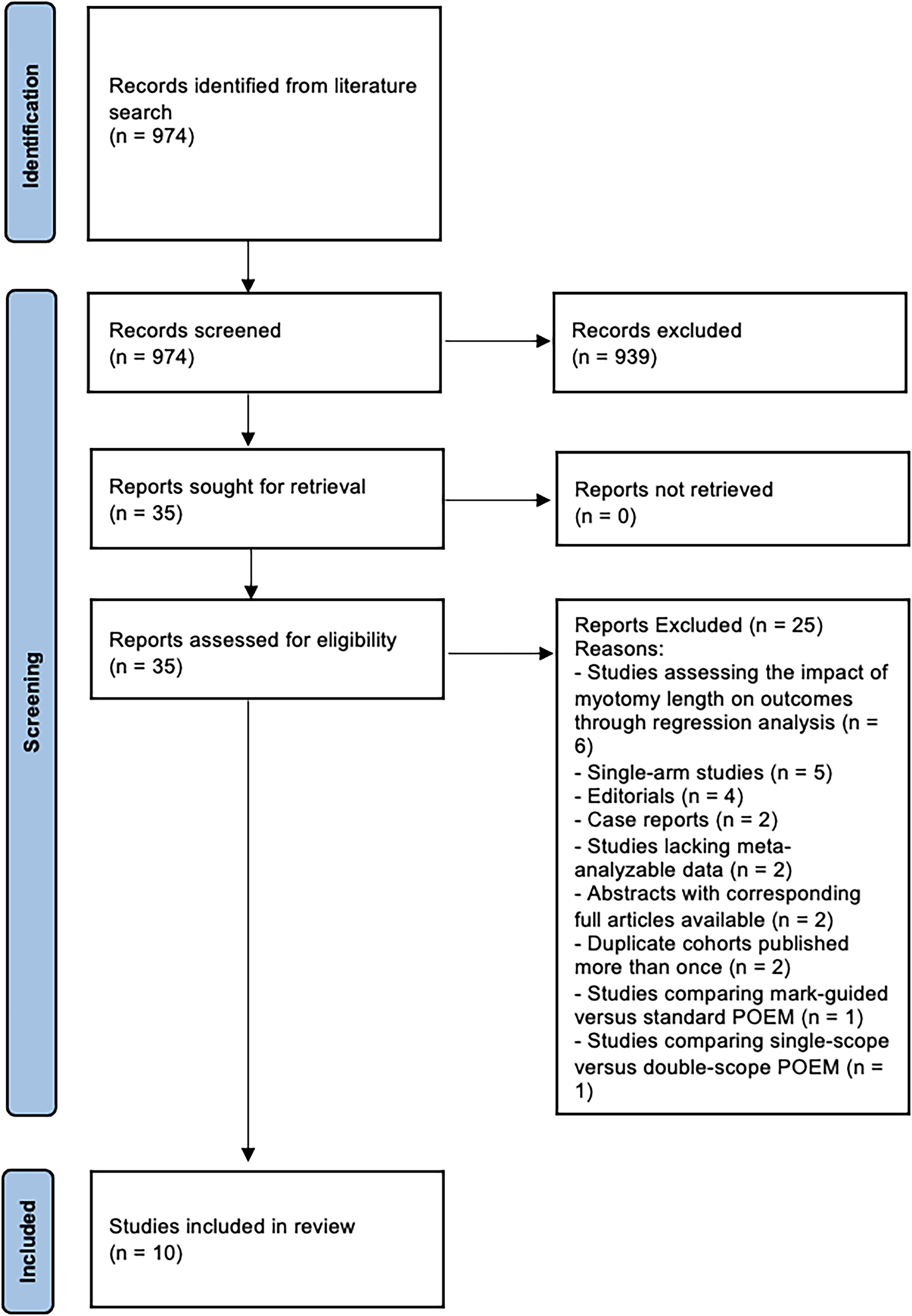
Literature review flow diagram following the PRISMA guidelines. The diagram illustrates the study selection process for inclusion in the review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality assessment results
Figure 2 illustrates the quality assessment results for the included studies, using the ROBINS-I (Fig. 2A) 24 and the RoB 2 tools (Fig. 2B). 25

Quality appraisal results of the studies using
The quality assessment of the five nonrandomized intervention studies, conducted using the ROBINS-I tool, classified two studies as having an overall moderate risk of bias. This classification was primarily driven by a moderate risk in the first domain (D1), which addresses confounding. The moderate risk was attributed to the absence of propensity-matched analysis, despite no significant differences in perioperative characteristics between the two groups. Two other nonrandomized intervention studies were classified as having an overall serious risk of bias, mainly due to a serious risk in the first domain (D1), where differences in at least one perioperative characteristic between the groups were identified. In the fifth study, insufficient information was provided in the first domain (confounding bias), making it challenging to determine the study’s overall quality (overall risk of bias) (Fig. 2A).
The quality assessment of the five randomized controlled trials, evaluated using the RoB 2 tool, indicated a low overall risk of bias in four of the studies. However, the fifth study was presented as an abstract and could not be assessed (Fig. 2B).
Study characteristics and baseline demographics
Table 1 provides a summary of the key characteristics of each study, including the country of origin, study design, and baseline demographic data (sample size, male-to-female ratio, and mean age) for patients in the S-POEM and L-POEM groups. In addition, it presents the quality assessment results, including the overall risk of bias.
General Characteristics, Baseline Demographics, and Quality Assessment Results
Age is reported as a mean, except in the two studies by Cecil (2024) and Familiari (2023).
This study was conducted in collaboration with 12 centers worldwide.
F, female; L, long POEM; M, male; NR, not reported; RCT, randomized controlled trial; S, short POEM; YO, year-old.
Technical data on POEM
Table 2 presents the technical details of POEM as reported in the included studies, including myotomy orientation or approach (anterior or posterior), extent or depth of myotomy (circular muscle or full-thickness), and myotomy length in the S-POEM and L-POEM groups.
Technical Data on POEM from Included Studies
The myotomy length is reported as a mean, except in three studies: it is reported as a median in Cecil (2024) and Familiari (2023), and as a range in Gu (2021).
In the Familiari, 2023, study, the myotomy approach/orientation was predominantly anterior but was posterior in a few cases.
In the Li, 2019, study, the myotomy depth was progressively full-thickness, initially targeting the circular muscle, with the depth increasing distally until achieving full-thickness. This technique was employed in most cases, whereas in a few cases, the myotomy was performed as a full-thickness myotomy, a circular muscle myotomy, or a combination of circular muscle incision and balloon plasty.
In the Nabi, 2021, study, circular muscle myotomy was performed in the upper portion of the tunnel, while full-thickness myotomy was conducted from 2–3 cm above the gastroesophageal junction (GEJ) to the lower end of the tunnel.
Approximately two-thirds of the patients underwent posterior myotomy, while the remaining patients underwent anterior myotomy.
Half of the patients in the short POEM group underwent full-thickness myotomy, while the other half underwent partial-thickness myotomy. In contrast, most patients in the long POEM group underwent full-thickness myotomy, with only a few cases involving partial-thickness myotomy.
Ant, anterior; CM, circular muscle; FT, full-thickness; L-POEM, long POEM; NR, not reported POEM, peroral endoscopic myotomy; post, posterior; S-POEM, short POEM.
Meta-analysis
Table 3 summarizes all 12 meta-analyses, categorized as follows: perioperative outcomes (4 meta-analyses), GERD-related outcomes (4 meta-analyses), and efficacy-related outcomes (4 meta-analyses).
Outcomes Summary
GERD, gastroesophageal reflux disease; IRP, integrated relaxation pressure; LES, lower esophageal sphincter; LOS, length of stay.
Meta-analyses of perioperative outcomes
Six studies reported the mean operative time (total patients = 526), with 190 patients in the S-POEM group and 336 in the L-POEM group. These studies showed a statistically significant decrease in the mean operative time in the S-POEM group compared with the L-POEM group (MD: −18.98, 95% CI: −23.37 to −14.59, P < .00001). The I2 = 25% (P = .25). Subgroup analysis, after dividing the studies into randomized and nonrandomized groups, did not reveal statistically significant differences between the subgroups (Fig. 3A).

Forest plot comparing the mean operative time
Eight studies reported the rate of adverse events (total patients = 776), with 359 patients in the S-POEM group and 417 in the L-POEM group. These studies showed a statistically insignificant decrease in the incidence of adverse events in the S-POEM group compared with the L-POEM group (OR: 0.73, 95% CI: 0.39–1.36, P = .32). The I2 = 25% (P = .23). Subgroup analysis, after dividing the studies into randomized and nonrandomized groups, did not reveal statistically significant differences between the subgroups (Fig. 3B).
Three studies reported the mean number of clips used (total patients = 206), with 93 patients in the S-POEM group and 113 in the L-POEM group. These studies showed a statistically significant decrease in the mean clips used in the S-POEM group compared with the L-POEM group (MD: −0.69, 95% CI: −1.34 to −0.04, P = .04). The I2 = 0% (P = .95). Subgroup analysis, after dividing the studies into randomized and nonrandomized groups, did not reveal statistically significant differences between the subgroups (Fig. 3C).
Three studies reported the mean length of stay (LOS) (total patients = 275), with 116 patients in the S-POEM group and 159 in the L-POEM group. These studies showed a statistically insignificant decrease in the mean LOS in the S-POEM group compared with the L-POEM group (MD: 0.25, 95% CI: −0.14 to 0.63, P = .21). The I2 = 37% (P = .20). Subgroup analysis, after dividing the studies into randomized and nonrandomized groups, did not reveal statistically significant differences between the subgroups.
Meta-analyses of GERD-related outcomes
Seven studies reported the rate of symptomatic GERD (total patients = 687), with 319 patients in the S-POEM group and 368 in the L-POEM group. These studies indicated a statistically insignificant decrease in the rate of symptomatic GERD in the S-POEM group compared with the L-POEM group (OR: 0.67, 95% CI: 0.44–1.02, P = .06). The I2 = 0% (P = .56). Although the reduction in symptomatic GERD with S-POEM did not reach statistical significance (p was .06), the P value was very close to the threshold for significance (.05). Furthermore, all the seven studies included in the analysis reported a decrease in symptomatic GERD with S-POEM. Subgroup analysis, after dividing the studies into randomized and nonrandomized groups, did not reveal statistically significant differences between the subgroups (Fig. 4A). The definition of symptomatic GERD was unclear in four of the seven studies, while the remaining three studies defined it using the GERD-Q score (see limitations).

Forest plot comparing the rates of symptomatic GERD
Four studies reported the rate of abnormal esophageal acid exposure on 24-hour pH-impedance testing (total patients = 328), with 171 patients in the S-POEM group and 157 in the L-POEM group. These studies showed a statistically significant decrease in the rate of abnormal esophageal acid exposure on 24-hour pH-impedance testing in the S-POEM group compared with the L-POEM group (OR: 0.62, 95% CI: 0.38–0.99, P = .04). The I2 = 0% (P = .46) (Fig. 4B). The NNT with S-POEM to prevent a single case of abnormal esophageal acid exposure on 24-hour pH impedance testing was 10 (95% CI: 6–422). The definition of abnormal esophageal acid exposure was based on 24-hour pH impedance testing, with a pH <4 observed for more than 6% of the time in all studies, except for Gu, 2021, where the threshold was set at greater than 5% of the time. Although the majority of patients in three of the studies underwent 24-hour pH impedance testing, this was not the case in Rai, 2024, where approximately half of the patients in both groups had the test (see limitations). In the Familiari, 2023, study, although most patients underwent 24-hour pH impedance testing, the number of patients tested in the L-POEM group was lower than in the S-POEM group (see limitations).
Seven studies reported the rate of esophagitis (total patients = 665), with 314 patients in the S-POEM group and 351 in the L-POEM group. These studies showed a statistically insignificant decrease in the rate of esophagitis in the S-POEM group compared with the L-POEM group (OR: 0.69, 95% CI: 0.37–1.27, P = .23). The I2 = 46% (P = .09). Subgroup analysis, after dividing the studies into randomized and nonrandomized groups, did not reveal statistically significant differences between the subgroups (Fig. 4C). Of the seven studies included in the esophagitis incidence meta-analysis, all or the majority of patients in both groups underwent postprocedural EGD in six studies. However, in the study by Swei, 2024, most patients did not undergo postprocedural EGD.
Two studies reported the mean LES pressure (total patients = 161), with 62 patients in the S-POEM group and 99 in the L-POEM group. These studies showed a statistically insignificant increase in the mean LES pressure in the S-POEM group compared with the L-POEM group (MD: 1.06, 95% CI −1.78 to 3.89, P = .47). The I2 = 76% (P = .04). Of the two studies included in the LES sphincter pressure meta-analysis, most patients in the L-POEM group in the study by Huang, 2020, underwent high-resolution manometry, whereas the majority in the S-POEM group did not (see limitations). In contrast, nearly all patients in the Gu 2021 study underwent high-resolution manometry.
Meta-analyses of efficacy-related outcomes
Eight studies reported the rate of clinical success (defined as Eckhardt score <3) (total patients = 747), with 349 patients in the S-POEM group and 398 in the L-POEM group. These studies indicated a statistically insignificant increase in the rate of clinical success (defined as Eckhardt score <3) in the S-POEM group compared with the L-POEM group (OR: 1.09, 95% CI: 0.54–2.21, P = .80). The I2 = 0% (P = .90). Subgroup analysis, after dividing the studies into randomized and nonrandomized groups, did not reveal statistically significant differences between the subgroups (Fig. 5A).

Forest plot comparing the rate of clinical success, the mean Eckardt score, and the mean IRP between S-POEM and L-POEM. IRP, integrated relaxation pressure; L-POEM, long peroral endoscopic myotomy; S-POEM, short peroral endoscopic myotomy.
Three studies reported the mean Eckhardt score (total patients = 268), with 113 patients in the S-POEM group and 155 in the L-POEM group. These studies showed a statistically insignificant increase in the mean Eckhardt score in the S-POEM group compared with the L-POEM group (MD: 0.01, 95% CI: −0.15 to 0.18, P = .90). The I2 = 0% (P = .40). Subgroup analysis, after dividing the studies into randomized and nonrandomized groups, did not reveal statistically significant differences between the subgroups (Fig. 5B).
Four studies reported the mean IRP (total patients = 351), with 170 patients in the S-POEM group and 181 in the L-POEM group. These studies showed a statistically significant increase in the mean IRP in the S-POEM group compared with the L-POEM group (MD: 1.04, 95% CI: 0.28–1.79, P = .007). The I2 = 12% (P = .33) (Fig. 5C). Among the four studies included in this analysis, high-resolution manometry was performed on all or nearly all patients in three studies (Gu, 2021, Rai, 2024, and Nabi, 2021). However, this information was unclear in the remaining one study (Huang, 2019).
Two studies reported the mean barium column height at 5 minutes (total patients = 124), with 61 patients in the S-POEM group and 63 in the L-POEM group. These studies showed a statistically insignificant increase in the mean barium column height at 5 minutes in the S-POEM group compared with the L-POEM group (MD: 0.25, 95% CI: −0.93 to 1.43, P = .67). The I2 = 76% (P = .04). In the two studies included in the analysis, all patients in Nabi, 2021, and Rai, 2024, underwent timed barium esophagogram (TBE).
Discussion
POEM has established itself as a safe and effective modality for treating achalasia and other nonachalasia spastic esophageal motility disorders. Since its introduction by Inoue and colleagues over a decade ago, 13 the fundamental technique of POEM has remained largely consistent. Key technical variations in POEM practices worldwide include the orientation of the myotomy (anterior versus posterior), the extent of the myotomy (full-thickness versus partial-thickness), and the esophageal myotomy length (short versus long). The impact of esophageal myotomy length on POEM outcomes remains inadequately understood. The standard myotomy length, initially established at approximately 10 cm by Inoue et al., 13 has since been widely adopted in clinical practice. The Society of American Gastrointestinal and Endoscopic Surgeons currently recommends extending the myotomy at least 4 cm into the distal esophagus and 1–2 cm below the esophagogastric junction onto the gastric wall to optimize outcomes. 33 Ten comparative studies in the literature have evaluated the perioperative outcomes, efficacy-related outcomes, and GERD-related outcomes of S-POEM versus L-POEM. Our meta-analysis of these studies has yielded noteworthy findings.
Perioperative outcomes
One notable advantage of a shorter myotomy is the significant reduction in operative time. The submucosal dissection, which is the most time-consuming part of the procedure, is shortened with a reduced tunnel length, thereby expediting the entire process. 30 Our meta-analysis demonstrates a consistent decrease in operative time across all included studies, highlighting this benefit. Shorter procedures also lead to reduced occupation of the operating or endoscopy room, offering substantial savings in both costs and resources. This efficiency may enable additional procedures to be performed within a single workday, further optimizing health care delivery. 30 Furthermore, a shorter submucosal tunnel directly affects the number of clips required, as less tissue is dissected. Consistent with the reduction in operative time, our analysis revealed a decrease in the number of clips used in the S-POEM group, potentially contributing to cost savings. From a safety perspective, no significant differences were observed between groups in terms of LOS or adverse events.
Efficacy-related outcomes
There has been speculation that a shorter myotomy length might compromise the efficacy of POEM. However, our study provides evidence to the contrary. No significant differences were observed between S-POEM and L-POEM in terms of postprocedural clinical success rates, mean Eckardt scores, or barium column height at 5 minutes. While a shorter myotomy was associated with a minor impact on IRP reduction, the mean difference was approximately +1.0. This small variation does not appear to influence clinical outcomes or symptom resolution, as reflected in comparable clinical success and Eckardt scores between the two groups. These findings suggest that shortening the myotomy does not compromise the overall efficacy of the procedure.
GERD-related outcomes
GERD has emerged as a significant drawback of the POEM procedure. Previous studies have attempted to identify associations between GERD incidence and various preoperative factors, patient characteristics, or technical aspects, but no consensus has been reached.16–23 Our meta-analysis suggests that reducing the length of myotomy may decrease the incidence of GERD, as indicated by both symptomatic GERD and abnormal esophageal acid exposure on 24-hour pH impedance testing analyses. Although the reduction in symptomatic GERD with S-POEM did not reach statistical significance (P was .06), the P value was very close to the threshold for significance (.05). Moreover, all seven studies included in the symptomatic GERD meta-analysis consistently demonstrated a lower incidence of symptomatic GERD with S-POEM compared with L-POEM. This finding was further supported by the statistically significant reduction in abnormal esophageal acid exposure, as objectively measured on 24-hour pH impedance testing. The reduction in abnormal acid exposure rates was consistent across all included studies with NNT of 10. Incidence of esophagitis and LES pressure did not differ significantly between groups.
The mechanisms underlying the observed reduction in GERD with shorter myotomy length in S-POEM remain speculative. One hypothesis suggests that preserving longer circular muscle fibers in S-POEM might help maintain esophageal axial shortening due to the spiral morphology of these fibers, facilitating aboral movement and preventing reflux of gastric contents into the esophagus.31,34,35 In addition, it has been proposed that a shorter esophageal myotomy preserves the gastric sling fibers of the LES, reducing sphincter laxity. 32 Because laxity of the LES has been shown to correlate with post-POEM GERD, preserving these fibers could potentially decrease GERD incidence.23,36–38
Limitations
This study has several limitations. First, half of the included studies were not randomized controlled trials, which limits the strength of the evidence and introduces potential biases. In addition, the quality assessment of the five nonrandomized studies revealed a moderate risk of bias in two studies, a serious risk of bias in two studies, and an unclear risk of bias in one study due to insufficient information.
Furthermore, within each study, there was no stratification of data according to achalasia type. Most studies included patients with both type 1 and type 2 achalasia, with a few also including type 3 achalasia. Stratifying the data to compare S-POEM and L-POEM for each type individually would provide greater insight into whether the findings apply uniformly across all achalasia types. Another limitation is the lack of stratification based on patients’ prior treatment history. While most studies included a small number of cases where endoscopic treatments had been attempted before POEM, this was not analyzed separately. Stratifying data to compare S-POEM and L-POEM specifically in patients with prior treatments would clarify whether the results are generalizable to this subgroup.
The definition of symptomatic GERD was unclear in four of the seven studies included in the analysis, while the remaining three studies used the GERD-Q score to define symptomatic GERD. This inconsistency introduces variability that could impact the reliability of the pooled results. Similarly, the meta-analysis of abnormal esophageal acid exposure on 24-hour pH impedance testing is limited by two of the four included studies (Rai, 2024, and Familiari, 2023). Although the majority of patients in three of the studies underwent 24-hour pH impedance testing, this was not the case in Rai, 2024, where approximately half of the patients in both groups had the test. In the Familiari, 2023, study, although most patients underwent 24-hour pH impedance testing, the number of patients tested in the L-POEM group was lower than in the S-POEM group. These observations in the Rai, 2024, and Familiari, 2023, studies may introduce a risk of bias due to missing data.
Further limitations relate to the meta-analyses of mean IRP and LES pressure. Among the four studies included in this analysis, high-resolution manometry was performed on all or nearly all patients in three studies (Gu, 2021, Rai, 2024, and Nabi, 2021). However, this information was unclear in the remaining one study (Huang, 2019). For the LES sphincter pressure analysis, one study (Huang, 2020) reported that most patients in the L-POEM group underwent high-resolution manometry, while the majority in the S-POEM group did not, introducing potential bias due to missing data. In addition, the inclusion of only two studies in this meta-analysis limits the robustness of the findings.
Finally, the meta-analysis of the barium column at 5 minutes is not reliable, as it included only two studies.
Conclusions
This study provides evidence suggesting that shortening the myotomy length may reduce the incidence of GERD following POEM without compromising its efficacy in treating achalasia. In addition, a shorter myotomy length decreases operative time, thereby reducing time-related costs and improving workflow. However, given the significant limitations of the current study, further randomized controlled trials with larger sample sizes are necessary to validate these findings.
Footnotes
Disclaimer
This research was supported in whole or in part by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the authors and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Authors’ Contributions
A.-R.F.D.: Literature reviewing, data collection, data interpretation, abstract writing, main text writing, and corresponding author. J.A.S.: Project design, data interpretation, and main text writing. C.M.: Literature reviewing, data collection, and main text writing. A.H.: Literature reviewing and data collection. Y.D.A.: Literature reviewing and data collection. S.D.: Project design, data interpretation, and mentorship in all project stages. C.G.D.: Project’s idea generation, project design, data interpretation, mentorship in all project stages, and principal investigator.
Disclosure Statement
The authors declare that there are no conflicts of interests.
Funding Information
No funding was received for this study.