
Abstract
Background:
Liver resection remains the cornerstone for curative management in primary liver malignancies. Liver surgery ranges from simple wedge resections to complex hepatectomies involving vascular or biliary reconstructions. The anatomical complexity of the liver and these varied surgical approaches create challenges in assessing operative difficulty. This literature review explores the key factors influencing operative difficulty in liver resection for primary liver malignancy across surgical techniques.
Methods:
A broad literature review was conducted to determine the factors that were associated with increased operative difficulty in liver resection using the Embase, PubMed, and Cochrane databases for studies published between 2000 and 2025.
Results:
This review identifies several patient, tumor, and surgical factors that influence operative difficulty in liver resection. Numerous difficult scoring systems were identified, yet their applicability across different operative approaches remains uncertain. Across open and minimally invasive techniques, tumor size and location are commonly used to determine complexity. However, debate remains regarding the optimal cutoff for tumor diameter. Other identified factors include the extent of resection, patient-specific variables (e.g., cirrhosis, body mass index, previous surgeries), and surgical technique. In addition, liver resection procedures classified based on the 2000 Brisbane terminology have been stratified into three groups of increasing difficulty.
Conclusion:
The ability to predict operative difficulty is useful for case selection, surgical planning, and risk stratification for meaningful shared decision-making. Future research should focus on refining predictive models by integrating composite measures, including patient-reported outcomes and long-term survival. A unified, validated scoring system applicable across surgical techniques could enhance consistency in clinical practice and research to improve outcomes.
Introduction
The treatment of primary liver cancer is nuanced and depends on the subtype or location of the tumor, but surgery remains the mainstay for curative intent. “Liver resection” is a broad term that encompasses heterogenous procedures ranging from simple wedge resections to complex hepatectomies involving vascular or biliary reconstructions. Partly due to the complexity and variability of liver anatomy, there have been inconsistencies in resection nomenclature in the past.
In 1979, Tung described “minor” and “major” liver resections, with “minor” being defined as the resection of two or fewer Couinaud segments and “major” as three or more Couinaud segments. 1 At the meeting of the International Hepato-Pancreato-Biliary Association in Brisbane, Australia, in 2000, there was an attempt to rationalize and standardize the numerous and often confusing nomenclature of hepatic anatomy and resections. 2 This led to the Brisbane 2000 Nomenclature of hepatic anatomy and resection based on the following eight attributes: (1) it is anatomically correct, (2) anatomical and surgical terms are in agreement, (3) consistency, (4) self-explanatory, (5) linguistically correct, (6) precise, (7) concise, and (8) translatable. 2 Although the Brisbane classification has improved communication among hepatic surgeons, its limitations include the use of multiple terms for the same resection and its failure to adequately describe nonanatomical resections, multiple resections, or combined bilio-vascular reconstructions. Since then, further classification systems have been proposed, including the “New World” terminology by Nagino et al. (2021) and the updated Brisbane classification by Wakabayashi et al. (2022). Regardless of the nomenclature or system used, classification of the relative difficulty of a resection is not standardized and remains at the discretion of the surgeon.3,4
There is a spectrum of technical difficulty encompassing the broad range of liver resection operations. The terms “minor” and “major” resections can be misleading as they do not stratify the complexities of the procedure despite having the same name. For example, a left lateral sectionectomy (segments 2 and 3) and a right anterior sectionectomy (segments 5 and 8) would both be classified as a minor resection, although, they vary greatly in complexity. Certainly, within laparoscopic liver resection, there is agreement that complexity varies significantly based on the location. For example, accessing posterior segments is much more challenging laparoscopically than it is during an open approach. 5
The differentiation of surgical complexity or the technical difficulty of an operation is challenging because it is a subjective measure and varies depending on the experience and training of the surgeon. Surrogate markers for technical or operative difficulty have been proposed, including operative time, duration of inflow occlusion, estimated blood loss, number of units of blood transfused, and whether a minimally invasive approach was converted to an open approach. In a range of general surgical procedures, operative time and conversion to open approach have been used as surrogates for operative difficulty.6–9 Furthermore, increased operative time is associated with an increased risk of postoperative complications across open, laparoscopic, and robotic liver resections. 10 Understanding the difficulty of a procedure is beneficial because surgeons can accumulate experience in easier cases during their operative learning curve, and then progress to more challenging cases as they progress. Furthermore, understanding the difficulty of an operation would aid with planning of the approach, which is particularly important for minimally invasive approaches.
There is still much to understand about predicting the difficulty of a liver resection and understanding the factors that impact the intraoperative complexity. Addressing these issues would be useful for justifying a specific operative technique, for improving patient counseling, and to assist with comparative clinical outcome research. This narrative review aims to investigate the factors associated with predicting operative difficulty in liver resection for malignant tumors.
Methods
A thorough literature review of existing literature was completed using the Embase, PubMed, and Cochrane databases to complete this narrative review. The following search terms were applied between December 10, 2025, and December 26, 2024:
(“liver resection” OR hepatectomy) AND operative AND difficulty AND (malignan* OR cancer) (“liver resection” OR hepatectomy) AND (difficult* OR complex*) AND (malignan* OR cancer) “Hepatectomy”[Mesh] AND (difficult* OR complex*) AND (malignan* OR cancer)
Results between 2000 and 2025 were screened. After duplicate results were removed, relevant articles were screened through title and abstract review (Fig. 1). Further relevant articles were reviewed through a full-text review. Inclusion criteria were all study types, including systematic reviews, meta-analyses, randomized control trials, and cohort studies that assessed factors that impacted intraoperative difficulty in liver resection for malignancy. This study included liver resection operations, including open, laparoscopic, and robotic techniques.
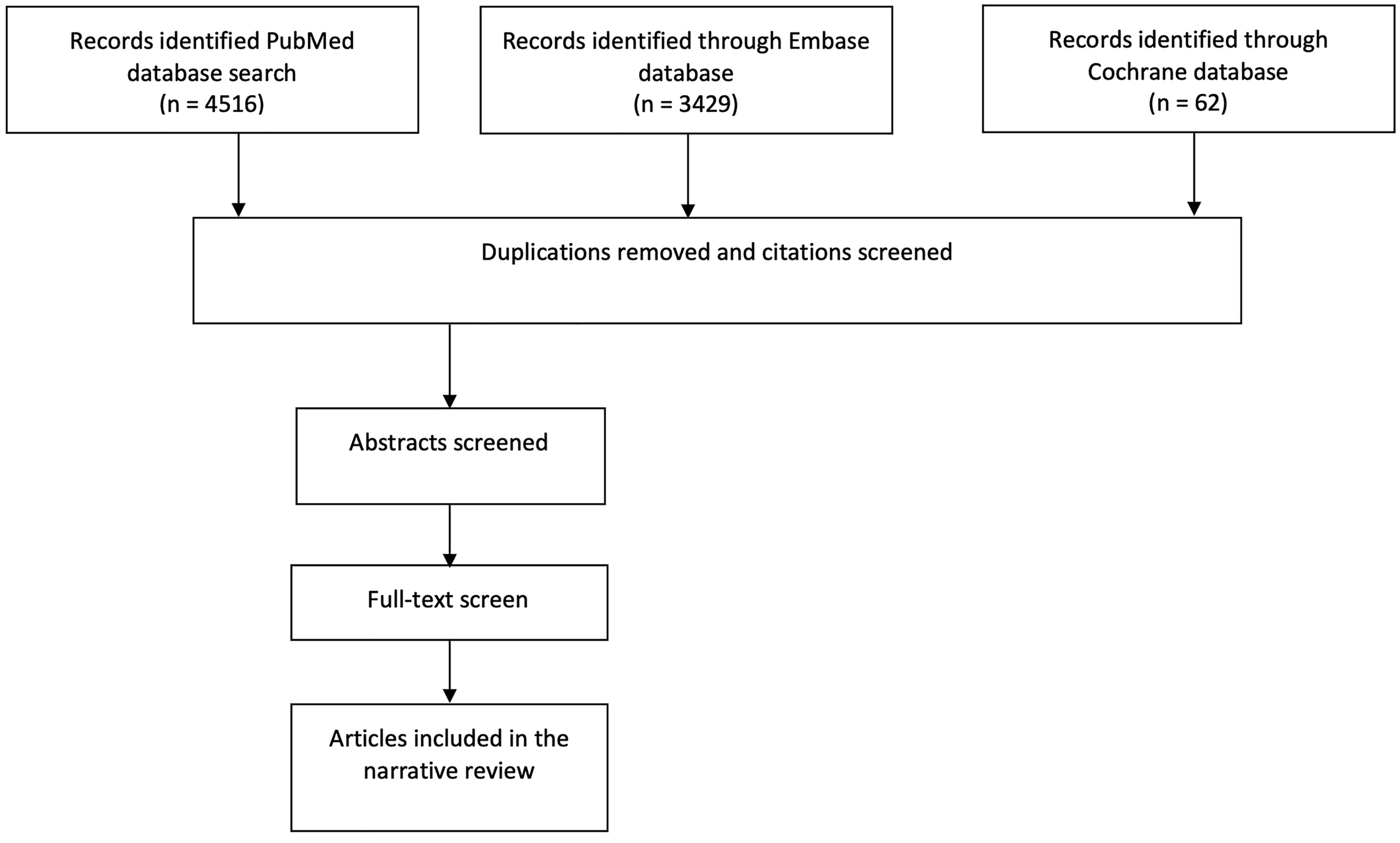
Search strategy.
Results
After evaluating the existing literature, numerous operative difficult scoring systems were identified that were developed based on expert opinion or retrospective review of existing databases. However, these scoring systems were validated across a single operative technique, for example, open, laparoscopic, or robotic. A summary of the various difficulty scoring systems is summarized in Table 1. There have been attempts to rationalize the difficulty of different types of liver resections based on the anatomical location of the resection. A summary of the identified classifications based on the procedure is summarized in Table 2. In addition, patient factors have been assessed to determine which parameters influence intraoperative difficulty.
Comparison of Factors Included in Operative Difficulty Assessment Tools for Liver Resection
Comparison of Classification Tools of Liver Resection Procedures by Difficulty
Open liver resection
The development of a difficult scoring system in open liver resection was completed by Pothet et al. (2021), where operative difficulty was defined based on the operative time, the liver transection time, the estimated blood loss, and the number of vascular inflow (Pringle) maneuvers. 11 Operations were stratified into two categories as follows: “standard liver resection” and “difficult liver resection” through a multicenter prospective cohort study known as the DIFF-sCOR study. 11 To calculate the probability of a difficult liver resection, the tool assess the patient’s body weight, number of tumor nodules, maximum tumor size (>10 cm), type of hepatectomy (anatomical versus nonanatomical), whether transection planes were used in the resection, the site of a nonanatomical resection, whether vena caval reconstruction is required, whether a bilio-enteric anastomosis is required, and whether there will be more than one liver specimen to calculate the probability of a difficult liver resection. Although this scoring system was useful in predicting intraoperative outcomes, its use may be limited by the complexity of the formula to predict difficulty and it was not able to accurately predict postoperative outcomes. 11
Prior to this, Pulitanò et al. in 2007 attempted to identify preoperative factors associated with perioperative blood transfusion in liver surgery. 19 Using a forward-step regression model, they demonstrated that a preoperative hemoglobin of ≤12.5 g/dL, exposure of the vena cava, the presence of cirrhosis, having an associated surgical procedure, and the largest tumor >4 cm were associated with increased incidence of perioperative blood loss. 19 These five clinical variables were then used to develop a transfusion risk score, demonstrating good discrimination in the validation set. 19 The number of blood units transfused has been used as a surrogate marker of operative difficulty, and hence, these factors may be useful in determining the operative difficulty. Furthermore, a retrospective assessment of patient factors that might affect the difficulty of a colorectal metastasis liver resection was undertaken by Inoue et al. (2020), who showed that the overall body mass index (BMI) did not impact operative times or estimated blood loss. 20 However, in relation to the operative technique, a further subgroup analysis of patients with BMI >25 showed that an open resection took 87 minutes longer than a minimally invasive approach, highlighting that there may be a benefit in using a minimally invasive approach in patients with obesity. 20
Laparoscopic liver resection
Various operative difficulty scoring systems have been developed to estimate the difficulty of laparoscopic liver resections.
Ban et al. (2015) proposed a 10-level index that reflected the variable difficulty of laparoscopic liver resection after completing a three-center retrospective study examining 90 cases. 12 The study used subjective assessment by the surgeon in relation to the degree of difficulty, and determined that the culmination of five factors, including tumor location, the extent of liver resection, tumor size (<3 cm or ≥3 cm), proximity to major vessels, and the Child–Pugh status, aligned with the difficulty assessment completed by the surgeon. 12 Furthermore, when the 10-index score was converted into a three-level assessment (low, intermediate, and high) system, the scoring system also showed 95% agreement. 12 Subsequently, this become known as the IWATE difficulty scoring system and has since been validated by other studies.21–25 Expanding on this work, a successive novel difficulty scoring system was proposed by Xi et al. (2022) that used a 14-point scoring system. 13 It differs from the original scoring system by including additional factors such as the caudate lobe as a location of the tumor, a diagnosis of either a benign or malignant condition, and whether there was a history of hepatobiliary surgery.
The Hasegawa scoring system (2017) proposed for Japanese patients was developed through a retrospective review of a prospectively collected database. These authors examined a range of preoperative factors, determining that obesity, low platelet count, and the extent of resection were correlated with increased operative time. 14 However, this scoring system excluded patients with resection involving segment 1, tumors ≥10 cm, patients with ≥4 lesions, patients with visceral metastatic disease, or those who underwent concomitant vascular or bile duct reconstructions. In contrast to the IWATE score, this study found that proximity to a major vessel was not associated with increased operative time; however, this may be due to the exclusion of certain patients as described above. 14 From the initial multivariate analysis, they proposed a three-level difficulty tier with the extent of resection, the location of the tumor, the presence of obesity (BMI > 30), and the preoperative platelet count (≤100 × 109/L) showing statistically significant differences between the three tiers in terms of surgical time, blood loss, and length of stay in the hospital.
Furthermore, the Institut Mutualiste Montsouris (IMM) score was developed by Kawaguchi et al. (2018) in French patients who underwent laparoscopic liver resection. 18 This was completed through a retrospective review of prospectively collected patient data, stratifying procedures based on the Brisbane classification across three levels based on operative time < or ≥190 minutes), blood loss (< or ≥100 mL), duration of the Pringle maneuver, and rates of conversion to an open operation (< or ≥4.2%). 18 Similar to the other groups, the study cohort excluded patients who underwent biliary or vascular reconstruction, multiple liver resections (>4), repeat laparoscopic liver resection, and concomitant extrahepatic procedures (except cholecystectomy). 18 These authors classified wedge resection of the anterolateral segment, wedge resection of the posterolateral segment, or left lateral resection as group I; anterolateral segmentectomy and left hepatectomy as group II; and posterosuperior segmentectomy, right hepatectomy, extended right hepatectomy, right posterior hepatectomy, central hepatectomy (segments 5 and 8 or segments 4, 5, and 8), and extended left hepatectomy as group III.
The Southampton difficulty scoring system, developed by Halls et al. (2018), used operative time as an objective marker of operative difficulty. 15 Following a survey of 80 surgeons through the European African Hepato-Pancreato-Biliary Association, as well as a literature review, they identified variables that increased operative difficulty. Through a retrospective review, they determined that a previous open liver resection, a diagnosis of benign or malignant condition, the tumor size (<3 cm, 3–5 cm, >5 cm), and the classification of the resection (minor, technically major or anatomically major) would be included in their scoring system. With a higher score, this group demonstrated an increased likelihood of intraoperative complications, as well as predicting 90-day mortality. 15 Subsequently, an external validation of the Southampton score was shown to be a good effective predictor of intraoperative outcomes and postoperative outcomes.23,26
Additional difficulty scoring systems have been proposed for repeat laparoscopic liver resection. Okamuru et al. (2019) proposed a system derived from the IWATE score for repeat laparoscopic liver resection by adding a parameter to include whether the tumor was on the cranial or dorsal side of the previous surgical site. 27 However, only limited conclusions can be drawn from this study, as it was based on only 40 patients, with inclusion criteria restricted to patients who underwent partial hepatectomy or left lateral sectionectomy without thoracotomy, consequently limiting generalizability. 27 Furthermore, in patients with recurrent hepatocellular carcinoma, Kinoshita et al. (2019) demonstrated that two or more previous liver resections and procedures more radical than a sectionectomy were associated with increased operative times, while the operative approach in the previous resection (open or laparoscopic), a history of cholecystectomy at the time of the previous resection or a history of nonsurgical treatment before the operation, was not associated with operative difficulty. 28 These studies highlight the need for further research to assess which variables most effectively determine operative difficulty in repeat laparoscopic liver resection.
There have been attempts to rationalize the optimal cutoffs for tumor size to stratify the operative difficulty in laparoscopic liver resection. Ivanecz et al. (2021) proposed using 3.8 cm as the cutoff size for tumor diameter after a retrospective review to assess how the IWATE score affects intraoperative and postoperative complications.12,29 Furthermore, Kabir et al. (2022) found that a larger tumor size in laparoscopic liver resections was associated with increased operative time as well as prolonged postoperative hospital stay. 30 They suggested using a trichotomy of <3 cm, 3–6.9 cm, ≥7 cm as tumor size cutoffs and that this would be a better predictor than using the dichotomy in the IWATE scoring system. However, this study excluded patients who underwent concomitant operations. 30 Furthermore, Aizza et al. (2022) argued that in relation to laparoscopic lateral sectionectomy, cutoffs should be 0–3.9 cm, 4–6.9 cm, 7–9.9 cm, and ≥10 cm as they determined that these sizes consistently discriminated between open conversion rates, operative time, estimated blood loss, transfusion rates, and Pringle maneuver use, as well as correlating with major postoperative complication rates. 31 A subsequent retrospective review by Kato et al. (2023), involving 1396 patients who underwent laparoscopic major hepatectomies, showed that tumor cutoffs of 5 and 10 cm impacted the rates of conversion to open surgery, operative times, estimated blood loss, application of the Pringle maneuver, and requirement for an intraoperative blood transfusion. 32 However, these factors did not affect major postoperative complications or length of stay in the hospital. 32 Therefore, although a tumor diameter of 3 cm was used as the cutoff in the IWATE score, given the heterogeneity in liver resection, a single or unifying tumor cutoff size may not be appropriate as further studies have suggested that this may not be the optimal diameter to effectively stratify operative difficulty.
Patient and radiological factors
In addition to the abovementioned difficulty scoring systems in laparoscopic resection, other studies have assessed patient and radiological factors that might impact operative difficulty. A multicenter retrospective review of 1034 patients undergoing minimally invasive liver resection for colorectal metastasis by Ghotbi et al. (2023) showed that neoadjuvant chemotherapy did not impact open conversion rates, mean operating time, or intraoperative transfusion rates. 33 Indirectly, this suggests that these factors have no impact on the difficulty of the operation, despite being used in the Southampton difficulty scoring system. 34 Montalti et al.’s (2023) multicenter retrospective review of patients undergoing minimally invasive (laparoscopic or robotic) major liver resection showed that males, previous abdominal surgery, ASA score ≥ 3, median tumor size, IMM score class III, and portal hypertension were independently associated with an increased risk of conversion to open surgery. 33 Interestingly, the leading cause of conversion to open surgery in this study was bleeding. 33
Although liver cirrhosis and tumor size have previously been shown to increase the difficulty of the operation due to distorting anatomy, it was suggested that ASA ≥ 3 was associated with high conversion rates because of a lower threshold for conversion in the presence of comorbidities. Also, it was suggested that male patients had an increased risk of converting to open surgery because of higher BMIs, larger liver size, and a higher incidence of cirrhosis compared with female patients, as opposed to other technical challenges of the procedure.33,35 The findings of liver cirrhosis increasing operative difficulty have been replicated in patients with Child–Pugh A liver cirrhosis undergoing minimally invasive liver resection of the anterolateral segments, laparoscopic left sectionectomy, and major laparoscopic liver resection, with studies also showing an increase in postoperative hospital stay and morbidity.36–38 Interestingly, subgroup analysis comparing patients with Child–Pugh A and B showed no difference in intraoperative outcomes, and additionally, there was no difference in intraoperative outcomes in a subgroup analysis of cirrhotic patients with or without portal hypertension.37,38 This highlights the relative increase in difficulty of laparoscopic liver resection for patients with cirrhosis due to stiffened parenchyma and the loss of tactile feedback, along with a lowered threshold for accepting bleeding in these patients.
Furthermore, Chen et al. (2023) showed that increasing BMI is associated with longer operative times, increased blood loss, higher blood transfusion rates, greater use of the Pringle maneuver, and higher conversion to open rates in laparoscopic left lateral sectionectomy. 39 In addition, Guilbaud et al. (2020) estimated the technical difficulty of the resection by estimating the total transection surface area using preoperative triple-phase liver protocol CT with 3D reconstruction. 40 They identified that the transacted area would increase with increasing IMM grade, and that is not an unexpected finding as IMM grades are based on the type of resection. This study demonstrated that an estimated parenchyma transection surface area ≥100 cm2 was associated with increased operative time, higher blood loss, and increased conversion to open surgery rates, as well as worse postoperative outcomes, including higher overall morbidity, higher biliary leakage rates, increased rates of fluid collections, and increased rates of pulmonary complications when compared with an estimated parenchyma transection surface area of <100 cm2. 40 Therefore, in laparoscopic liver resection, it is suggested that previous abdominal surgery, increasing BMI, cirrhosis, and estimated transection surface area are important factors associated with increasing technical difficulty of the operation.
Robotic surgery
While the widespread uptake of robotic approaches has been limited worldwide due to a lack of a dedicated robotic parenchymal transection tool, the development of a difficulty scoring system in robotic liver surgery is still of interest. The Tampa difficulty scoring system was developed by Sucandy et al. (2024) to predict the difficulty of robotic liver resection using the following parameters: whether neoadjuvant chemotherapy was used, the tumor location (segments 7 and 8 scoring the highest), the tumor size (<3 cm or ≥3 cm), the extent of the parenchymal resection, the need for a portal lymphadenectomy, and the need for extrahepatic biliary reconstruction. 16 Operative time and estimated blood loss were used as a surrogate marker for operative difficulty in this study. 16 Subsequently, an internal validation of the Tampa difficulty scoring system was conducted through a prospective cohort study showing that operative difficulty progressively increased with increasing grades. However, interestingly, there was increased estimated blood loss in the advanced group compared with the expert group. In addition, there was a progressive increase in the length of hospital stay with increasing difficulty. Although there was no analysis of whether this was associated with long-term overall survival. 41 In summary, similar variables used in laparoscopic procedures impact operative difficulty in robotic liver resection. Further studies are needed for external validation of the Tampa difficulty scoring system.
Anatomical classifications
The difficulty of liver resection has been assessed based on the anatomical location of the tumor and the resection site.
Through a survey study of international liver surgeons, Lee et al. (2015) classified open liver resections into three categories of complexity based on those expert opinions, placing operations into low-complexity (peripheral wedge resection and left lateral sectionectomy), medium-complexity (left hepatectomy without caudate resection, right hepatectomy, right posterior sectionectomy, left hepatectomy with caudate resection, and right trisectionectomy), and high-complexity categories (right anterior sectionectomy, middle hepatectomy, left trisectionectomy without caudate resection, and left trisectionectomy with caudate resection). 42 Subsequently, retrospective reviews of patients undergoing open liver resection for hepatocellular carcinoma showed that this classification system was effective in differentiating operative times, blood transfusion rates, and estimated blood loss from the low- to the high-complexity groups as well as in predicting postoperative outcome, including morbidity and major complication rates.43,44 Furthermore, the system outperformed the traditional minor/major classification.43,44 Lee et al. (2016) then conducted a further survey of experts and amended right hepatectomy to account for whether it was performed with or without caudate resection as well as taking into consideration vascular or biliary reconstructions. 17 As a result, the medium-difficulty procedures included a right hepatectomy without caudate resection and isolated caudate resection, and the high-complexity group included right hepatectomy with caudate resection, right hepatectomy with hepaticojejunostomy, anatomical middle hepatectomy, and right hepatectomy with portal vein reconstruction or inferior vena cava reconstruction. 17
Kawaguchi et al. (2020) completed a retrospective review of patients across two sites to determine whether the IMM score initially designed for laparoscopic liver resection would be applicable to open liver resection. 45 They demonstrated that operative time, estimated blood loss, and complication rates increased in a stepwise manner from grade I to III, indicating that this system could potentially also be used in open procedures. 45 Therefore, open resection of the posterosuperior segment (Couinaud segments 1, 4a, 7, and 8) was associated with worse surgical and postoperative outcomes compared with anterolateral segments (Couinaud segments 2, 3, 4b, 5, and 6).45,46 Interestingly, this trend has already been observed in laparoscopic liver resection.45,46
A multicenter retrospective review by Efanov et al. (2022) comparing the difficulty of laparoscopic limited liver resection in segment 7 compared with segment 8 showed that segmentectomies in segment 7 had longer operative times and subsequent lengths of stay compared with segment 8. 47 This contrasted with their findings that atypical resections in segment 7 had greater estimated blood loss, higher transfusion rates, longer operative times, and higher conversion rates compared with atypical resections of segment 8. 47 These findings are attributed to segment 7 being in a more anatomically difficult location to access because of its posterior location, where the ribs extending caudally restrict access in this region. However, these findings are significant given that the IWATE difficulty scoring system, the IMM scoring system, the Southampton difficulty scoring system, and the Hasegawa scoring system did not differentiate between segments 7 and 8 in terms of point rating or difficulty grade.
Furthermore, a retrospective review of prospectively collected data by Azoulay et al. (2022) to determine if open liver resection in the “central column” of the liver, defined accurately in their article, was associated with increased operative difficulty for colorectal metastasis. 48 They showed that resection of this area was associated with longer operative time and a higher number of units of blood transfused, suggesting increased operative difficulty. However, they also demonstrated that liver resection in the central column was associated with higher rates of severe postoperative complications. 48 These findings contrast with a prior meta-analysis comparing central liver resection and extended hepatectomy for malignant resections by Chan et al. (2018), which showed that central liver resections had fewer overall postoperative complications than extended hepatectomy, with similar mortality rates. However, this meta-analysis considered a wide range of surgical approaches, and its definition of central liver resection differed slightly from that used by Azoulay et al. (2022).48,49
Discussion
The results of this review show several patient, tumor, and surgical factors that are associated with increased operative difficulty in liver resection. Across open and minimally invasive techniques, tumor size and location are commonly used to determine the difficulty of the operation; however, there is still debate regarding the optimal cutoff for tumor diameter. Patient factors that impact operative difficulty include body habitus (BMI or weight), anemia, cirrhosis, thrombocytopenia, and whether there were previous abdominal operations. Of these, the only preoperative modifiable factors are body habitus and anemia status that could potentially help to decrease the technical difficulty of a procedure. Increasing BMI has been shown to increase the risk of steatohepatitis and cirrhosis due to the association with metabolic-associated fatty liver disease.50,51 This would not only increase the difficulty of the operation due to ensuring appropriate exposure of the patient but also due to concerns from steatosis or liver cirrhosis. Liver cirrhosis was shown to increase the difficulty of both open and minimally invasive techniques, which can be attributed to the fibrosed parenchyma, the frequent presence of portal hypertension, and coagulation deficits, distortion of the liver anatomy, and difficult intraoperative ultrasound visualization for assessment of tumor margins and localizations.5,35–38 Furthermore, steatohepatitis, which can be considered a precursor to liver cirrhosis, was shown to be one of the most common liver abnormalities in patients undergoing liver resection. 51 Patients with higher BMI have shown a greater degree of fibrosis likely secondary to increasing rates of steatosis, but steatosis has independently been shown to increase the blood loss in patients undergoing resection, suggesting steatosis could be a risk factor for increasing operative difficulty.52,53 Ultimately, understanding these factors contributing to the technical difficulty of procedures will assist the surgeon with preoperative planning in relation to the expected operation length, use of experienced operating room staff, and identifying patients who may require senior and more experienced assistance. Further research is needed to identify modifiable patient factors that can improve intraoperative and postoperative events.
Operative difficulty scoring systems in liver surgery are helpful, and are more accurate than the surgeons’ subjective expectation regarding postoperative outcomes, which generally have low sensitivity, specificity, accuracy, and performance, even when controlled for surgical experience, highlighting the need for an objective measure. 54 The scoring systems are superior because they use objective measures. The variables included in the multiple operative difficulty scoring systems identified in this review are summarized in Table 1, showing significant overlap, despite different operative approaches. The most common factors were the extent of the liver resection, the tumor location, and the tumor diameter. Table 2 highlights the anatomical classification of the liver resection based on the three-tiered difficulty systems in the IMM classification and by Lee et al. (2016). There are similarities in the classification for both laparoscopic and open procedures within these systems, highlighting that the relative difficulties of each procedure can translate across operative techniques. Although numerous operative difficulty scoring systems have been proposed to date, inconsistencies remain between them, possibly explaining why no single system has been universally adopted. Further work is required to determine the most effective system and for which surgical approach it is best suited.
Currently, the IWATE scoring system has been evaluated in open and robotic procedures, despite initially being developed for laparoscopic procedures only. For robotic liver resection, Chong et al. (2019) applied the IWATE scoring system in a prospective cohort study demonstrating a good correlation across the different grades for operative time, blood loss, morbidity rate, and postoperative hospital stay. 21 Furthermore, Luberice et al. (2020) highlighted increased operative time with increasing scores in robotic liver resection; however, interestingly, there was no statistically significant difference found between expert and advanced difficulty levels in terms of postoperative outcomes, compared with laparoscopic liver resection. 55 This suggests the most benefit with robotic surgery is in difficult procedures, where the utility of stereopsis and increased articulation in tight anatomical areas assist with challenging dissection with a trade-off in simpler cases where the benefit may be marginal or nonexistent. However, these advanced techniques place a larger economic burden, which can strain health care resources due to increased upfront costs for equipment, requirement for specialized teams in robotic surgery, and training in robotic surgery. While robotic surgery may offer benefits for a small subset of very advanced or difficult cases, the larger proportion of patients may receive minimal benefit, raising concerns about the cost-effectiveness. This highlights the need for future research to include economic evaluations through cost–benefit studies to fully assess the impact on resource allocation and sustainability of the procedure. Subsequent retrospective cohort studies have shown similar results with increasing IWATE difficulty scores correlating with increased operative time, estimated intraoperative blood loss, postoperative hospital stay, increased overall 90-day mortality, and liver failure rates, highlighting that the adoption of the IWATE score in robotic liver resection could be appropriate.56–58 The IWATE difficulty scoring system was used to stratify patients into uncomplicated and complex liver surgery by Xie et al. (2022) to identify differences between perioperative outcomes in liver resection between open, laparoscopic, and robotic techniques. 59 They demonstrated that in more straightforward liver resection, robotic and laparoscopic liver resection took longer to complete than in open, with no difference in postoperative complications, however, in technically challenging liver resection, open and laparoscopic techniques were quicker than robotic liver resection, but the robotic technique was associated with fewer postoperative compilations and shorter length of stay in hospital. Given the findings of these studies and the degree of overlap of factors in the operative difficulty systems, it highlights the potential utility of using the IWATE scoring system in robotic or open surgery, where a unified scoring system across operative techniques would increase ease of use among clinicians and assist with standardizing research when comparing operative techniques.
The laparoscopic difficulty scoring systems have been compared through several studies. Goh et al. (2021) completed a retrospective review to compare these scoring systems in terms of intraoperative and postoperative outcomes, assessing the IWATE, IMM, Southampton, and Hasegawa difficulty scoring systems. There was no difference in the calibration of the four systems in terms of blood loss and postoperative stay, however, the Southampton scoring system performed worse in predicting operative time compared with the other three systems in this study. All four scoring systems showed poor discrimination with respect to blood transfusion rates, conversion to open rate, and postoperative morbidity. 23 Similar comparison for patients with hepatocellular carcinoma undergoing laparoscopic liver resection by Linn et al. (2022) showed that all four difficulty scoring systems performed well in predicting operative time, estimating blood loss, postoperative complications, but the IWATE score was the only one able to predict conversion to open rates in their cohort. 60 Furthermore, Ruzzenente et al. (2022) conducted a machine learning analysis of these four scoring systems through a retrospective review of patients undergoing laparoscopic liver resection for both benign and malignant liver lesions, showing that all difficulty scoring systems had good discrimination for operative times and estimated blood loss. 58 The utility of the difficulty scoring systems in laparoscopic liver resection has also been assessed in patients undergoing nonmalignant resections, where Yang et al. (2019) showed that in the intergroup analysis both the IWATE and IMM difficulty scoring systems were able to accurately classify the degree of difficulty with respect to operative time, estimated blood loss, and conversion to open rates. 56
Moreover, increasing operative difficulty has been shown to impact postoperative patient outcomes. It has been established that increasing difficulty can lead to higher short-term morbidity, with studies revealing higher IMM classifications and increasing IWATE scores being associated with higher complication rates.18,44 Although surgical risk calculators such as the National Surgical Quality Improvement Program can predict the risk of postoperative complications based on patients’ clinical factors and can be used for liver resection, studies have suggested that it underestimates the risk in complex procedures, particularly liver resection.61,62 In addition, there are conflicting data regarding oncological outcomes, with Holowoko et al. (2020) showing that increasing IMM grades have worsened overall survival despite similar positive resection rates in laparoscopic liver resection for colorectal metastases, and Hobeika et al. (2021) demonstrated worsening textbook outcome rates with increasing difficulty in repeat laparoscopic liver resection for liver metastases.63,64 Interestingly, from a long-term perspective, increasing IWATE scores were inversely associated with a 5-year survival and the 5-year disease-free survival in hepatocellular carcinoma. 65 There is a dearth in the literature assessing the impact of operative difficulty on patient-reported outcome measures and quality-of-life measures, including complications such as prolonged recovery, chronic pain, and reduced functional capacity. Further research in this area would help to rationalize whether technically challenging procedures, although feasible, provide any meaningful benefit to the patient and could provide a better understanding of the trade-offs associated with complex resections. Here, a better understanding of the trade-offs associated with complex resections could enhance shared decision-making, allowing for more informed discussions between surgeons and patients regarding the risks and benefits of these procedures.
The operative difficulty scoring systems identified in this review used operative time as a marker for operative difficulty, which can vary significantly based on surgical experience. In the original studies, it was noted that the procedures were not controlled for operative experience.11,13–15 However, in the Southampton score, the authors stated that using numerous surgeons across multiple sites meant that the study incorporated surgeons at various points along the surgical learning curve. 15 Lee et al. (2016) found that in their initial study, surgeons with less experience were more likely to rate the same procedure as harder than experienced surgeons, and in their second study, more experienced surgeons had a lower overall total difficulty rating compared with less experienced surgeons. 17 This highlights that difficulty levels are inversely correlated with surgical skill and that the assessment of surgical difficulty should require a multivariate approach. In previous literature, there has been an over-reliance on using operative time as a surrogate marker for technical difficulty, but this does not always reflect technical challenges, especially in centers with skilled surgeons, advanced robotic systems, or where cases might be slowed by surgical trainees. Hence, to counteract the limitations of using operative time as a universal metric for operative difficulty, composite measures such as textbook oncological outcomes to assess surgical performance would be of utility and are of interest as they assess outcomes that are more clinically important. Textbook oncological outcomes are defined across seven variables as the absence of intraoperative incidents ≥ 2 as defined by the Oslo grade, grade ≥ B postoperative bile leak, grade ≥ B postoperative liver failure, postoperative complication ≥ 3a according to the Clavien–Dindo classification, readmission within 90 days of surgery with Clavien–Dindo ≥ 3 complications, 90-day or in-hospital mortality, and R1/R2 margin, and have been shown to be associated with improved long-term outcomes. 66 When comparing the various laparoscopic difficulty scoring systems, studies revealed that higher difficulty was associated with increased failure of textbook outcomes, with the Southampton score being the most accurate in predicting textbook outcome. 67 Although the Southampton score does not include obesity in its difficulty scoring system, obesity has been associated with poorer rates of achieving textbook outcomes. 67 Interestingly, of the identified difficulty scoring systems, the type of malignant disease was not an included variable for operative difficulty; however, it is known that the diagnosis impacts postoperative outcomes in liver resection, and this would need to be taken into consideration when using composite measures as an overall endpoint. Hence, the use of composite measures may be a better-suited method to assess the overall success of the operation considering both intra- and postoperative outcomes, providing better insight for shared decision-making. Further studies should assess if the difficulty of the operation is associated with achieving textbook outcomes and the performance of the various difficulty scoring systems in predicting textbook outcomes and long-term outcomes.
Conclusion
Numerous difficulty scoring systems exist for open, laparoscopic, and robotic procedures to predict intraoperative difficulty based on patient, tumor, and surgical factors. However, there are very few modifiable predictors of intraoperative difficulty in liver resection procedures. Current operative difficulty scoring systems provide essential tools for technical planning, and their predictive value for long-term outcomes is burgeoning. Integrating futility metrics, such as tumor biology and systemic health, could enhance decision-making by identifying patients who are unlikely to benefit from surgery. Future research should focus on developing and validating composite models that balance technical feasibility with meaningful clinical outcomes.
Footnotes
Authors’ Contributions
M.P.: Methodology (equal), writing—original draft (lead), conceptualization (supporting), investigation (equal), and writing—review and editing (supporting). A.R.G.: Methodology (supporting), visualization (equal), writing—review and editing (equal), validation (equal), and supervision (supporting). T.J.H.: Methodology (equal), writing—original draft (supporting), conceptualization (lead), investigation (equal), writing—review and editing (lead), and supervision (lead). This article has been approved by all authors and has not been submitted for publication elsewhere.
Disclosure Statement
No conflicts of interest to declare.
Funding Information
No funding has been sought for the production of this article.