
Abstract
Background:
The aging population has led to an increase in the prevalence of symptomatic paraesophageal hernias (PEHs), particularly among octogenarians. While elective repair is associated with improved outcomes compared to emergency repair, there are limited data on the safety and efficacy of robotic-assisted PEH repair in this high-risk population.
Methods:
We conducted a retrospective review of patients aged 65–89 who underwent robotic-assisted elective type IV PEH repair by a single surgeon at Mount Sinai Medical Center from 2020 to 2023. Patients were divided into two cohorts: octogenarians (80–89 years) and seniors (65–79 years). Demographics, perioperative outcomes, and complications were analyzed.
Results:
A total of 38 patients were included, with 15 octogenarians and 23 seniors. The mean ages were 84 ± 2 years and 73 ± 5 years, respectively. The majority of patients were female (73% octogenarians, 87% seniors), and the average body mass index was comparable between cohorts (25 kg/m2 ± 3.7 versus 25 ± 4.7). The mean hospital length of stay was 2.7 ± 1.8 days for octogenarians and 2.4 ± 1.8 days for seniors (P = .6). No intraoperative complications or 30-day mortality occurred. Two octogenarians (13%) and three seniors (13%) were readmitted within 30 days. At 6 months, 87% of octogenarians and 69% of seniors reported resolution of preoperative symptoms (P = .3).
Conclusions:
Robotic-assisted repair of type IV PEHs is a safe and effective option for both octogenarians and seniors. The absence of intraoperative complications and 30-day mortality supports its feasibility in elderly patients, including those in their eighth decade of life. These findings advocate for elective minimally invasive repair in carefully selected patients, regardless of advanced age, and highlight the importance of further studies to validate long-term outcomes.
Introduction
Background
The rising number of elderly individuals globally is associated with an increased prevalence of symptomatic paraesophageal hernias (PEHs). By 2050, the number of individuals aged 80 and older is expected to triple compared to 2019.1–3 PEHs are often asymptomatic, but when symptoms occur, they include heartburn, chest pain, regurgitation, early satiety, chronic anemia, and dysphagia. Laparoscopic PEH repair has been shown to significantly and durably improve gastrointestinal symptoms over a 5-year period.4–6 Additionally, PEH repair is associated with improved quality of life in octogenarians, provided patients are carefully selected and optimized preoperatively.7–9
Historically, elective PEH repair was recommended regardless of symptoms due to concerns about progression to acute presentations, which have high mortality rates. Mortality rates for emergency repairs range from 5% to 50%, compared to 0.5%–3% for elective repairs, making the timing of intervention critical.10–12 However, the management of PEHs in elderly populations remains debated. While some recent studies advocate for elective surgery as safe in octogenarians, others continue to support watchful waiting, citing surgical risks in this age group.13,14
A pivotal analysis in 2005 revealed significant contrasts in outcomes for octogenarians based on timing of intervention: mortality rates were 2.5% for elective repairs and 16% for nonelective repairs. More recent data confirm that nonelective paraesophageal hernia repairs remain strongly predictive of poor outcomes, including higher mortality, increased complications, longer hospital stays, and more frequent readmissions. Notably, octogenarians undergoing elective PEH repair fare better than those undergoing nonelective procedures, highlighting the importance of timely intervention.15,16
Minimally invasive repair is generally favored for its lower morbidity and mortality rates. Importantly, octogenarians remain underrepresented in current studies, necessitating further research to optimize surgical strategies and assess both operative and symptomatic outcomes. 17 These findings collectively support a proactive approach to paraesophageal hernia repairs in octogenarians, emphasizing elective repair with comprehensive preoperative assessment to improve patient outcomes and quality of life.
Rationale and knowledge gap
Given the aging population and the increasing prevalence of PEHs, further research is necessary to determine the safety and feasibility of robotic-assisted paraesophageal hernia repair (PEHR) in elderly patients, especially octogenarians. While minimally invasive surgery is favored for its lower morbidity and mortality rates, evidence on its application in this age group remains limited. A comprehensive analysis of outcomes in octogenarians undergoing robotic-assisted PEHR is essential to inform clinical decision-making and guide future studies.
Objective
This study aims to evaluate the safety and efficacy of robotic-assisted elective repair of type IV PEH in octogenarians compared to younger seniors. By analyzing perioperative outcomes, complications, and readmission rates, this study seeks to provide insights into the role of minimally invasive techniques in addressing this growing clinical challenge in an aging population.
Methods
We conducted a retrospective, chart-based review of all patients who underwent robotic-assisted type IV PEH repair from 2020 to 2023 by a single surgeon at Mount Sinai Medical Center (MSMC) in Miami Beach, Florida. This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the MSMC Institutional Review Board with waiver of informed consent due to minimal risk to participants; Federalwide Assurance Number FWA00000176. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Patient characteristics reviewed included age, sex, ethnicity, body mass index (BMI), preoperative workup, symptomatology, operative time, intraoperative and postoperative complications, hospital length of stay (LOS), and pre- and postoperative imaging. Those patients who underwent laparoscopic repair or those patients who did not have a type IV paraesophageal hernia were excluded.
Surgical Procedure
All procedures were performed by one thoracic surgeon between June 2019 and December 2023. The da Vinci Xi platform was used for all cases (Intuitive Surgical, Sunnyvale, California). Entry into the abdomen was performed using an Optiview trocar in the periumbilical region. Additional ports were placed in the left upper quadrant near the peritoneal reflection, one equidistant from prior ports, one in the right upper quadrant, and an assistant port in the right lower quadrant; a subxiphoid 5 mm incision was used for the Nathanson liver retractor. The robotic arms were routinely armed with the Cardiere forceps, camera, vessel sealer, and curved bipolar. Endo cigars were used for the mobilization of intrabdominal organs to avoid any injuries. The dissection began at the phrenoesophageal membrane until the level of the inferior pulmonary veins. The anterior and posterior vagus nerves were identified and preserved. Thereafter, the pars flaccida was opened, and the right crus was dissected, taking care to preserve the peritoneal lining. This area was dissected cephalad to meet the previously dissected anterior plane. A retroesophageal window was created for the passage of a Penrose drain to aid in retraction. The greater curvature was mobilized using the vessel sealer. We performed circumferential dissection of the esophagus until at least 3 cm of intraabdominal esophagus was obtained.
To facilitate a tension-free repair, we often placed a trocar into the fourth intercostal space to create a capnothorax that in turn created a floppy diaphragm. A composite cruroplasty (posterior and anterior) was performed with a bougie in place using a nonabsorbable 0 V-loc suture in a running fashion and secured with felt pledgets and hem-o-lok clips. Preoperative reflux symptoms and esophageal motility dictated whether an anterior gastropexy or fundoplication was performed. A chest x-ray was performed in the operating room prior to extubation to ensure proper lung expansion with no residual pneumothorax or pneumomediastinum.
Perioperative management
Patients underwent a comprehensive preoperative evaluation during their clinic visit, which included a detailed history and physical examination to assess symptoms, overall functional status, and medical comorbidities. The diagnostic workup consisted of chest and abdominal computed tomography, esophagram, and esophagogastroduodenoscopy to evaluate the hernia and related anatomy. Preoperative preparation involved a liquid diet for 48 hours, transitioning to clear liquids 24 hours before surgery. Additionally, bowel preparation was achieved using magnesium citrate the day prior to the procedure. All patients underwent routine esophagram on postoperative day one.
Statistical analysis
Continuous data were compared using Student’s t-test, and a P < .05 was considered statistically significant. Data were analyzed using Microsoft Office Excel (Microsoft, Redmond, WA, USA). Data are expressed as n, percentage, or as the mean ± standard deviation.
Results
Between 2019 and 2023, a total of 38 patients underwent robotic-assisted elective repair of type IV PEHs at our institution. Of these, 15 patients (39%) were octogenarians aged 80–89 years, and 23 patients (61%) were seniors aged 65–79 years. The mean age in the octogenarian cohort was 84 ± 2 years, while the senior cohort had a mean age of 73 ± 5 years. The majority of patients in both groups were female, accounting for 73% of the octogenarian cohort and 87% of the senior cohort. The average BMI was similar between the two groups, with a mean of 25 kg/m2 ± 3.7 in the octogenarian cohort and 25 ± 4.7 in the senior cohort. Patient demographics are shown in Table 1. In the octogenarian cohort, most patients underwent gastropexy, with only 13% (2/15) receiving fundoplication. In contrast, 43% (10/23) of patients in the senior cohort underwent fundoplication, reflecting a greater utilization of this technique in the younger age group (P = .05). The mean hospital LOS was 2.7 ± 1.8 days for octogenarians and 2.4 ± 1.8 days for seniors, with no statistically significant difference (P = .6). There were no intraoperative complications, 30- or 90-day mortalities. Two octogenarians (13%) and three seniors (13%) were readmitted within 30 days. Readmissions were due to pulmonary embolism, syncope, intolerance of oral intake, and ileus. At 6-month follow-up, symptom resolution was reported by 87% of octogenarians and 69% of seniors (P = .3). Perioperative outcomes are depicted in Figure 1.
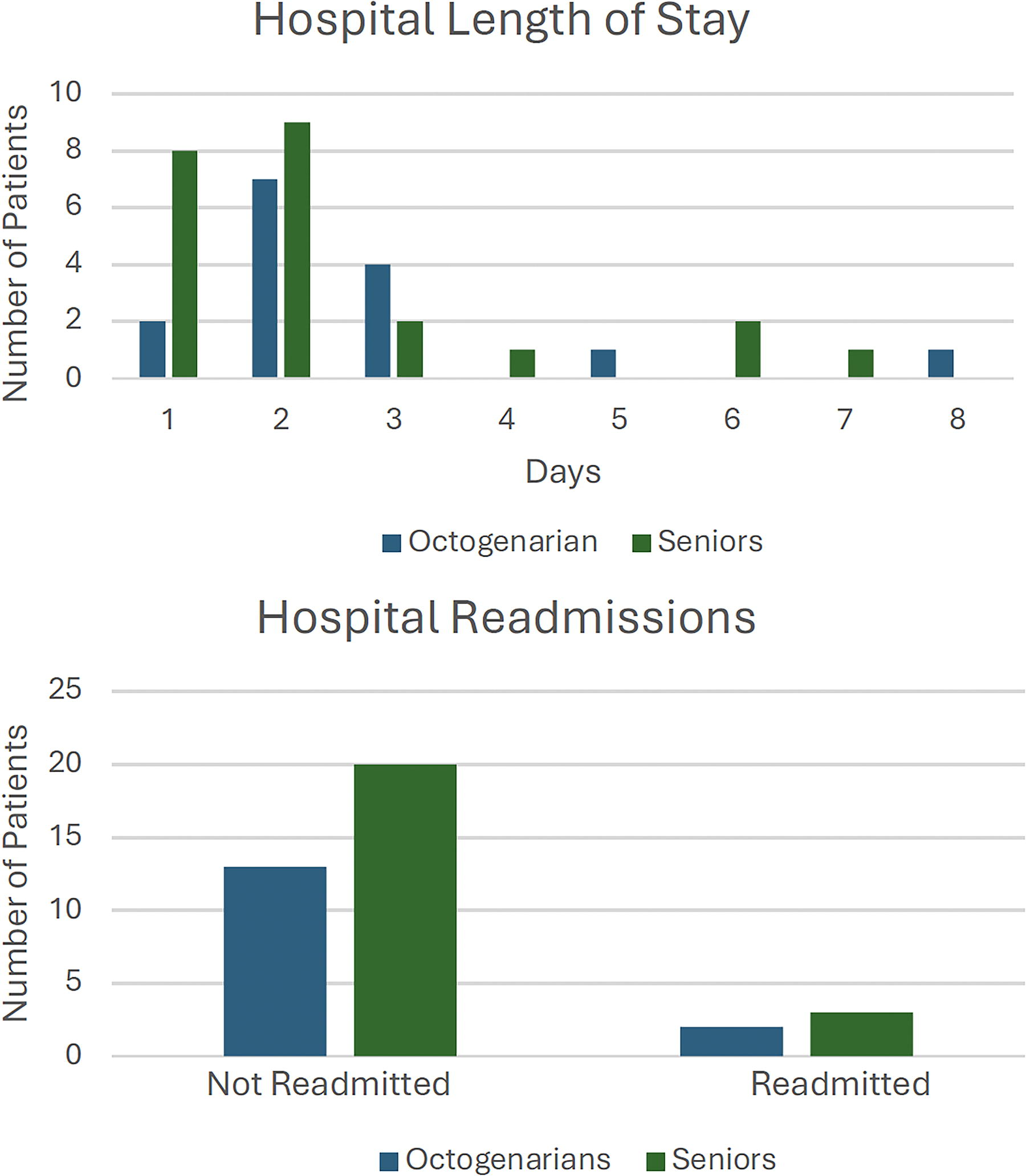
Perioperative outcomes including hospital length of stay and 30-day readmissions.
Patient Demographics
Variables are reported as mean ± standard deviation or as % (n).
Discussion
This study demonstrates that robotic-assisted type IV PEH repair is safe and effective for both octogenarians and seniors. The absence of intraoperative complications and low 30-day morbidity support the feasibility of minimally invasive techniques in carefully selected elderly patients. Robotic platforms may contribute to favorable outcomes by enabling meticulous dissection and reducing surgical trauma. The comparable LOS and symptom resolution rates between age groups suggest that chronological age should not preclude elective repair.
The study’s strengths include a focus on a homogeneous patient population, consistent surgical techniques performed by a single thoracic surgeon, and the use of advanced robotic-assisted methods. However, the study is limited by its retrospective nature, small sample size, and single-center setting, which may reduce generalizability. Additionally, the cohorts were relatively small, which may limit statistical power for detecting subtle differences between age groups.
This study supports the growing evidence that robotic-assisted paraesophageal hernia repair is a safe and effective approach for elderly patients, including octogenarians. With the aging population, this procedure could become a critical tool for addressing the increasing prevalence of symptomatic hernias in older adults. Future studies should focus on larger, multicenter cohorts and include long-term follow-up to further validate these findings and assess recurrence rates. Additionally, incorporating cost-effectiveness analysis could strengthen the case for the widespread adoption of robotic-assisted techniques in this population.
Conclusions
Robotic-assisted repair of type IV PEH is a feasible, safe, and effective option for both octogenarians and seniors. The outcomes demonstrate low perioperative morbidity with no mortality in either cohort, supporting the use of robotic platforms for managing complex hernias in elderly patients. These findings highlight the potential of minimally invasive approaches to improve surgical care for the aging population and advocate for their consideration in elective repair of PEH in carefully selected patients, regardless of age.
Footnotes
Authors’ Contributions
Conception and design: J.E.W. and F.M.S. Provision of study materials or patients: F.M.S. Collection and assembly of data: F.A. and J.E.W. Data analysis and interpretation: F.A., J.E.W., and F.M.S. Administrative support, article writing, and final approval of article: all authors.
Disclosure Statement
All authors have completed the ICMJE uniform disclosure form. The authors have no conflicts of interest to declare. The TREND reporting checklist has been completed. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The authors have no disclosures or conflicts of interest.
Funding Information
No funding was provided for this work.