
Abstract
Introduction:
Gallbladder cancer (GBC) is the sixth most common gastrointestinal malignancy and the most prevalent cancer of the biliary tract. Although recent studies suggest that extended resection may be the optimal approach for managing T1b GBC, there is no clear consensus on whether simple cholecystectomy (SC) or radical cholecystectomy (RC) offers better outcomes. Therefore, we conducted this systematic review and meta-analysis to compare these two surgical techniques in the treatment of T1b GBC.
Methods:
We systematically searched PubMed, Embase, and the Cochrane Library through June 20, 2024. We pooled odds ratios (ORs) with 95% confidence intervals (CIs) for binary outcomes and assessed heterogeneity using the I2 statistic.
Results:
We included 10 studies comprising 2,964 patients, of whom 51.5% underwent SC and 48.5% underwent RC. RC was associated with significantly higher 2 year (OR: 0.46; 95% CI: 0.28–0.77; P < .01; I2 = 51%) and five-year overall survival rates (OR: 0.79; 95% CI: 0.64–0.98; P = .03; I2 = 0%), and higher 5-year disease-specific survival (OR: 0.59; 95% CI: 0.35–0.99; P = .04; I2 = 0%) compared with SC. However, we found no significant differences in 10-year overall survival (OR: 0.71; 95% CI: 0.45–1.13; P = .15; I2 = 43%) or recurrence rates (OR 1.44; 95% CI: 0.72–2.88; P = .30; I2 = 0%).
Conclusion:
RC provides a short- to medium-term survival advantage over SC in patients with T1b gallbladder cancer, but this benefit appears to diminish over time.
Introduction
Gallbladder cancer (GBC) represents a significant health concern as the sixth most common gastrointestinal malignancy and the most prevalent cancer of the biliary tract. Adenocarcinoma accounts for approximately 98% of all gallbladder tumors. 1 Pathological stage T1b indicates invasion into the muscularis layer of the gallbladder wall. 2 Clinicians often discover T1b GBC incidentally following cholecystectomy, and re-resection is generally considered the optimal treatment. 3 However, the best surgical approach remains a subject of ongoing debate.
Both simple cholecystectomy (SC) and radical cholecystectomy (RC) are considered viable options for treating T1b GBC. Surgeons often favor the more extensive RC approach due to the risk of lymph node metastasis, which occurs in approximately 10% of cases. 3 By including lymphadenectomy, RC addresses potential nodal involvement and provides a more comprehensive treatment strategy aimed at improving long-term outcomes. 4
The decision-making process for surgical intervention in T1b GBC remains challenging due to the lack of randomized controlled trials, leading to variability in clinical practice. 5 As a result, determining the optimal surgical approach, whether simple or RC, continues to generate significant clinical interest. Therefore, we conducted this systematic review and meta-analysis to compare the efficacy and safety outcomes of SC and RC in the treatment of pathological stage T1b GBC.
Methods
Protocol and registration
We conducted this systematic review and meta-analysis following the Cochrane Handbook for Systematic Reviews of Interventions and structured the report according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, as detailed in Supplementary Table S1.6,7 We registered the study protocol in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420246000078. 8
Outcomes
The outcomes of interest were (1) overall survival, (2) disease-specific survival, and (3) loco-regional or systemic recurrence.
Eligibility criteria
We included studies that met the following eligibility criteria: (1) direct comparison between simple and RC for the treatment of T1b GBC, and (2) reporting at least one outcome of interest. We excluded case reports, trial registrations without available results, meta-analyses, reviews, and animal studies. In cases of overlapping populations, we selected the study with the larger sample size for analysis.
Search strategy and study selection
We systematically searched PubMed, Embase, and the Cochrane Library from inception to May 25, 2024. The search strategy included the following terms: (“Gallbladder Adenocarcinoma” OR “Gallbladder Cancer” OR “Gallbladder Carcinoma” OR “Cholecystic Adenocarcinoma” OR “Cholecystic Cancer” OR “T1 Gallbladder Carcinoma” OR “T1b”) AND (“Simple Cholecystectomy” OR “Conventional Cholecystectomy” OR “Standard Cholecystectomy” OR “SC” OR “Standard Resection”) AND (“Radical Cholecystectomy” OR “Radical Resection” OR “Extended Cholecystectomy” OR “EC” OR “RC”) NOT (“Systematic Review” OR “Meta-Analysis” OR “Case Report” OR “Animal Experiment” OR “Animal Study” OR “Review Article” OR “Editorial” OR “Letter to the Editor” OR “Conference Abstract”). We also manually searched the reference lists of the included studies and prior systematic reviews to identify additional eligible articles. 9
Two authors (L.M.D. and C.M.M.) independently performed the search, imported the results into Rayyan Software (Qatar Computing Research Institute, Qatar Foundation), and screened titles and abstracts. After removing duplicates and excluding unrelated records, they assessed the full-text articles for eligibility. A third author (B.F.P.) resolved any disagreements.
Data extraction
Two authors (G.H.A.M. and L.M.D.) independently extracted data into a standardized form, including study characteristics (title, authors, year of publication, publication format, study period, and country), number of participants, patient characteristics (age, sex, tumor histological grade), follow-up duration, and reported outcomes.
Risk of bias assessment
Two authors (C.M.M. and L.M.D.) independently assessed the risk of bias for each included study using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool. 10 They resolved any disagreements by consensus. We did not assess publication bias because the available methods lack sufficient power to detect funnel plot asymmetry when fewer than 10 studies are included. 11
Statistical analysis
Odds ratios (ORs) with 95% confidence intervals (CIs) were pooled for binary outcomes. We calculated the pooled proportions of the outcomes for each group using the inverse variance and logit transformation methods. We deemed a P value of <0.05 statistically significant for overall effect estimates. DerSimonian and Laird random-effects models were used for all outcomes. 12 Heterogeneity was assessed using the Cochran Q test and I2 statistics; P values <0.10 and I2 > 25% indicated significant heterogeneity. For outcomes with significant heterogeneity, we performed a leave-one-out sensitivity analysis to identify influential studies and their effect on the pooled estimates. Statistical analyses were performed using R statistical software, version 4.3.3 (R Foundation for Statistical Computing).
Results
Study selection and characteristics
As detailed in Figure 1, we identified 235 records through the initial search. After removing duplicates and screening titles and abstracts based on prespecified criteria, 23 studies remained for full-text review. Of these, we selected ten observational studies.13–22 The cohort included 2,964 patients, with 1,528 (51.5%) undergoing SC and 1,436 (48.5%) undergoing RC. Overall, 37% of the patients were male. The studies collected data between 1982 and 2018. Studies conducted in East Asia accounted for 52% of the patient population, while 48% were from the United States. Six studies reported the mean follow-up duration, with the shortest reported follow-up being 45 months. Table 1 presents the baseline characteristics of the included studies.

Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram of study screening and selection.
Baseline Characteristics of the Studies Included in the Meta-Analysis
*Median.
**Mean (no SD given).
aData from T1a, T1b, and T2 cohort.
NA, not available; PSM, propensity score matching; RC, radical cholecystectomy; RCT, randomized controlled trial; R-obs, retrospective observational study; SC, simple cholecystectomy.
Pooled analyses
2-Year overall survival
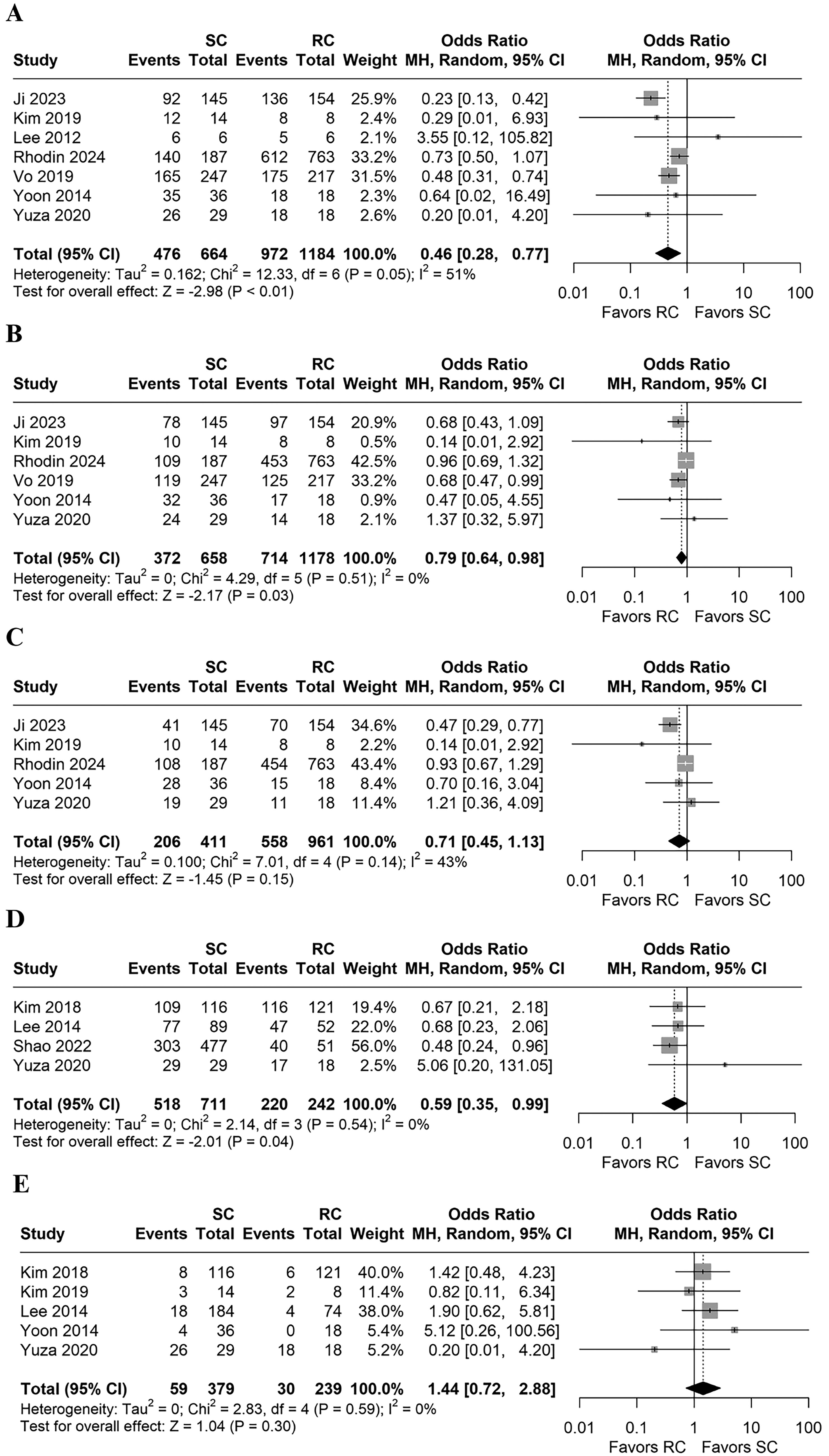
The pooled 2-year overall survival rate was 75.61% (95% CI 66.63%–82.80%) in the SC group and 83.61% (95% CI 78.63%–87.61%) in the RC group. The 2-year overall survival was significantly higher in the RC group (n = 1,848; OR: 0.46; 95% CI: 0.28–0.77; P < .01; I2 = 51%; Fig. 2A).15,16,18,20–23
RC was associated with higher
5-Year overall survival
The pooled 5-year overall survival rate was 62.48% (95% CI: 55.84%–68.69%) in the SC group and 64.20% (95% CI: 53.38%–73.74%) in the RC group. The 5-year overall survival was also significantly higher in the RC group (n = 1,836; RR .79; 95% CI: 0.64–0.98; P = .03; I2 = 0%; Fig. 2B).15,18,20–23
10-Year overall survival
The pooled 10-year overall survival rate was 59.22% (95% CI: 39.39%–76.45%) in the SC group and 60.46% (95% CI: 47.88%–71.79%) in the RC group. The difference in 10-year overall survival between groups was not statistically significant (n = 1,372; OR: 0.71; 95% CI: 0.45–1.13; P = .15; I2 = 43%; Fig. 2C).15,18,21–23
5-Year Disease-Specific survival
The pooled 5-year disease-specific survival rate was 87.98% (95% CI: 66.43%–96.44%) in the SC group and 90.72% (95% CI: 78.81%–96.26%) in the RC group. Although slightly higher in the RC group, the difference was not significant (n = 953; OR: 0.59; 95% CI: 0.35–0.99; P = .04; I2 = 0%; Fig. 2D).14,17,19,22
Loco-regional or systemic recurrence
The pooled loco-regional or systemic recurrence rate was 21.94% (95% CI 6.74%–52.24%) in the SC group and 15.84% (95% CI 3.66%–48.25%) in the RC group. Recurrence rates did not differ significantly between groups (n = 618; OR: 1.44; 95% CI: 0.72–2.88; P = .30; I2 = 0%; Fig. 2E).14,15,17,21,22
Sensitivity analysis
Sensitivity analysis for 2-year overall survival identified the study by Ji et al. 23 as the main source of heterogeneity. Removing this study eliminated between-study heterogeneity without significantly changing the effect estimate (OR: 0.61; 95% CI: 0.46–0.81; I2 = 0%; Supplementary Fig. S1). For 10-year overall survival, sensitivity analysis indicated that both the studies by Rhodin et al. 18 and Ji et al. 23 contributed to heterogeneity. Excluding Ji et al. 23 did not significantly affect the effect estimate (OR: 0.92; 95% CI: 0.68–1.24; I2 = 0%; Supplementary Fig. S2). However, excluding Rhodin et al. 18 eliminated heterogeneity and changed the 10-year overall survival result from statistically nonsignificant to statistically significant, favoring RC (OR: 0.53; 95% CI: 0.35–0.82; I2 = 0%; Supplementary Fig. S2).
Risk of bias assessment
Most included studies exhibited a moderate risk of bias, primarily due to confounding factors. This assessment reflected the lack of procedures to match patients based on baseline characteristics. Ji et al. 23 and Yoon et al. 21 demonstrated a low risk of bias, as they performed propensity score matching to minimize the effects of confounding and selection bias. In contrast, Shao et al. 19 showed a serious risk of bias, as their data, derived from the SEER database, lacked essential baseline information necessary for an adequate comparison of interventions. Figure 3 summarizes the risk of bias assessment.
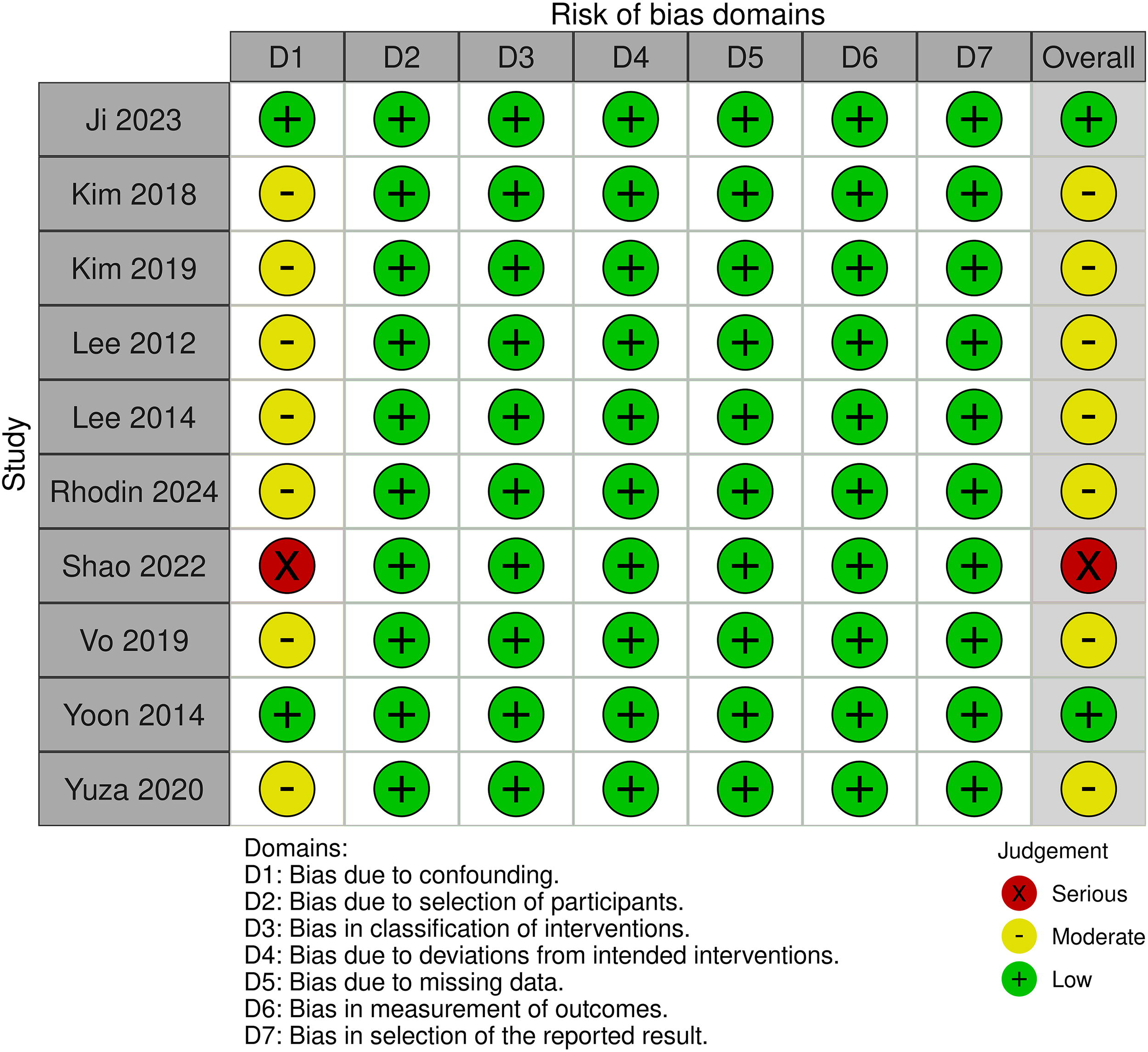
Critical appraisal of studies according to Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I).
Discussion
In this systematic review and meta-analysis of ten studies involving 2,964 patients, we compared the efficacy of SC and RC for treating pathological stage T1b GBC. Our findings indicate that RC is associated with significantly higher 2-year and 5-year overall survival rates and improved 5-year disease-specific survival compared with SC. However, the 10-year overall survival rates and loco-regional or systemic recurrence rates were similar between groups.
The decision between SC and RC for T1b GBC should be based on a comprehensive evaluation of factors such as tumor histological grade, patient comorbidities, and lymph node involvement. Our results suggest that RC offers a survival advantage in the short to medium term, but this benefit becomes less certain over longer follow-up periods, as evidenced by similar 10-year survival rates. These findings may help surgeons weigh the potential benefits of a more extensive procedure like RC, particularly in patients at higher risk of lymph node metastasis, against the increased surgical complexity and morbidity risks.
Lymphadenectomy plays a crucial role in the accurate staging and prognosis of T1b GBC. Goetze et al. highlighted its importance in improving survival by ensuring the removal of potentially metastatic nodes, 24 while Cheng et al. demonstrated that en bloc laparoscopic lymphadenectomy is feasible and maintains favorable oncologic outcomes with lower complication rates. 25 Given the approximate 10% risk of lymph node metastasis in T1b cases, extended resection with lymphadenectomy remains recommended. 26 Lymph node status is the strongest prognostic factor in stage I GBC, 27 with reported lymph node metastasis rates ranging from 0% to 15.6%,14,28–30 The 8th edition of the AJCC Staging Manual recommends harvesting at least six lymph nodes for accurate staging, an increase from the previous threshold of three nodes set by the 6th edition.31,32
Tumor staging data were missing in most of the included studies, which limits the consistency of disease severity assessment across cases. Lee et al. reported lymph node metastasis in 9.9% of T1b patients, while Vo et al. found a node positivity rate of 14.8% among patients undergoing RC. In contrast, Yuza et al. observed no lymph node metastasis in their cohort, and Rhodin et al. excluded patients with positive lymph nodes from their study. This variation reflects the clinical heterogeneity within T1b GBC, emphasizing the need for individualized treatment strategies based on specific patient profiles and staging information.
Patterns of recurrence in T1b GBC remain unclear, as limited studies focus on recurrence outcomes. Our analysis found no significant differences in recurrence rates between SC and RC, suggesting comparable effectiveness in disease control. The decision to perform isolated lymphadenectomy or radical resection should be individualized and guided by a multidisciplinary team, taking into account clinical, anatomical, and biological factors. Technical challenges, such as resecting visceral-side tumors located near adjacent structures, may increase surgical complexity and impact outcomes.24,25 Therefore, the surgical approach must be tailored to optimize oncological results while preserving quality of life.
The similar 10-year overall survival rates between SC and RC indicate that the early survival benefit of RC may diminish over time. Several factors may contribute to this observation, including differences in tumor biology, patient comorbidities, the efficacy of long-term adjuvant therapies, and the limited availability of long-term data. Although RC appears to delay mortality, it may not substantially alter the long-term survival trajectory for all patients. It is important to interpret these findings with caution, given the smaller patient population available for analysis at the 10-year mark.
This study has several limitations. First, all included studies were retrospective cohorts, which may introduce selection and information biases. Second, several outcomes exhibited significant heterogeneity. However, sensitivity analyses identified the sources of heterogeneity in some cases and demonstrated that the overall findings were generally robust and not dependent on individual studies. Notably, the study by Shao et al. 19 was the only one to systematically employ LNR analysis in the SC group, which may have contributed to the observed heterogeneity.
Conclusions
RC provides a short- to medium-term survival advantage over SC in patients with T1b GBC. However, this benefit appears to diminish over longer follow-up periods. These findings highlight the importance of tailoring surgical decisions to individual patient characteristics, balancing potential benefits against surgical risks. Further high-quality, prospective studies are needed to validate these results and to refine management strategies for T1b GBC.
Footnotes
Authors’ Contributions
Conception and design: L.M.D., B.F.P., G.H.A.M., C.M.M., and S.M.P.d.F. Data acquisition: L.M.D., B.F.P., G.H.A.M., C.M.M., and S.M.P.d.F. Data analysis: L.M.D., B.F.P., G.H.A.M., C.M.M., and S.M.P.d.F. Data interpretation: L.M.D., B.F.P., G.H.A.M., C.M.M., and S.M.P.d.F. Drafting and editing the article: L.M.D., B.F.P., G.H.A.M., C.M.M., and S.M.P.d.F. Revised it critically for important intellectual content: L.M.D., B.F.P., G.H.A.M., C.M.M., and S.M.P.d.F.; All authors approved the final version of the article, including the authorship list.
Disclosure Statement
No competing interests to disclose.
Funding Information
This meta-analysis did not receive any funding.