
Abstract
Purpose:
Minimally invasive surgery is the standard approach for colorectal cancers and requires an abdominal incision for specimen removal. Natural orifice specimen extraction (NOSE) may improve outcomes, reducing trauma, and speeding postoperative recovery. This study compares both techniques regarding postoperative complications, operative outcomes, and recurrence.
Methods:
We searched PubMed, Scopus, and Cochrane Central Register of Clinical Trials for studies published up to November 2024. Odds ratios (ORs) and mean differences (MDs) with 95% confidence intervals (CIs) were pooled using a random-effects model, and heterogeneity was assessed with I2 statistics. Statistical analyses were conducted using R Software version 4.4.1 (R Foundation for Statistical Computing).
Results:
Four randomized controlled trials involving 439 patients with colorectal cancer were included, with 212 (48.2%) undergoing NOSE and 227 (51.7%) undergoing conventional laparoscopic specimen extraction. NOSE significantly reduced postoperative pain (visual analog scale score: mean difference [MD] −1.8; 95% confidence interval [CI] −2.5 to −1.1; P = .01), time to pass flatus (MD −0.8; 95% CI −1.1 to −0.6; P < .01), and surgical site infection rates (OR 0.15; 95% CI 0.03–0.69; P = .015) but was associated with a longer operative time (MD 11.1 minutes; 95% CI 1.5–20.6; P = .02). No significant differences were observed between the groups in bowel leaks, lymph nodes harvested, intraoperative blood loss, hospital stay duration, or local recurrence rates.
Conclusion:
NOSE was associated with reduced postoperative pain, faster time to pass flatus, and lower infection rates but required longer operative time than conventional laparoscopic specimen extraction. Other outcomes, including complications, operative characteristics, and recurrence, showed no significant differences between the techniques.
Introduction
Colorectal cancer ranks as the third most diagnosed cancer globally and the second leading cause of cancer-related mortality.1,2 Minimally invasive laparoscopic-assisted procedures are widely preferred for colorectal cancer due to their balance between reduced trauma, enhanced recovery, and effective surgical outcomes.3–6 However, these procedures often require a 5–10 cm abdominal incision for specimen extraction and to provide the final steps of colorectal anastomosis.3,6,7
Laparoscopic natural orifice specimen extraction (NOSE) was first described by Franklin in 1993. 5 Subsequently, the technique was further refined into what is now known as natural orifice transluminal endoscopic surgery (NOTES), which merges laparoscopic and endoscopic methods.5,6,8,9 This approach allows for colonic mobilization, transection, and intracorporeal colorectal anastomosis to be performed laparoscopically while the specimen is extracted transanally, avoiding the need for a mini-laparotomy.5,6,8,9 This innovation eliminates abdominal incisions for specimen extraction, reducing surgical trauma and improving postoperative recovery.4,6,10–12 NOSE and NOTES have gained particular traction in China due to their minimally invasive nature and potential for better cosmetic and functional outcomes. These techniques represent a significant advancement in colorectal surgery, aligning with the goals of modern minimally invasive procedures to enhance recovery and reduce complications.4,6,10–12
In recent years, several meta-analyses have compared NOSE and conventional laparoscopic approaches.13,14 One included low-quality randomized studies with overlapping samples, 13 while another focused on observational studies and three randomized trials but failed to distinguish between right- and left-sided colorectal cancers. 14 Our study updates the evidence by adding more randomized controlled trials (RCTs) and focusing exclusively on left-sided colorectal cancer treated with the NOSE or NOTES procedure and no overlapping sample.
Materials and Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. 15 The study protocol was registered in the International Prospective Register of Systematic Reviews with registration number CRD42024626086. 16
Search strategy
A systematic search was performed on PubMed, Cochrane Central Register of Clinical Trials, and Scopus for studies published up to December 2024. The search strategy was as follows: ((“Colorectal Cancer” OR “Colonic cancer” OR “Left-sided colon cancer” OR “Left colon cancer” OR “Colon neoplasms” OR “Colorectal neoplasms” OR “Colon* carcinoma” OR “Colonic tumor” OR “Left colonic cancer” OR “Left colectomy” OR “Left hemicolectomy” OR “Sigmoid cancer” OR “Sigmoidectomy” OR “Rectal cancer” OR “Rectal neoplasms” OR “Rectal carcinoma” OR “colon* adenocarcinoma” OR “Malignant neoplasm of the colon” OR “Large bowel cancer”) AND (“Natural orifice specimen extraction” OR “NOSE” OR “N.O.S.E” OR NICE OR “Transrectal specimen extraction” OR “Transvaginal specimen extraction” OR “Transcolonic specimen extraction” OR “Natural orifice surgery” OR “Natural orifice surgery extraction” OR “NOTES” OR “Specimen extraction”) AND (“Conventional colectomy” OR “Laparoscopic colectomy” OR “Open colectomy” OR “Hemicolectomy” OR “Left hemicolectomy” OR “Transabdominal specimen extraction” OR “Laparoscopic surgery” OR “Surgical specimen extraction” OR “Minimally invasive colectomy” OR “Minimally invasive surgery” OR “Traditional colectomy” OR “Conventional surgery”)).
Eligibility criteria
We included RCTs comparing NOSE or NOTES and conventional laparoscopic-assisted procedures for left-sided colorectal cancer. The exclusion criteria were: (1) patients undergoing diverting procedures, (2) studies lacking a control group, or (3) case reports, conference abstracts, reviews, or animal experiments.
Data extraction and endpoints
Two authors (J.H.B. and L.S.G.) independently screened the articles for inclusion criteria and extracted data from the selected studies. Any disagreements were resolved by consensus or, if necessary, by consulting a third author (B.F.P.). The outcomes assessed were postoperative complications, including (1) visual analog scale (VAS) score within 5 days, (2) surgical site infection (SSI), (3) bowel leak, (4) gas passage, (5) lymph nodes harvested, (6) blood loss, (7) operative time, (8) hospital stay, and (9) local recurrence.
Quality assessment
Two authors (B.F.P and L.S.G) independently assessed the quality of included studies using the Revised Cochrane risk-of-bias tool (RoB 2). 17 In this assessment, each study is categorized as low risk or high risk or may express some concerns in five domains: randomization, deviations from intended intervention, missing outcome data, measurement of the outcome, and selection of the reported result. Disagreements were resolved unanimously with the senior author (F.B.F).
Statistical analysis
We pooled risk ratios (RR) for binary outcomes and mean differences (MD) for continuous endpoints, with 95% confidence intervals (CI). A random-effects model was used for all outcomes. Statistical significance was defined as P < .05. Heterogeneity was assessed using the Cochran Q test and I2 statistics, with P values lower than .10 and I2 >25% being considered significant for heterogeneity. For outcomes with substantial heterogeneity, we used Baujat plots to assess each study’s contribution to the overall effect and heterogeneity. Furthermore, we also performed leave-one-out sensitivity analyses by systematically removing each study from the pooled estimates to ensure the robustness of the results. R Software (R Foundation for Statistical Computing), version 4.4.1, was used for statistical analysis.
Results
Study selection and characteristics
As shown in Figure 1, the initial database search identified 1214 results. After screening, 260 duplicates were removed and 946 records were excluded based on titles and abstracts, leaving four RCTs for the final analysis.3–6

PRISMA flow diagram of study screening and selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
The included trials involved 439 patients diagnosed with colorectal cancer. Of these, 212 (48.2%) underwent NOSE, while 227 (51.7%) received traditional laparoscopic specimen extraction.3–6 Men constituted 51.2% of the study population.3–6 The average age was 60.5 ± 2.9 years in the NOSE group and 63.0 ± 5.4 years among those treated with conventional methods.3–6 The mean BMI was reported as 23.0 ± 0.7 kg/m2 in the NOSE group and 23.4 ± 0.8 kg/m2 in the non-NOSE cohort.3–6
In two of the included trials, endoscopic devices were utilized for specimen extraction in the NOSE group.3,4 One study used a Cai tube inserted transanally, while the other employed a sleeve pouch for specimen removal via the same route.5,6 Conversely, the conventional laparoscopic group relied on a laparotomy incision for specimen extraction.3–6 Tumor localization was distributed as follows: 2.1% in the descending colon, 40.4% in the sigmoid colon, 9.6% in the rectosigmoid junction, and 47.9% in the rectum.3–6 Tumor, Node, Metastasis staging revealed 29.6% of cases classified as stage I, 39.8% as stage II, 23.1% as stage III, and 0.9% as stage IV.3–6 The mean tumor size for left-sided lesions was 2.95 ± .51 cm, with a mean distal margin of 4.15 ± 1.46 cm.3–6 The average follow-up period across all studies was 33.83 ± 12.56 months, although one trial reported a longer follow-up of 48.9 ± 32.3 months.3–6 Additional details regarding study characteristics are provided in Tables 1 and 2.
Baseline Characteristics of the Randomized Controlled Trials Included
Mean and standard deviation.
C, conventional colectomy; N, NOSE colectomy; NA, not available; NOSE, natural orifice specimen extraction; RCT, randomized control trial
Surgical Characteristics of the Studies Included in the Meta-Analysis
Mean and standard deviation.
C, conventional colectomy; N, NOSE colectomy; NA, not available.
Pooled analyses of all studies
Postoperative complications
In the pooled analysis with patients who underwent laparoscopic surgery for colorectal cancer with NOSE versus conventional specimen extraction, postoperative pain (VAS score) was significantly lower in the NOSE group compared with the non-NOSE group (MD −1.8; 95% CI −2.5 to −1.1; P = .01; I2 = 93%; Fig. 2A).3–6 There was a high heterogeneity. Similarly, the NOSE group was significantly associated with lower rates of SSI (odds ratio [OR] 0.15; 95% CI 0.03–0.69; P = .015; I2 = 0%; Fig. 2B).3–6 No significant differences were observed between the groups for bowel leak (OR 1.95; 95% CI 0.50–7.65; P = .336; I2 = 0%; Fig. 2C). The last two outcomes demonstrated low heterogeneity.3,5,6

Forest plots of comparison between NOSE versus conventional laparoscopic surgery in colorectal cancer:
Operative and recurrence
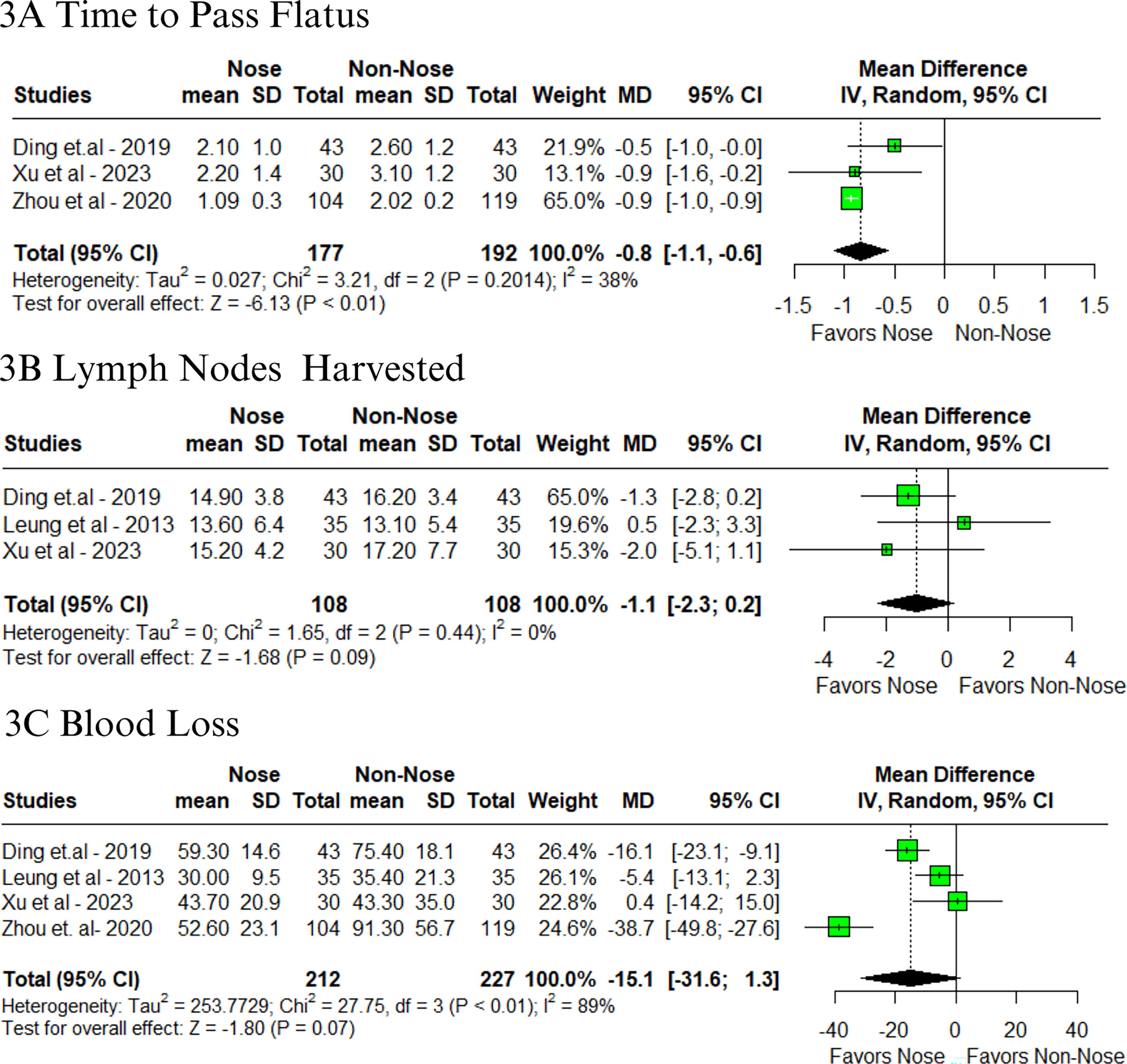
In terms of operative outcomes, a significant difference was observed in the time to pass flatus, favoring the NOSE group (MD −0.8; 95% CI −1.1 to −0.6; P < .01; I2 = 38%; Fig. 3A).3,5,6 However, for lymph nodes harvested (MD −1.1; 95% CI −2.3 to 0.2; P = .09; I2 = 0%; Fig. 3B) and intraoperative blood loss (MD −15.1 mL; 95% CI −31.6 to 1.3; P = .07; I2 = 89%; Fig. 3C), no significant differences were found.3–6 The lymph node resection outcome showed low heterogeneity, while the other two demonstrated moderate to high heterogeneity.
Forest plots of comparison between NOSE versus conventional laparoscopic surgery in colorectal cancer:
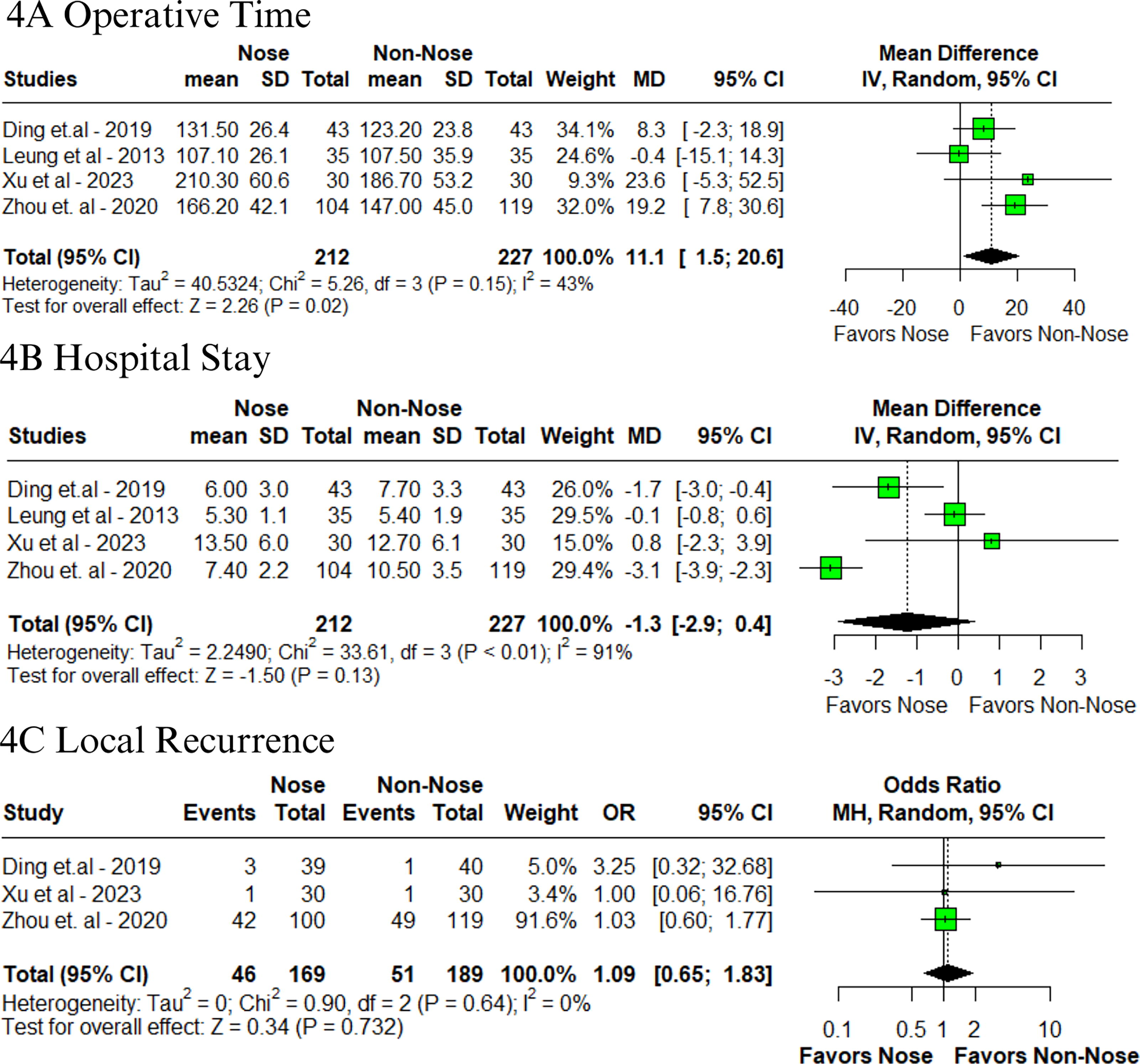
Conversely, operative time was significantly longer in the NOSE group (MD 11.1 minutes; 95% CI 1.5–20.6; P = .02; I2 = 43%; Fig. 4A).3–6 There was moderate heterogeneity. No significant differences were found between the groups in the length of hospital stay (MD −1.3 days; 95% CI −2.9 to 0.4; P = .13; I2 = 91%; Fig. 4B) and local recurrence (OR 1.09; 95% CI 0.65–1.83; P = .732; I2 = 0%; Fig. 4C).3–6 High and low heterogeneity were observed, respectively.
Forest plots of comparison between NOSE versus conventional laparoscopic surgery in colorectal cancer:
Sensitivity analyses
In the Baujat plot analysis, the studies that contributed most to heterogeneity were identified. Regarding postoperative pain, Leung et al. were the primary contributors, and after its exclusion in the leave-one-out analysis, the results remained consistent (Supplementary Figs. S1, Figs. S2). 4 For time to pass flatus, Ding et al. emerged as the main contributor; excluding this study did not affect the overall results (Supplementary Figs. S3, Figs. S4). 3 When evaluating blood loss, Zhou et al. stood out as the primary contributor (Supplementary Fig. S5). 5 The leave-one-out analysis confirmed consistent results (Supplementary Fig. S6). Similarly, Leung et al. contributed the most to heterogeneity for operative time (Supplementary Fig. S7). 4 Their exclusion in the leave-one-out plot did not change the results (Supplementary Fig. S8). Lastly, Zhou et al. were identified as the main contributors to heterogeneity in hospital stay, and their exclusion showed consistent results (Supplementary Figs. S9, Figs. S10). 5
Quality assessment
The individual assessment of each study included in the meta-analysis is illustrated in Figure 5. After thoroughly evaluating the five domains, all RCTs were determined to have a low risk of bias in every domain.3–6
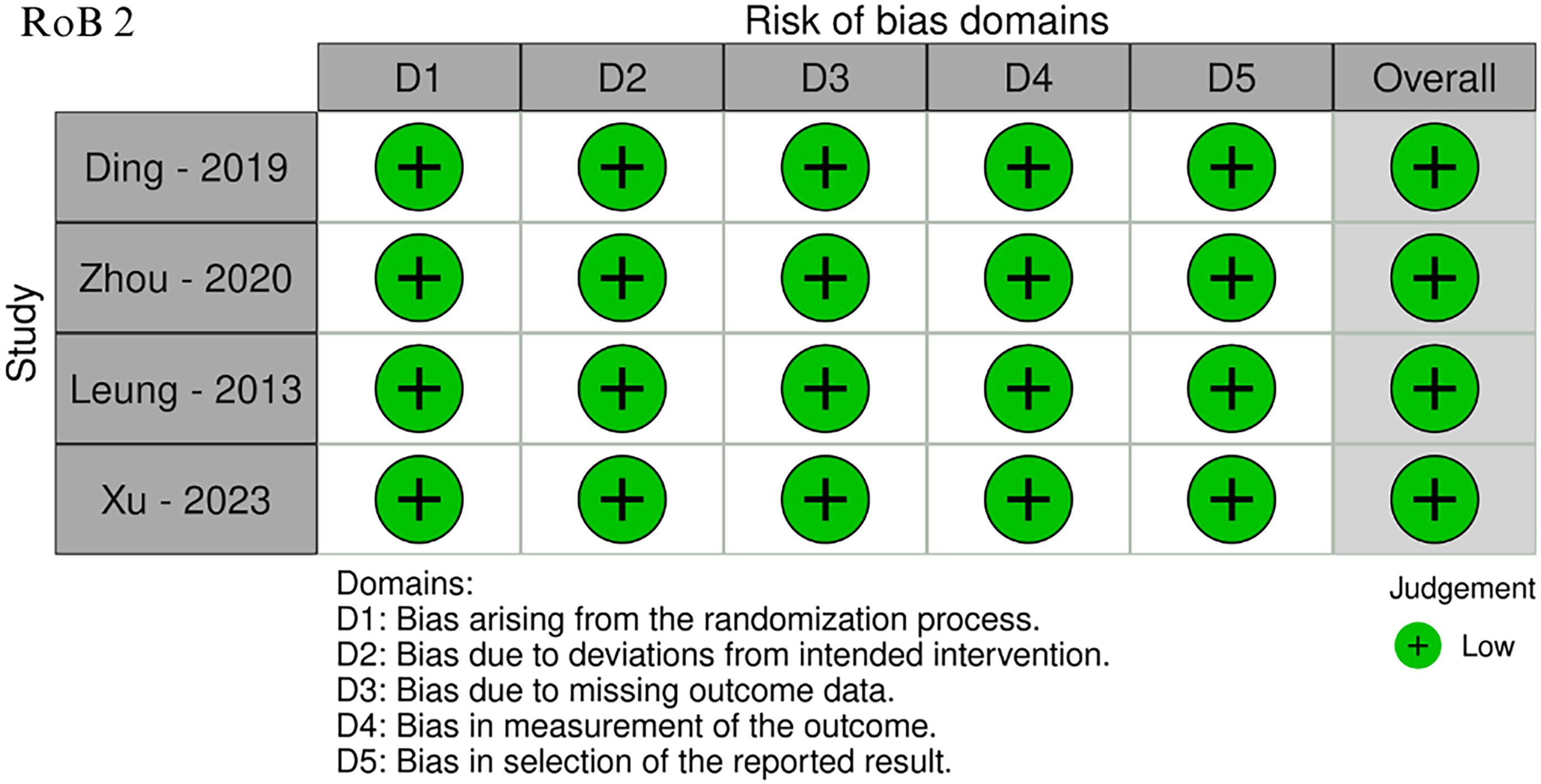
Critical appraisal of RCTs according to the Cochrane Collaboration’s tool for assessing risk of bias (Rob 2). RCT, randomized controlled trial.
Discussion
In this systematic review and meta-analysis, which included four RCTs with a total of 439 patients undergoing laparoscopic surgery for colorectal cancer, the NOSE procedure was associated with significantly reduced postoperative pain (VAS score), faster time to pass flatus, and lower SSI rates compared to conventional specimen extraction methods. However, operative time was significantly longer in the NOSE group. No significant differences were observed between the groups regarding bowel leaks, lymph nodes harvested, intraoperative blood loss, hospital stay duration, or local recurrence rates.
The short-term advantages of conventional laparoscopic surgery over open surgery, particularly in terms of reduced trauma and faster recovery, are well-established.12,13,18,19 However, with the continuous advancement of minimally invasive techniques, scarless surgeries, also known as total laparoscopic procedures, are gaining prominence.3–6,9,20 These approaches offer the potential to further improve outcomes related to wound complications, minimize pain, and enhance surgical recovery rates.
The concept of NOSE was first proposed by Franklin in 1993, introducing an innovative approach to minimize surgical trauma during specimen extraction.5,9 Later, the idea of NOTES was put forward by Kalloo et al. from Johns Hopkins University in 2004.3,20 NOSE encompasses a wide variety of approaches, including the oral cavity, vaginal, or anal routes, providing access to the abdominal cavity without visible incisions.3–6,9–11,20–24
Despite the advancements in minimally invasive procedures, conventional laparoscopic approaches still require a transabdominal incision to extract the surgical specimen.3–6,9–11,20–24 This additional step can increase postoperative pain and delay gastrointestinal recovery.3–6,9,20 For example, Wolthuis et al. conducted a RCT involving patients with diverticulitis and colorectal cancer, comparing laparoscopic NOSE colectomy to conventional laparoscopic colectomy. 12 Their findings demonstrated that NOSE significantly reduced postoperative pain and analgesic requirements, including lower morphine and paracetamol use. 12 Similarly, in a single-center study, Chang et al. evaluated NOSE in the context of reduced port laparoscopic surgery (RPLS-NOSE) for colorectal cancer, comparing it to conventional specimen extraction (RPLS-CSE). 10 Chang’s study revealed that NOSE not only significantly reduced analgesic use (33.9 versus 43.4 mg morphine; P = .011) but also alleviated postoperative pain. 10 These findings collectively underscore the benefits of NOSE in minimizing postoperative pain and enhancing recovery and align with the findings of our study. Furthermore, the reduced use of analgesics and opioids facilitates faster gastrointestinal transit recovery. When we compared the two techniques, we identified that NOSE was associated with shorter recovery times for ileus, consistent with findings from other studies.3–6,9–11,20–24
Operative time is a critical quality indicator in surgery, as longer procedures may be associated with an increased risk of postoperative complications. In our study, the NOSE group demonstrated longer operative times, likely due to the learning curve associated with the novel procedural steps. Similarly, Xu et al. in a propensity score-matched (PSM) analysis comparing NOSES and conventional laparoscopic colectomy for left-sided colorectal cancer, also reported a significantly longer operative time for NOSE (212.5 versus 178.0 minutes; P = .0001). 21 Consistent with these findings, Chang et al. observed similar trends in their studies.10,12 However, Zhao et al., using comparable PSM methodologies, did not find statistically significant differences in operative times.11,22,23 Furthermore, the appropriate handling of devices used for specimen extraction, such as flexible endoscopy instruments, Cai tubes, or endo-bags, may also contribute to longer operative times. It is important to note that not all surgical centers have access to these resources, which could limit the broader adoption of these techniques.
Our study demonstrated significantly lower rates of SSI, a key factor in wound complications.3–6 The absence of laparotomy in scarless surgeries is a major contributor to improved clinical outcomes related to wound healing.3–6 Some studies comparing open and minimally invasive surgeries highlight that similar complications can still arise when larger incisions are made.25,26 For instance, one study analyzed laparoscopic colon resection (LCR) and open colon resection (OCR) in 83 patients, with 37 undergoing LCR and 46 OCR. 25 It reported infection rates of 13.5% for LCR (10.8% at the extraction site, 2.7% at trocar sites) and 10.9% for OCR. 25 Incisional hernias were observed in 24.3% of LCR cases and 17.4% of OCR cases, with 85.7% of LCR wound complications linked to the extraction site. 25 Additionally, our meta-analysis focused on Eastern populations, where obesity, a key risk factor for wound complications, is less common. In Western populations with higher obesity rates, scarless surgeries like NOSE could reduce wound complications, health care costs, and future interventions. 27
Finally, it is reasonable to consider the potential risk of malignant cell contamination at the end of the procedure, which could theoretically compromise survival.3–6,9–11,20–24 However, Li et al. recently conducted a PSM study to evaluate the long-term oncologic outcomes of NOSE compared with conventional laparoscopic-assisted resection in rectal cancer patients. 24 Their findings revealed no significant differences in overall survival or disease-free survival between the groups. 24 Similarly, our results demonstrated no difference in 3-year local recurrence rates between the two approaches. These findings align with other studies, reinforcing that NOSES provides equivalent long-term oncologic safety to LAP while also offering notable short-term benefits.3–6,9–11,20–24
This study has limitations. First, although the included studies were randomized, they were conducted in Eastern populations, where risk factors such as obesity and other comorbidities differ significantly from Western populations and may influence the outcomes. Second, there was significant heterogeneity in some outcomes assessed, however, sensitivity analyses were performed, and mostly stable results were observed. Third, the lack of uniformity in surgical techniques and perioperative care protocols among the included studies may have contributed to variability in the outcomes. Fourth, the small sample size in some studies could limit the statistical power to detect differences in critical outcomes, particularly rare events such as long-term complications or recurrence rates. Fifth, the included studies often lacked data on functional outcomes, such as quality of life, continence, and sexual function, which are crucial for evaluating the overall impact of these procedures. Lastly, the follow-up duration in some studies may have been insufficient to capture long-term oncologic and functional results comprehensively. These limitations underscore the importance of conducting additional RCTs in diverse populations with standardized protocols and extended follow-up to provide more robust evidence and improve clinical decision-making.
Conclusion
In this systematic review and meta-analysis of RCTs with a total of 439 patients undergoing laparoscopic surgery for colorectal cancer, the NOSE procedure was associated with significantly reduced postoperative pain, faster gas passage time, lower SSI incidence, but longer operative time compared with conventional specimen extraction methods. No significant differences were observed between the groups regarding bowel leaks, lymph nodes harvested, intraoperative blood loss, hospital stay duration, or local recurrence rates.
Footnotes
Authors’ Contributions
Conception and design—B.F.P., F.B.F., and S.M.P.d.F. Data acquisition—B.F.P., L.S.d.S.P.G., L.S.G., and L.M.D. Data analysis—B.F.P., L.S.G., J.H.B., and L.S.d.S.P.G. Data interpretation—B.F.P., L.S.G., J.H.B., and L.S.d.S.P.G. Drafting and editing the article—B.F.P., J.H.B., and L.M.D. Revising it critically for important intellectual content—B.F.P., F.B.F., and S.M.P.d.F. All authors approved the final version of the article, including the authorship list.
Disclosure Statement
F.B.F. is a speaker for Janssen Brazil. All other authors report no relationships that could be construed as a conflict of interest. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Funding Information
No funding was received for this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.