
Abstract
Introduction:
The analysis of postoperative pain has gained prominence as an important outcome following inguinal hernia repair (IHR), and various strategies have been employed. However, the use of erector spinae plane block (ESPB) in IHR is debated. Therefore, this systematic review and meta-analysis evaluates their efficacy.
Methods:
We searched PubMed, Embase, Cochrane, and Web of Science for randomized controlled trials (RCTs), comparing the impact of ESPB on pain outcomes following IHR. Outcomes included pain using the visual analog scale (VAS) at 2, 6, 12, and 24 hours after surgery and postoperative nausea and vomiting (PONV) rates. Statistical analyses were performed using R software and trial sequential analysis.
Results:
We included three RCTs comprising 145 patients, of which 66 (45.5%) were submitted to ESPB. Between the included studies, two analyzed minimally invasive IHR, while one analyzed the open Lichtenstein technique. We found no differences in VAS pain scores at 2 hours (MD: −0.56; 95% CI: [−3.53; 2.42]; P = .71) and at 6 hours (MD: −1.13; 95% CI: [−2.50; 0.23]; P = .1) postoperatively. Also, no clinically or statistically significant differences were found in the VAS score for ESPB at 12 hours (MD: −0.96; 95% CI: [−1.94; −.02]; P = .051) and 24 hours postoperatively (MD: −0.19; 95% CI: [−0.53; .15]; P = .28). No statistically significant differences were found in PONV rates between the groups (7.6% versus 20.3%; RR 0.38; 95% CI: [0.14; 1.0]; P = .05).
Conclusion:
This meta-analysis found no differences in postoperative pain scores or PONV between the ESPB and control groups. Further studies are necessary to better understand the role of ESPB in inguinal hernia repair.
Introduction
Managing postoperative pain has become a crucial aspect of surgical care, particularly in the context of inguinal hernia repair (IHR). 1 Effective pain control enhances patient comfort and improves recovery outcomes, including reduced hospital stays and faster return to daily activities. 2 As such, the analysis of postoperative pain has gained prominence as a significant outcome following IHR.
Various strategies have been developed to address the complex nature of postoperative pain, with multimodal analgesia serving as a key component of the enhanced recovery after surgery protocol. 3 Within this multimodal framework, nerve blocks have emerged as an essential component due to their ability to provide targeted pain relief while preserving systemic hemodynamic stability. 4 One such nerve block that has garnered attention is the erector spinae plane block (ESPB). This interfacial plane block has several advantages over traditional neuraxial and peripheral nerve blocks, 5 with associated low complication rates, minimal hemodynamic alterations, and fewer contraindications, making it a viable option for patients who may not be candidates for neuraxial anesthesia. 6
Despite its growing use, the analgesic efficacy of ESPB in the specific context of IHR has not been systematically evaluated. To address these uncertainties, we conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to assess the role of ESPB in postoperative pain management for IHR. Our study aims to clarify comprehensive insights into the potential benefits and limitations of ESPB, thereby informing evidence-based clinical practice and guiding future research efforts in this domain.
Methods
Eligibility criteria
This systematic review and meta-analysis were performed and reported by the Cochrane Collaboration Handbook for Systematic Review of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement guidelines.7,8
Inclusion in this meta-analysis was restricted to studies that met all the following eligibility criteria: (1) RCTs; (2) comparing ESPB versus no block; (3) in patients undergoing IHR; (4) reporting postoperative pain via the visual analog scale. We excluded studies with overlapping patient populations, studies analyzing the use of ESPB for other abdominal surgeries, as well as case reports, case series, review articles, retrospective data analysis, or nonrandomized prospective studies. Outcomes of interest included pain using the VAS at 2, 6, 12, and 24 hours after surgical procedure and postoperative nausea and vomiting (PONV) rates.
Search strategy and data extraction
We systematically searched PubMed, Embase, Web of Science, and Cochrane Central Register of Controlled Trials from inception to April 2024 with the following search terms: “Erector Spinae,” “ESPB,” “Inguinal hernia,” “groin hernia,” “femoral hernia.”
The references from all included studies, previous systematic reviews, and meta-analyses were also manually searched for additional studies. Two authors (C.O. and C.S.) independently extracted the data following predefined search criteria and quality assessment. Any discrepancy was resolved by discussion in a consensus meeting among the authors. The prospective meta-analysis protocol was registered on PROSPERO on January 19, 2024, under protocol CRD42025635933.
Endpoints and subanalyses
The Primary Outcome included postoperative pain at 2, 6, 12, and 24 hours after surgical repair using the VAS, and the secondary endpoint included PONV rates after the procedure. No subgroup analysis was performed in the course of this work due to data availability.
Quality assessment
We evaluated the risk of bias in randomized studies using version 2 of the Cochrane Risk of Bias assessment tool (RoB 2). 9 Two independent authors (C.O. and A.S.) completed the risk of bias assessment. After discussing the reasons for the discrepancy, disagreements were resolved through consensus.
Publication bias was investigated by funnel plot analysis of point estimates in relation to study weights. Missing means and standard deviations were estimated from medians and interquartile ranges by applying the method by Wan and Luo. 10 Furthermore, where data were only available in graphical format, Webplotdigitizer version 3.9 was used as a tool for data extraction. 11
Statistical analysis
Mean difference (MD) with 95% confidence intervals (CIs) was used to compare treatment effects for continuous endpoints and risk ratio (RR) with 95% CI was used to compare treatment effects for dichotomous endpoints between the two treatment arms. Weighted treatment effects were calculated using a random effects model. We used Cochran’s Q test and I2 statistics with 95% CIs to evaluate for heterogeneity. 12 Endpoints were considered to have low heterogeneity if P > .10 and I2 < 30%, moderate heterogeneity if I2 between 30% and 75%, and high heterogeneity if I2 > 75%. In outcomes with high heterogeneity, pooled estimates were computed with DerSimonian and Laird random-effects model. Statistical analyses were performed with RStudio version 4.3.1 (R Foundation for Statistical Computing) and trial sequential analysis (TSA) Software 0.9.5.10 Beta (Copenhagen Trial Unit, Center for Clinical Interventional Research) for TSA evaluation with an estimated risk of type 1 error at 5% and 80% power.13–16
Results
Study selection and characteristics
The initial search yielded 845 results. After removing duplicate records and ineligible studies, 11 remained and were thoroughly reviewed based on inclusion criteria. Of those, three studies were included, comprising 145 patients from 3 RCTs (Fig. 1).
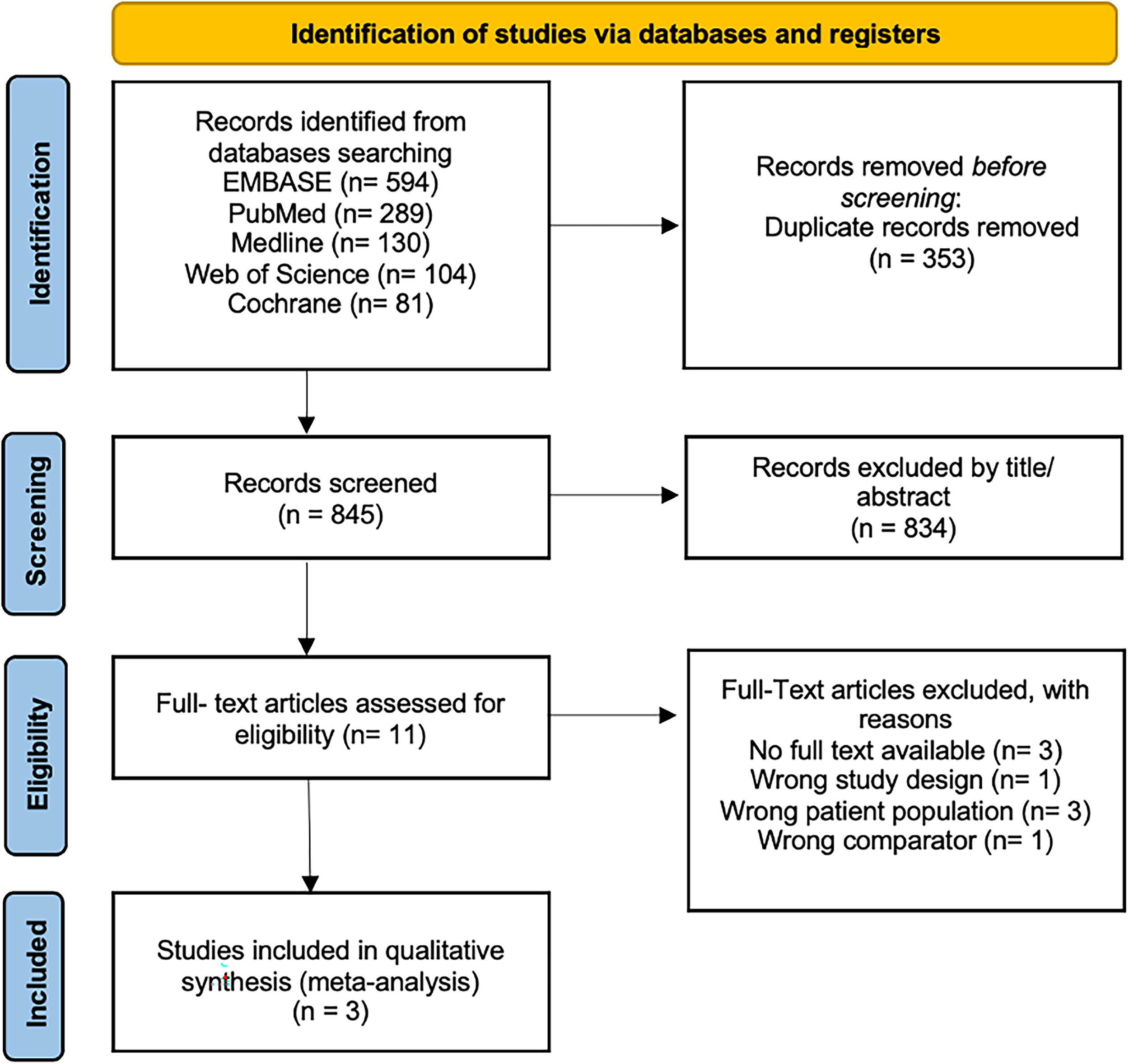
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only.
A total of 66 (45.5%) patients were submitted to ESBP. Study characteristics are reported in Table 1. Significant between-study variability existed regarding surgical technique, components of the control and intervention groups, and the methods used for postoperative pain measures. Two studies assessed minimally invasive surgical IHR,17,18 and one assessed the open Lichtenstein technique. 19 One article compared ESPB with saline, 18 one compared with no intervention, 17 and one used spinal anesthesia in both the control and interventional group, 19 adding the ESPB in the interventional group. Two studies assessed postoperative pain using the VAS,18,19 and one assessed using a numerical rating scale. 17
Baseline Characteristics of Included Studies
Mean.
ASA, American Society of Anesthesiologists; BMI, body mass index; ESPB, erector spinae plane block; TAPP, transabdominal preperitoneal; TEP, totally extraperitoneal.
Pooled analysis of all studies
The overall analysis demonstrated no statistically significant results regarding pain using the VAS at 2 hours (MD: −0.56; 95% CI: [−3.53; 2.42]; P = .71; I2 = 95%; Fig. 2), 6 hours (MD: −1.13; 95% CI: [−2.50; 0.23]; P = .1; I2 = 83%; Fig. 3), 12 hours (MD: −0.96; 95% CI: [−1.94; −0.02]; P = .051; I2 = 79%; Fig. 4), and 24 hours (MD: −0.19; 95% CI: [−0.53; 0.15]; P = .28; I2 = 0%; Fig. 5) after surgical repair. In addition, no statistically significant differences were found in PONV rates between the groups (7.6% versus 20.3%; RR 0.38; 95% CI: [0.14; 1.0]; P = .05; I2 = 0%; Fig. 6).

Pain 2 hours after surgery using a visual analog scale was not significant between groups in the overall analysis.

Pain 6 hours after surgery was not significant between groups in the overall analysis.

Pain 12 hours after surgery was not significant between groups in the overall analysis.

Pain 24 hours after surgery was not significant between groups in the overall analysis.
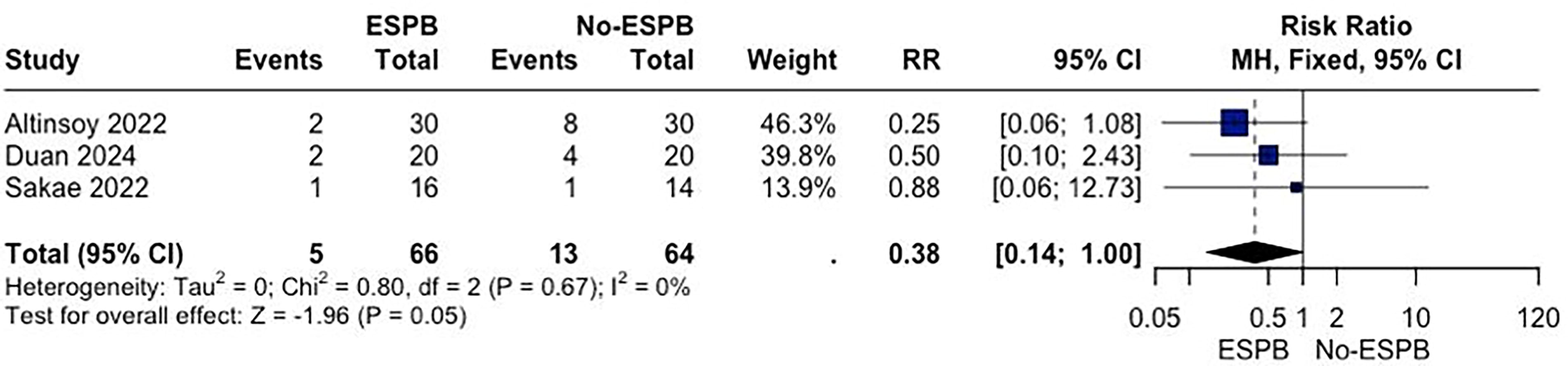
Postoperative nausea and vomiting rates were not significant between groups in the overall analysis.
Quality assessment
In the overall analysis, the TSA did not achieve the required information size (RIS) for postoperative pain 2, 6, 12, and 24 hours using the VAS, indicating that future studies are needed to confirm these findings (Supplementary Fig. S1, S2, S3, and S4). Similarly, the RIS was not met for PONV rates (Supplementary Fig. S5).
The Risk of Bias 2 (RoB 2) tool was used for the quality assessment of RCTs. No studies were considered at high risk of bias, as described in Supplementary Figure S6 in the Supplementary Appendix.
On funnel plot analysis for pain 24 hours after surgery, studies occupied symmetrical distribution according to weight and converged toward the pooled effect as the weight increased (Supplementary Fig. S7).
Discussion
This systematic review and meta-analysis comprising 145 patients from 3 RCTs evaluated the analgesic impact of ESPB in IHR. The general analysis revealed that the nerve block was not associated with a significant difference in pain scores after surgery using the VAS, just as PONV rates between patients. The TSA indicated that the RIS was not achieved for the assessed outcomes, suggesting that further studies are needed to draw definitive conclusions for this population.
The ESPB was first described in 2016 for the treatment of thoracic neuropathic pain, 20 when studies started analyzing the use of ESPB first at thoracic levels. Recently, it has been trialed for intraoperative analgesia in abdominal surgery with promising results, reducing the need for intravenous anesthesia 21 and decreasing postoperative pain and rescue analgesia. Postoperative discomfort represents a significant concern, as it can lead to increased opioid consumption for uncontrolled pain, not only impairing recovery but also increasing the risk of opioid-related complications, including respiratory depression, nausea, ileus, medication abuse, hyperalgesia, and chronic pain.22,23 Consequently, effective measures are needed to reduce those factors and increase patient’s comfort after procedures.
Few studies describing a case series demonstrated that patients undergoing open or laparoscopic abdominal surgeries such as VHR with ESPB could be associated with a decreased necessity for opioid rescue postoperatively.6,21 These findings are similar to the ones found in two RCTs included in our study, showing that the benefits of ESPB could also be extended to laparoscopic IHR, resulting in pain management improvements, reduced reliance on anesthetic drugs, and potentially enhanced patient recovery experience.17,18
ESPB was also demonstrated to have better hemodynamic stability for the patients. According to Cherukuri Kaushik et al., (2022), 24 the group using ESPB and general anesthesia had a remarkable reduction in systolic and diastolic blood pressures. They had a reduction in the requirement of analgesic and inhaled agents when compared to the group with general anesthesia alone.
However, one RCT evaluating 45 patients on ESPB for open IHR showed that the nerve block was considered an ineffective technique for providing postoperative analgesia, and there were no statistically significant differences in the mean values of VAS scores. 19 Our meta-analysis demonstrated similar results, including the rates of PONV between groups. However, these findings may be explained by the small population size, short follow-up period, variations in medication regimens, and surgical techniques, emphasizing the need for further studies to understand the role of the ESPB in IHR.
This study has several limitations. First, the relatively small number of studies and patients limits the generalizability of our findings. The included studies exhibited significant heterogeneity, particularly in the postoperative pain rates using the VAS, which could influence the results. Second, variations in study design, patient characteristics, follow-up periods, and surgical techniques may also affect the applicability of our conclusions to clinical practice. Nevertheless, we were able to perform a sensitivity analysis of all the included outcomes.
Conclusion
In conclusion, our systematic review and meta-analysis showed that the analgesic impact of ESPB during IHR is not associated with significant differences related to postoperative pain score and PONV rates compared to no nerve block, highlighting the need for further studies evaluating this patient population.
Footnotes
Authors’ Contributions
The authors included each contributed significantly to this research as per the guidelines of the International Committee of Medical Journal Editors (ICMJE). Study design: C.N.B.d.O., A.G.e.S., C.A.B.d.S., J.P.G.K., D.C., D.L.L., and F.M. Data collection and analysis: C.N.B.d.O., A.G.e.S., C.A.B.S., J.P.G.K., and D.L.L. Manuscript preparation and editing: C.N.B.d.O., A.G.e.S., C.A.B.d.S., J.P.G.K., D.C., D.L.L., and F.M.
Author Disclosure Statement
C.N.B.O., A.G. S., C.A.B.S., J.P.G.K., D.C., and D.L.L. have no conflict of interest. F.M. discloses consulting fees from BD, Intuitive, Integra, DeepBlue, and Allergan & Medtronic, outside the submitted study.
Funding Information
There was no funding for this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.