
Abstract
Background:
Anastomotic stricture is a common complication following laparoscopic radical resection of rectal cancer, affecting up to 30% of patients and significantly impacting quality of life. This study aimed to develop a predictive model to identify high-risk patients and characterize stricture subtypes.
Methods:
Retrospective analysis of 304 patients undergoing laparoscopic rectal cancer resection (August 2019–April 2024) identified independent risk factors through multivariate logistic regression. A nomogram was developed and validated using receiver operating characteristic curves, calibration plots, and decision curve analysis. Subtype analysis compared Type I (dilatable, n = 51) and Type II (refractory, n = 38) strictures.
Results:
The nomogram incorporated five independent predictors: preoperative radiotherapy (odd ratio [OR] = 4.13), diverting stoma creation (OR = 6.98), lack of left colic artery preservation (OR = 3.95), anastomotic leakage (OR = 16.53), and anastomotic distance ≤3 cm (OR = 4.02), achieving an area under the curve (AUC) of .827. Type I strictures were significantly associated with diverting stoma creation (82.4% versus 39.5%, P = .004) and an anastomotic distance >3 cm (70.6% versus 36.8%, P = .001). The refined nomogram for Type II strictures demonstrated superior discrimination (AUC = .883, P < .001).
Conclusion:
This dual-phase nomogram effectively predicts overall anastomotic stricture risk and identifies refractory subtypes, enabling personalized postoperative management.
Introduction
Anastomotic stricture is a common complication following laparoscopic radical resection of rectal cancer, with reported incidence rates ranging from 5% to 30%. 1 This complication can significantly impact patient quality of life and may require additional interventions such as endoscopic dilation or surgical revision. 2 Predicting the risk of anastomotic stricture in patients undergoing laparoscopic radical resection of rectal cancer is important for optimizing postoperative management strategies and improving patient outcomes.
Several risk factors have been identified for the development of anastomotic stricture, including patient age, sex, body mass index (BMI), tumor location, and surgical technique.3–4 However, there is currently no widely accepted nomogram available to predict the individual risk of anastomotic stricture in this patient population.
In this retrospective study, we aimed to develop and validate a nomogram for predicting the risk of anastomotic stricture after laparoscopic radical resection of rectal cancer. By incorporating relevant patient characteristics and surgical factors into the nomogram, we sought to provide clinicians with a useful tool for assessing individual patient risk and tailoring postoperative care accordingly.
Materials and Methods
Patients
This retrospective study aimed to develop a predictive nomogram to identify key factors associated with the development of anastomotic stricture after laparoscopic radical resection of rectal cancer. We reviewed the medical records of patients who underwent laparoscopic radical surgery for rectal cancer between August 2019 and April 2024. All procedures were performed by experienced colorectal surgeons specializing in minimally invasive techniques. Inclusion criteria were as follows: (1) patients aged 18 years or older who underwent laparoscopic radical resection for rectal cancer; (2) patients who developed an anastomotic stricture postoperatively; and (3) patients with complete medical records and available follow-up data. Exclusion criteria were as follows: (1) patients who underwent open surgery or converted from laparoscopic to open surgery for rectal cancer; (2) patients without a confirmed diagnosis of anastomotic stricture; (3) patients with incomplete or missing medical records; and (4) patients who underwent additional surgeries that could affect the development of anastomotic stricture (e.g., reoperations for other pelvic diseases).
Data collection
We collected clinical, laboratory, and imaging data using the hospital’s electronic health records system. The following information was gathered: (1) demographic characteristics: age, sex, BMI, and comorbidities such as diabetes mellitus and hypertension; (2) clinical characteristics: tumor location (distance from the anal verge), preoperative chemoradiotherapy history, and TNM staging based on the American Joint Committee on Cancer criteria; (3) surgical details: operative time, blood loss, protective stoma creation, and intraoperative complications; and (4) postoperative outcomes: time to first flatus, length of hospital stay, postoperative complications including anastomotic leakage, and time to diagnosis of anastomotic stricture.
Laboratory tests included preoperative and postoperative measurements of white blood cell count, C-reactive protein, albumin levels, and hemoglobin. Imaging studies such as contrast-enhanced computed tomography scans and colonoscopy reports were reviewed to assess anastomotic integrity and confirm the presence of strictures.
Anastomotic stricture was identified through the assessment of one or more of the subsequent criteria: (1) the 12-mm coloscope was unable to pass through the anastomosis; (2) a digital rectal examination indicated either an obstructed anastomosis or a detectable narrow ring; and (3) gastrointestinal fluoroscopy revealed a stricture with a diameter smaller than 10 mm. We reclassified the cases based on the clinical management of the strictures: Type I (dilatable stricture): resolved with ≤3 sessions of finger or rigid endoscopic dilation. Type II (refractory stricture): required ≥4 dilation sessions or surgical reconstruction.
An exemption was received regarding ethical approval for this retrospective study from the institutional review board. The requirement for informed consent was waived due to the retrospective nature of the study and the use of deidentified patient data.
Statistical analysis
Statistical analyses were performed using GraphPad Prism 8.0 (GraphPad Inc., CA, USA) and IBM SPSS Statistics 23.0 (IBM Corp., Armonk, NY, USA). Data are presented as mean ± standard deviation or as counts and percentages (n, %). Depending on the data characteristics, the Chi-square test, Student’s t-test, or Mann–Whitney U test was utilized accordingly. Receiver operating characteristic (ROC) curve analyses were employed to assess the predictive value of continuous variables for postoperative weight regain and to determine optimal cutoff values. Risk factors for weight regain were assessed using binary univariate and multivariate logistic regression analyses with the “Enter” method. A nomogram incorporating the identified risk factors was constructed and evaluated using R software (version 4.0.1) with the “rms” package. A P value <.05 was considered statistically significant.
Results
Patient demographics and baseline characteristics
A total of 304 patients who underwent laparoscopic radical resection for rectal cancer were included in the study. Among these patients, 89 (29.3%) developed an anastomotic stricture postoperatively. The demographic and baseline characteristics of the patients are summarized in Table 1.
Patient Demographics and Baseline Characteristics
BMI, body mass index; LCA, left colic artery; TNM, tumor node metastasis classification; ASA, American society of Aneshesiologists(ASA) physical status classification system.
There were no significant differences between the stricture and non-stricture groups regarding age (64.1 ± 11.2 versus 62.3 ± 10.5 years, P = .15), sex distribution (male: 61.8% versus 60.5%, P = .82), ASA classification, hypertension, diabetes mellitus, alcohol consumption, preoperative hemoglobin levels, preoperative albumin levels, tumor size, tumor location, chemotherapy status, operative time, or TNM stage (all P > .05).
However, patients who developed an anastomotic stricture had a significantly higher BMI compared to those who did not (24.8 ± 7.2 kg/m2 versus 22.5 ± 6.3 kg/m2, P = .032). Preoperative radiotherapy was more common in the stricture group (53.9% versus 20.9%, P = .021). The creation of a diverting stoma was significantly associated with the development of anastomotic stricture (60.7% versus 17.7%, P = .010). Preservation of the left colic artery (LCA) was less frequent in patients with strictures (23.6% versus 77.7%, P = .001). Additionally, the incidence of postoperative anastomotic leakage was higher in the stricture group (51.7% versus 11.2%, P = .020). The anastomotic distance from the anal verge was ≤3 cm in a greater proportion of patients with strictures (62.9% versus 29.8%, P = .001).
Univariate and multivariate analysis of risk factors
Univariate logistic regression analysis identified several factors significantly associated with an increased risk of anastomotic stricture, including higher BMI (P = .015), preoperative radiotherapy (P = .021), creation of a diverting stoma (P = .001), lack of LCA preservation (P = .032), occurrence of anastomotic leakage (P = .021), and an anastomotic distance ≤3 cm from the anal verge (P = .001) (Fig. 1).

The forest plot of univariate logistic regression analysis for anastomotic stricture.
Variables with a P value <.05 in the univariate analysis were included in the multivariate logistic regression model. The multivariate analysis revealed that preoperative radiotherapy (odds ratio [OR] = 4.13; 95% confidence interval [CI]: 1.93–6.65; P = .012), creation of a diverting stoma (OR = 6.98; 95% CI: 3.02–7.95; P = .015), lack of LCA preservation (OR = 3.95; 95% CI: 1.89–6.02; P = .041), occurrence of anastomotic leakage (OR = 16.53; 95% CI: 4.99–18.05; P = .002), and an anastomotic distance ≤3 cm (OR = 4.02; 95% CI: 2.21–12.95; P = .001) were independent risk factors for the development of anastomotic stricture (Fig. 2, Table 2).
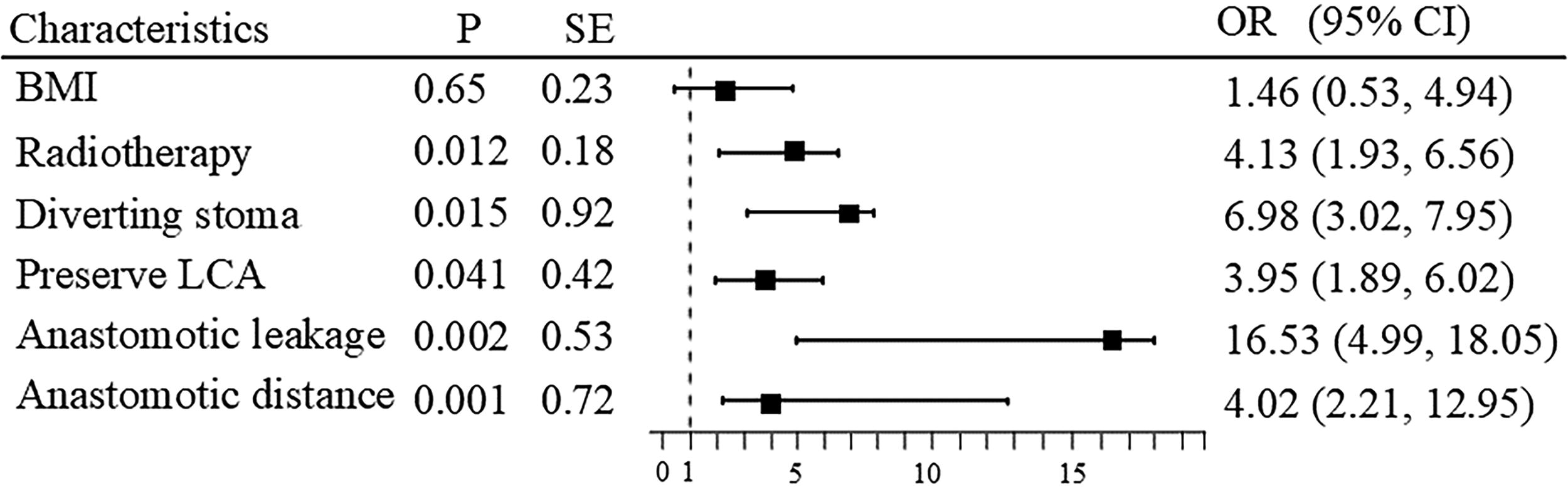
The forest plot of multivariate logistic regression analysis for anastomotic stricture.
Multivariate Logistic Regression Analysis of Risk Factors for Anastomotic Stricture
CI, confidence interval; LCA, left colic artery; OR, odds ratio.
Development of the nomogram
Based on the results of the multivariate analysis, a nomogram was constructed to predict the risk of anastomotic stricture after laparoscopic radical resection of rectal cancer (Fig. 3). The nomogram incorporated the five independent risk factors: preoperative radiotherapy, diverting stoma creation, LCA preservation, anastomotic leakage, and anastomotic distance from the anal verge. Each variable was assigned a score proportional to its relative contribution to the risk of stricture formation.

Nomogram for predicting the risk of anastomotic stricture after laparoscopic radical resection of rectal cancer.
Validation of the nomogram
The predictive performance of the nomogram was evaluated using the ROC curve and calibration plots. The nomogram demonstrated good discrimination, with an area under the ROC curve (AUC) of .827 (Fig. 4). Calibration plots indicated good agreement between the predicted probabilities and the actual observed outcomes, suggesting that the nomogram was well calibrated (Fig. 5).
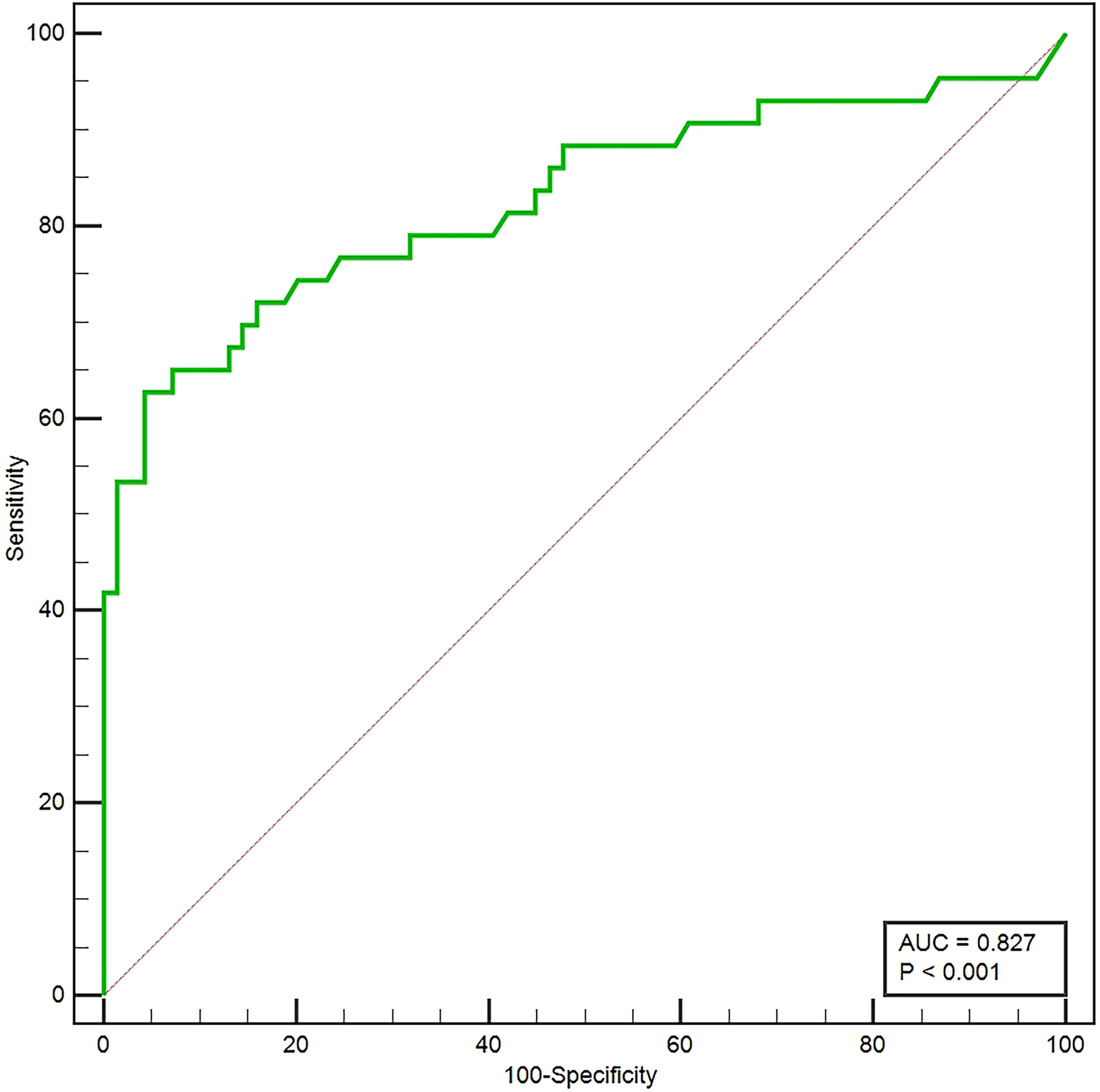
Receiver operating characteristic (ROC) curve for the nomogram.

Calibration plot for the nomogram.
Clinical utility of the nomogram
Decision curve analysis (DCA) was performed to assess the clinical utility of the nomogram. The DCA demonstrated that the nomogram provided a net benefit across a wide range of threshold probabilities, indicating its potential usefulness in clinical decision-making (Fig. 6). By using the nomogram, clinicians can identify high-risk patients who may benefit from closer postoperative surveillance and early interventions to prevent or manage anastomotic strictures.

Decision curve analysis (DCA) for the nomogram.
Analysis of stricture types
The analysis of risk factors for anastomotic stricture subtypes (Type I and Type II) is summarized in Table 3. Radiotherapy was more common in Type II strictures (44.7%) compared to Type I (21.6%), while the absence of radiotherapy was higher in Type I (78.4%) than in Type II (55.3%) (P = .621). Diverting stoma creation was significantly more frequent in Type I strictures (82.4%) compared to Type II (39.5%), whereas the absence of a diverting stoma was more common in Type II (60.5%) than in Type I (17.6%) (P = .004). Preservation of the LCA was observed in 76.5% of Type I strictures and 23.7% of Type II strictures, while the absence of LCA preservation was higher in Type II (76.3%) than in Type I (23.5%) (P = .152). Anastomotic leakage occurred in 52.6% of Type II strictures compared to 11.8% of Type I strictures, while the absence of leakage was more frequent in Type I (88.2%) than in Type II (47.4%) (P = .371). Anastomotic distance ≤3 cm was more common in Type II strictures (63.2%) compared to Type I (29.4%), while a distance >3 cm was more frequent in Type I (70.6%) than in Type II (36.8%) (P = .001). The predictive performance of the nomogram for Type II anastomotic stricture was evaluated using the ROC curve, as shown in Figure 7. The AUC was .883 (P < .001), indicating an excellent discriminative ability. The ROC curve demonstrates a high sensitivity and specificity for the nomogram in predicting Type II anastomotic strictures, confirming its robustness and clinical applicability.

Receiver operating characteristic (ROC) curve for the nomogram predicting Type II anastomotic stricture.
Comparative Analysis of Risk Factors Between Type I and Type II Anastomotic Strictures
LCA, left colic artery.
Discussion
In this retrospective study, we developed and validated a nomogram to predict the risk of anastomotic stricture following laparoscopic radical resection of rectal cancer. Our findings indicate that preoperative radiotherapy, creation of a diverting stoma, lack of preservation of the LCA, occurrence of anastomotic leakage, and an anastomotic distance of ≤3 cm from the anal verge are significant independent risk factors for anastomotic stricture. The nomogram incorporating these factors demonstrated good predictive accuracy and calibration, suggesting its potential utility in clinical practice.
Anastomotic stricture is a substantial postoperative complication that can adversely affect patient quality of life by causing symptoms such as obstructed defecation and abdominal discomfort.5–6 The reported incidence of anastomotic stricture varies widely, ranging from 5% to 30%, due to differences in definitions, surgical techniques, and patient populations.7–8 Identifying patients at high risk for stricture formation is essential for implementing preventive measures and optimizing postoperative management.
Our analysis revealed that preoperative radiotherapy significantly increases the risk of anastomotic stricture. Radiotherapy can impair wound healing by inducing fibrosis, reducing vascularity, and decreasing tissue oxygenation at the anastomotic site. 9 This finding aligns with previous studies that report higher rates of anastomotic complications in patients receiving preoperative radiotherapy.10–11 Therefore, careful consideration should be given to the timing and necessity of radiotherapy in patients with rectal cancer to mitigate this risk.
The creation of a diverting stoma was also identified as an independent risk factor. While diverting stomas are employed to reduce the severity of potential anastomotic leaks, they may contribute to mucosal atrophy and decreased blood flow due to diverted fecal stream, ultimately promoting stricture formation. 12 Clinicians should weigh the benefits and risks of stoma creation and consider strategies to preserve mucosal integrity when stomas are necessary.
Lack of LCA preservation emerged as a significant factor associated with stricture development. Preserving the LCA maintains adequate blood supply to the distal colon and anastomosis, which is crucial for healing. 13 Vascular compromise resulting from LCA ligation may lead to ischemia and subsequent fibrosis at the anastomotic site.14–15 Surgical techniques that prioritize vascular preservation could potentially reduce the incidence of strictures.
Anastomotic leakage was the strongest predictor of stricture formation in our study. Leakage induces local inflammation, fibrosis, and scar tissue formation, which can narrow the anastomotic lumen.16–17 Early detection and prompt management of anastomotic leaks are critical to minimize long-term complications such as strictures. Implementing intraoperative techniques to test anastomotic integrity and postoperative monitoring protocols may be beneficial.
An anastomotic distance of ≤3 cm from the anal verge was associated with an increased risk of stricture. Low rectal anastomoses pose technical challenges due to limited surgical space and may have compromised blood supply. 18 Additionally, the tension at low anastomotic sites can impede healing.19–20 Surgeons should exercise meticulous technique in low rectal anastomoses and consider protective measures to enhance healing.
The nomogram constructed from these risk factors demonstrated an AUC of .842, indicating strong discriminative ability. Calibration plots showed good agreement between predicted and observed outcomes, reinforcing the model’s reliability. DCA further supported the nomogram’s clinical applicability by demonstrating net benefit across a range of threshold probabilities.
Table 3 highlights the differences in risk factor distribution between Type I (dilatable strictures) and Type II (refractory strictures). Patients with Type II strictures had a higher proportion of preoperative radiotherapy (44.7% versus 21.6%) and absence of LCA preservation (76.3% versus 23.5%) compared to Type I strictures. Additionally, Type II strictures were more frequently associated with anastomotic leakage (52.6% versus 11.8%) and an anastomotic distance ≤3 cm (63.2% versus 29.4%). These findings suggest that Type II strictures are more likely to occur in patients with compromised vascularity, increased inflammation, or technical challenges related to low anastomoses. The significant differences in diverting stoma creation (39.5% in Type II versus 82.4% in Type I) further emphasize the complex interplay between protective measures and stricture severity.
Figure 7 demonstrates the robust predictive performance of the nomogram for identifying patients at risk of Type II strictures. The ROC curve yielded an AUC of .883, indicating an excellent discriminative ability. This high AUC value underscores the nomogram’s utility in accurately stratifying patients based on their risk of developing refractory strictures. The strong predictive performance aligns with the inclusion of key independent risk factors, such as preoperative radiotherapy, diverting stoma creation, LCA preservation, anastomotic leakage, and anastomotic distance.
These findings collectively validate the clinical relevance of the nomogram in tailoring postoperative management strategies. For patients identified as high-risk for Type II strictures, closer monitoring, early endoscopic interventions, or alternative surgical techniques may be warranted to mitigate complications. Future studies should explore the integration of this nomogram into clinical workflows and assess its impact on long-term patient outcomes.
Our study has several strengths, including a substantial sample size derived from two institutions and comprehensive data collection allowing for robust multivariate analysis. However, certain limitations must be acknowledged. The retrospective design may introduce selection and information biases. Additionally, the study’s findings are based on data from two centers, and external validation in diverse populations is necessary to confirm the generalizability of the nomogram. Factors such as smoking status, nutritional parameters, and genetic predispositions were not evaluated and could potentially influence stricture risk.
Future research should focus on prospective studies to validate our nomogram and explore interventions targeting modifiable risk factors. For instance, strategies to enhance anastomotic healing in patients receiving radiotherapy or innovations in surgical techniques that preserve vascular supply could be investigated. Personalized postoperative care protocols based on individual risk assessments may improve patient outcomes and reduce the incidence of anastomotic strictures.
Conclusion
We have developed and validated a nomogram that effectively predicts the risk of anastomotic stricture following laparoscopic radical resection of rectal cancer. The nomogram incorporates five independent risk factors: preoperative radiotherapy, diverting stoma creation, lack of LCA preservation, anastomotic leakage, and an anastomotic distance of ≤3 cm from the anal verge. This predictive tool can assist clinicians in identifying high-risk patients, allowing for tailored postoperative management strategies aimed at preventing or promptly addressing anastomotic strictures. Implementation of this nomogram in clinical practice has the potential to enhance patient outcomes and quality of life after rectal cancer surgery.
Footnotes
Acknowledgment
The authors thank the medical staff of their hospital for database management.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was received for this article.