
Abstract
Background:
Indocyanine green (ICG) florescence cholangiography is a method to help recognize biliary structures during cholecystectomy. However, the optimal dosage and timing of ICG injection are still under investigation, and there is no consensus internationally. Previous studies revealed the use of various dosages of ICG, ranging from 0.05 mg/kg to 7.5 mg regardless of body weight, while it was revealed that the majority of the quality of ICG cholangiography was suboptimal, i.e., grade B/C. Recently, it has been advocated the use of much diluted ICG, as a higher dose might result in over-detection of adjacent structures, making the biliary tract more difficult to distinguish from its surroundings. This study aimed to investigate the efficacy and safety of a super-diluted intravenous dose, 0.025 mg, given on induction of general anesthesia, for ICG cholangiography in cholecystectomy.
Methods:
From 19th December 2024 to 14th February 2025, ICG cholangiography was performed with intravenous ICG .025 mg on induction of general anesthesia in all cholecystectomies in a hepatobiliary team. Grading of ICG cholangiography was observed.
Results:
Totally 18 patients underwent cholecystectomy with ICG cholangiography performed. Sixteen out of 18 (88.9%) ICG cholangiographies were grade A. Two (11.1%) ICG cholangiograpies were grade B. Two (11.1%) patients required conversion to open surgery. There was no bile duct injury.
Conclusions:
High-quality ICG cholangiography can be safely performed in cholecystectomy with a single-shot intravenous 0.025 mg ICG on induction of general anesthesia.
Background
Bile duct injury is a severe complication in cholecystectomy. It has been shown that many cases of bile duct injury were due to poor visualization and misidentification of anatomical structures. Indocyanine green (ICG) florescence cholangiography is a method to help surgeons in the recognition of biliary structures during cholecystectomy. However, it is not adopted worldwide in standard cholecystectomy, as the optimal dosage and timing of ICG injection are still under investigation, and there is no consensus internationally. Previous studies revealed the use of various dosages of ICG, ranging from 0.05 mg/kg to 7.5 mg, regardless of body weight.1–23 Time of injection also varies from 20 hours before the operation, to just before the operation or intraoperatively.1–23
A single-center randomized controlled trial was published by She et al. in 2022 19 with the use of 3.5 mg intravenous ICG 30 minutes before general anesthesia for emergency cholecystectomy. Cholangiography was graded A, B, and C in comparison of contrast between biliary tract and liver (A: contrast of biliary tract stronger, B: biliary tract and liver similar, and C: contrast of liver stronger). The result found that majority (60.9%) of the quality of ICG cholangiography was suboptimal, i.e., grade B/C, while only 39.1% was grade A.
Recently, it has been advocated the use of much diluted ICG, as a higher dose might result in over-detection of adjacent structures, making the biliary tract more difficult to be distinguished from its surroundings.
Objectives
This study aimed to investigate the efficacy and safety of a super-diluted intravenous dose, 0.025 mg, given on induction of general anesthesia, for ICG cholangiography in cholecystectomy.
Methods
From 19th December 2024 to 14th February 2025, ICG cholangiography was performed in all cholecystectomies in a hepatobiliary team in the Department of Surgery in the New Territories West Cluster (NTWC) of the Hospital Authority in the Hong Kong Special Administrative Region, China. Operations were performed in two hospitals (Tuen Mun Hospital and Pok Oi Hospital) in the NTWC. In our center, our hepatobiliary team would usually perform cholecystectomies with prior biliary complications (e.g., prior cholecystitis, cholangitis, pancreatitis) and gallbladder neoplasm, while cholecystectomies without prior complications (e.g., symptomatic gallstones) would usually be performed by the general surgical teams.
Apart from the use of fluorescence imaging system, cholecystectomy was performed as usual. All procedures were started with a laparoscopic approach and would be converted to open surgery, if necessary, as clinically judged by the operating surgeons. All procedures were performed by a surgical fellow (with at least 7 years of surgical training) or performed by a higher surgical trainee (with at least 3 years of surgical training), who is supervised by a surgical fellow.
Three endoscopic fluorescence imaging systems were used. One was the VISERA ELITE II 10 mm IR Telescope (Olympus Corporation, Tokyo, Japan). The second one was HOPKINS RUBINA 30° NIR/ICG 10 mm Fluorescence Imaging (Karl Storz SE, Tuttlingen, Germany). The third one was the Stryker 10.0 mm 30° AIM HD Autoclavable Laparoscope, 33 cm (Stryker Corporation, Kalamazoo, Michigan, USA). Surgeons were allowed to freely switch between white-light color images and fluorescence images during the operation.
A vial of 25 mg ICG was diluted into 0.025 mg with normal saline and was injected intravenously on induction of general anesthesia (Fig. 1), followed by a 5 mL normal saline flush. No repeated dose of ICG was used. Intravenous antibiotics were given as usual.
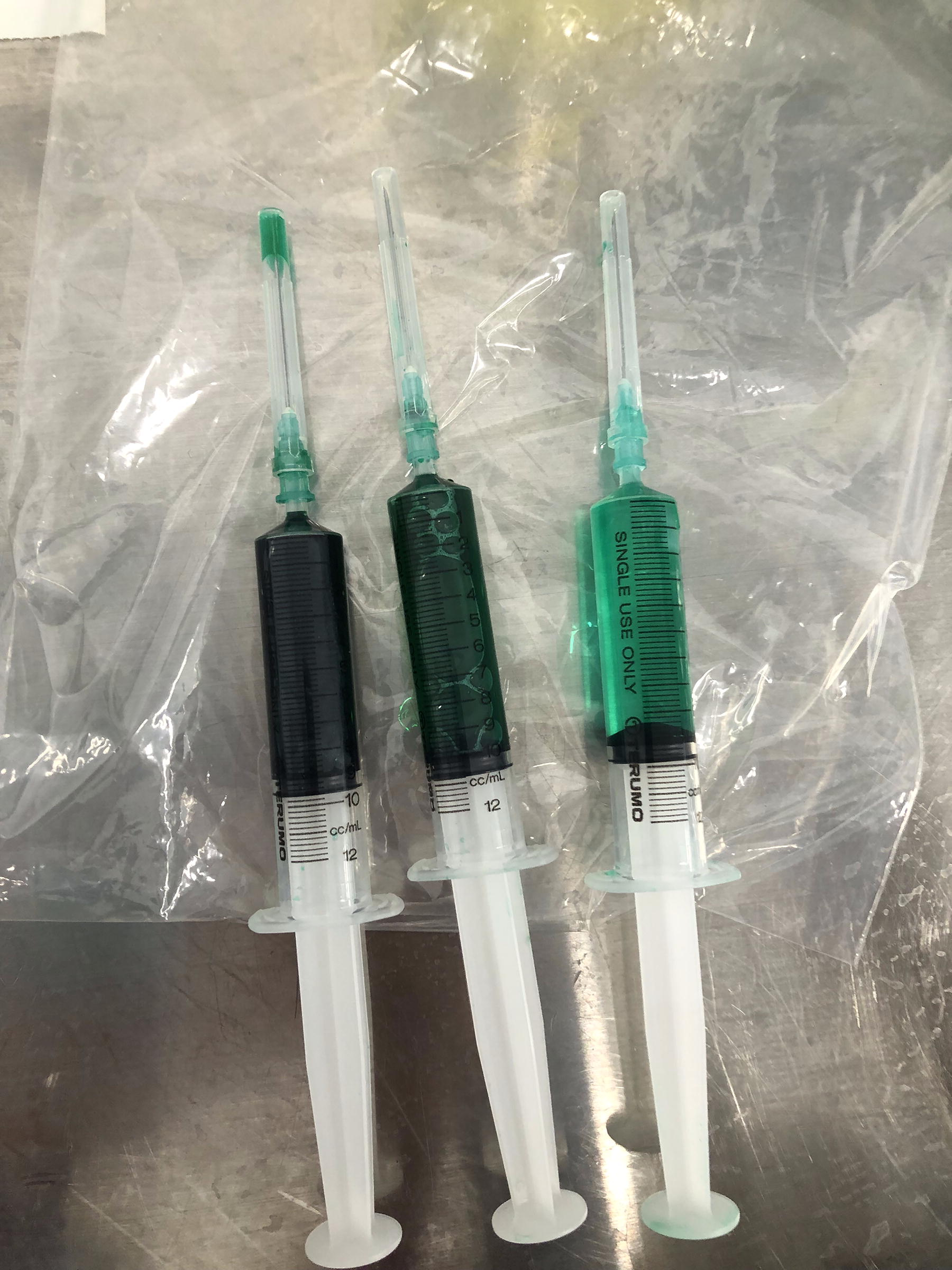
Left: 25 mg in 10 mL normal saline; middle: further dilution with normal saline to 2.5 mg in 10 mL; right: further dilution with normal saline to 0.25 mg in 10 mL, and 1 mL (0.025 mg) was injected.
Outcomes including grading of cholangiography (grade A/B/C) (Fig. 2, Fig. 3), time to identify biliary structure (common bile duct or cystic duct), operation time, rate of conversion to open surgery, reasons for conversion, hospital stay, and bile duct injury were observed.

Grade A cholangiography, contrast stronger in biliary structure than in liver; this cholangiography showed a long cystic duct with low insertion to the common bile duct.

Grade C cholangiography, contrast stronger in liver than in biliary structure; this cholangiography was obtained during a synchronized left hemicolectomy and cholecystectomy for colorectal cancer and gallbladder neoplasm, in which 7.5 mg intravenous ICG was injected by the colorectal surgeons for colonic anastomosis 1 hour before cholecystectomy.
Results
A total of 18 patients underwent cholecystectomy in the study period. ICG cholangiography was performed in all patients. Two of them were emergency cholecystectomies for acute cholecystectomy, while others were elective cholecystectomies. Indications for elective cholecystectomy included interval cholecystectomy for previous acute cholecystitis, common bile duct stone requiring endoscopic retrograde cholangiopancreatography, biliary pancreatitis, large gallbladder polyp/neoplasm, and porcelain gallbladder. (Table 1)
Indication of Cholecystectomy; PTC, Percutaneous Transhepatic Cholecystostomy; ERCP, Endoscopic Retrograde Cholangiopancreatography
The mean age of patients was 59.8 years old (39–74). Ten of them (55.6%) were male, while 8 of them (44.4%) were female.
Sixteen out of 18 (88.9%) ICG cholangiographies were grade A. 2 out of 18 (11.1%) ICG cholangiographies were grade B. There was no grade C ICG cholangiography. Mean time to identify biliary structure was 33.3 (20–70) minutes. Mean operation time was 90.9 (30–164) minutes.
Two patients (11.1%) required laparoscopic converted to open cholecystectomy due to dense peritoneal adhesion from previous laparotomy and dense adhesion at Calot’s triangle, respectively. The mean hospital stay was 2.4 (1–6) days. There was no bile duct injury.
As shown in the Supplementary Video, the use of ICG cholangiography in a case of laparoscopic cholecystectomy was illustrated. The indication for this operation was porcelain gallbladder. The gallbladder was dumbbell-shaped on laparoscopic view, and there were marked thickening and hardening at its midbody. ICG cholangiography was performed, and the common bile duct showed up at the beginning of the procedure. ICG fluorescence intensity at the liver was only minimal. It was a grade A cholangiography. Dissection was started at the cystic gallbladder junction. The gallbladder was accidentally perforated during dissection. At the time of perforation, ICG fluorescence intensity over the leaked bile was only minimal. The dissection around Calot’s triangle continued, and the cystic duct showed up clearly after time. It was a long cystic duct with low insertion to the common bile duct. As dissection continued, the ICG fluorescence intensity over the leaked bile increased and became obvious. A critical view of safety was achieved after further dissection. The cystic artery was divided between metal clips. The cystic duct was divided between Hemoclips at the cystic gallbladder junction. The gallbladder was then dissected from the liver with diathermy, and cholecystectomy was effected. The leaked bile was effectively sucked away with the help of ICG fluorescence. At the end of the procedure, bile leakage was checked with ICG fluorescence to ensure there was no bile leakage.
Discussion
High-quality ICG cholangiography can be safely performed with a single-shot intravenous 0.025 mg ICG on induction of general anesthesia. It has been proven to be beneficial in cholecystectomy with reduced conversion rate and operative time, 1 although more studies are required to prove whether it can help reduce the chance of biliary injury.
ICG cholangiography is easy to use and apply. In our study dosage, only a single shot of 0.025 mg ICG and no additional dose were required. Also, the time of injection was convenient. We injected ICG at the time of induction, which was usually at the same time that we administrated prophylactic antibiotics, in contrast to some studies that required injection hours before operation.2,6,8,14 In addition, the cost of ICG is low. In our center, each vial containing 25 mg ICG costs HKD$382.2 (USD$49.1). Our team used a whole vial to dilute 1000 times to 0.025 mg in the operation theatre for each patient due to medication safety. The cost could be further reduced if a single vial was used in multiple patients with pre-dilution done by the pharmacy unit.
ICG fluorescence not only was used to distinguish biliary structure, but it also was used to check any bile leakage and aid suction of leaked bile at the end of procedure.
Anaphylaxis was a theoretical risk for ICG cholangiography. However, the risk is low, and previous studies reported the risk of anaphylaxis was 0.05%, 24 with manifestations as hypotension and arrhythmia.
The intensity of ICG fluorescence varies among different patients. One of the factors that affects the intensity is the thickness of the tissue around the biliary structure. In the case of an emergency operation with an acutely inflamed gallbladder, the tissue thickness would be higher, and therefore, the biliary structure might be more difficulty to show up. In our study, 2 patients underwent cholecystectomies in an emergency setting. Both of the operations revealed grade A cholangiography. Time to identify biliary structure was 25 minutes and 35 minutes, respectively. The time was similar to the average time (33.3 minutes) in our study.
Previous studies used a much higher dose of ICG for ICG cholangiography. Yet, the quality of ICG cholangiography was suboptimal, as a higher dose made biliary structure more difficult to be distinguished from its surrounding. Our study used a much-diluted dose, 0.025 mg, for ICG cholangiography, which made a higher quality ICG cholangiography easily feasible. Therefore, we advocate liberal use of ICG cholangiography in laparoscopic cholecystectomy.
Conclusions
88.9% ICG cholangiography was grade A with a single-shot intravenous 0.025 mg ICG on induction of general anesthesia. High-quality ICG cholangiography can be safely performed with this dosage in cholecystectomy.
Footnotes
Acknowledgments
The authors acknowledge the staff of the operation theatre of Tuen Mun Hospital and Pok Oi Hospital of the Hospital Authority for providing support the use of ICG cholangiography in hepatobiliary surgery.
Authors’ Contributions
All authors contributed equally to this work.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.