
Abstract
Introduction:
Few studies have evaluated the relationship between vascular anatomical variations and laparoscopic gastrectomy outcomes in patients with gastric cancer. In this study, we aimed to evaluate the effects of preoperatively detected hepatic artery variations on surgical outcomes in patients with gastric cancer undergoing laparoscopic radical gastrectomy.
Materials and Methods:
A retrospective analysis was conducted on the radiological, intraoperative, postoperative, and clinical data of 186 patients who underwent laparoscopic gastrectomy for gastric cancer. Patients were divided into two groups: those with variations and those without. The distinction between the two groups was determined by preoperative radiological imaging. The impact of these variations on perioperative and postoperative complications, as well as surgical outcomes, was subsequently evaluated.
Results:
Arterial variations were identified in 69 patients (37.1%). The most prevalent arterial variation was the aberrant left hepatic artery, observed in 25 patients (13.4%). In the cohort exhibiting arterial variations, operation time (P < .001; 203 minutes [195–220] versus 191 minutes [180–202]), intraoperative blood loss (P < .001; 100 mL [70–150] versus 50 mL [40–80]), and the total number of dissected lymph nodes (P = .006; 24 [20–34] versus 21 [17–29]) were found to be significantly higher, with statistically significant differences observed between the groups.
Conclusions:
A comprehensive evaluation of radiological imaging in patients prior to laparoscopic gastric cancer surgery, employing a multidisciplinary approach and preoperative identification of potential variations, has the potential to prevent complications and enhance surgical outcomes.
Introduction
Gastric cancer is one of the most common causes of cancer-related deaths worldwide. 1 Notwithstanding the advancements in adjuvant and neoadjuvant therapy, curative surgery remains the primary treatment modality for gastric cancer. In addition to resection with appropriate surgical margins, D2 dissection including perigastric, celiac trunk, splenic artery, and hepatic artery is of vital importance in surgical treatment. Today, stage-appropriate lymph node dissection has become standard in the treatment of gastric cancer in both Eastern and Western guidelines.2,3
The role of minimally invasive surgery in the treatment of gastric cancer is increasing gradually. This is due to a reduction in postoperative complications, such as less bleeding during surgery, a shorter hospital stay, less pain, and similar oncological outcomes.4,5 However, laparoscopic surgery is not without drawbacks, including its two-dimensional and narrow visual angle, the absence of tactile sensation, the potential for manipulation difficulties in the event of complications such as large vessel injuries, and its limited range of motion. It is imperative to detect anatomical variations during preoperative radiological evaluations, especially to prevent vascular complications. Multidetector computed tomography (MDCT) is currently regarded as one of the most preferred radiological imaging modalities for the purpose of preoperative staging in patients with gastric cancer. However, given the emphasis placed on clinical staging during preoperative evaluations, vascular variations may be inadvertently overlooked. Consequently, it is imperative that patients undergo preoperative evaluation by a multidisciplinary team and that surgical and treatment plans are formulated accordingly.
A paucity of studies exists in the extant literature that evaluates the effects of vascular variations on surgical outcomes in patients with gastric cancer. Consequently, the impact of variations in vascular anatomy on laparoscopic gastrectomy outcomes remains uncertain. In this study, MDCTs of patients who underwent laparoscopic gastrectomy were retrospectively analyzed for the presence of hepatic artery variation. The objective of this study was to assess the impact of hepatic artery variations on surgical outcomes in patients undergoing laparoscopic gastrectomy.
Materials and Methods
Patient selection
From January 2020 to October 2023, patients who were diagnosed with gastric adenocarcinoma and underwent curative surgery in Ankara University Department of Surgical Oncology were retrospectively screened. Patients with available MDCT images who underwent laparoscopic gastrectomy and D2 lymph node dissection were included in the study. Patients were excluded from participation in this study if they underwent open gastrectomy due to tumor invasion of surrounding organs, underwent multiorgan resection due to invasion of surrounding organs, had a history of upper abdominal surgery, and did not undergo D2 lymph node dissection.
Study design
The patients were divided into two groups: one comprised patients with vascular variations, and the other comprised patients without such variations. This division was based on preoperative MDCTs. The analysis of surgical outcomes, intraoperative, and postoperative complications was performed according to hepatic artery variation. The following variables were evaluated: age, gender, pathological stage, tumor localization, size, the number of dissected lymph nodes, any intraoperative and postoperative complications, amount of intraoperative bleeding, need for blood transfusion, length of hospital stay, type of operation, any postoperative reoperation and rehospitalization, and the presence and type of variation. The Clavien–Dindo complication grading system was used to classify the severity of postoperative complications. Grade I patients are considered to have no need for treatment; therefore, Grade II or higher patients were included in the analysis. 6 Tumor stages were analyzed according to the eighth edition of American Joint Committee on Cancer. 7 MDCT images were retrospectively analyzed by two surgical oncologists. The retrospective nature of this study, in conjunction with the exclusion of any potentially identifiable patient data, rendered the requirement for informed consent moot. This study was approved by the Ankara University Faculty of Medicine Institutional Ethics Committee (No: 2023000752-1).
Vascular variations were classified according to the Hiatt classification. 8 Hiatt classification is based on angiographies of 1000 individuals and divides hepatic artery variations into six classes: (type 1) normal anatomy, (type 2) aberrant left hepatic artery (aLHA) originating from the left gastric artery (LGA), (type 3) aberrant right hepatic artery (aRHA) originating from the superior mesenteric artery (SMA), (type 4) aLHA originating from the LGA and aRHA originating from the SMA, (type 5) aberrant common hepatic artery (aCHA) originating from the SMA, and (type 6) other variations.
Surgical technique
All patients included in the study underwent surgery by the same experienced surgical team. In our institution, the surgical procedure and the extent of lymph node dissection are performed in accordance with the recommendations of the Japanese Gastric Cancer Treatment Guidelines. 2 The traditional approach for laparoscopic gastrectomy and D2 lymph node dissection is similar to those reported in the literature. 9 However, in the event that vascular variation is detected preoperatively, alternative techniques may be employed in conjunction with our standard surgical approach. 10
Statistical analysis
The data distribution was verified for nonparametric characteristics using the Kolmogorov–Smirnov test. Descriptive statistics were provided, with continuous variables presented as median, quartile 1 (Q1), and quartile 3 (Q3), and categorical variables presented as counts and percentages. For data exhibiting a nonnormal distribution, nonparametric Mann–Whitney U tests were applied. Chi-square analysis was used for categorical variables. Subgroup analysis for vascular variations was conducted using the Kruskal–Wallis test. Statistical significance was set at P < .05. Data analysis was performed using the Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL), version 23 for Windows.
Results
Among the 287 patients diagnosed with gastric cancer who underwent surgical treatment, 58 underwent open gastrectomy, while the remaining 229 were planned for laparoscopic gastrectomy. Of these, 16 experienced a conversion to open surgery, 11 had a history of upper abdominal surgery, 10 underwent multiorgan resection, 4 did not undergo D2 dissection, and 2 were unable to obtain MDCT images. After excluding these patients, 186 patients were included in the final analysis (Fig. 1). Of the 186 patients included in the analysis, 115 (61.8%) were male, and 71 (38.2%) were female. The median age of the patients was 64 years (range: 56–72), and the median body mass index (BMI) was 26.4 kg/m2 (range: 24.2–28). Among the patients, 42.5% were in stage 3, and approximately one-quarter of the population received neoadjuvant chemotherapy. In one-third of the patients, the tumor was localized in the upper third of the stomach, whereas in the remaining two-thirds, it was located in the middle or lower third. A total of 91 patients (48.9%) underwent laparoscopic total gastrectomy, and 95 patients (51.1%) underwent laparoscopic subtotal distal gastrectomy (Table 1).
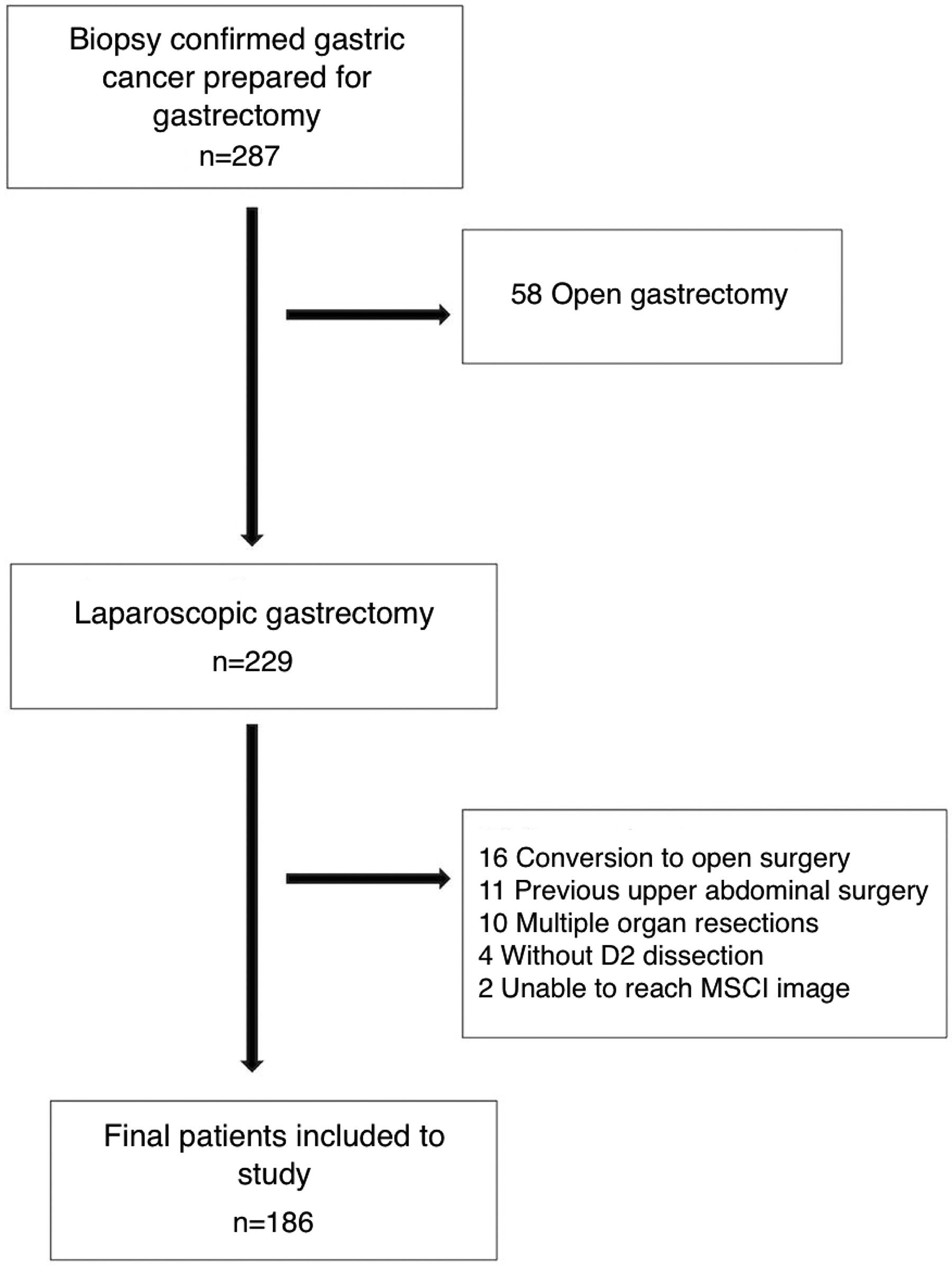
Study flow chart.
Descriptive Analysis of Demographic and Perioperative Data
BMI, body mass index; LN, lymph node; tx, transfusion.
Arterial variations were identified in 69 patients (37.1%). The most prevalent arterial variation was the aLHA, observed in 25 patients (13.4%). This was followed by the aRHA in 21 patients (11.3%), the aCHA in 11 patients (5.9%), and the combination of aRHA and aLHA in 6 patients (3.2%). Other variations were seen in 6 patients (3.2%) (Fig. 2). A statistical analysis revealed that there were no statistically significant differences between the two groups, with and without arterial variations, with respect to age, gender, BMI, tumor location, stage, and neoadjuvant therapy. These findings suggest that the two groups were homogeneous in these parameters.
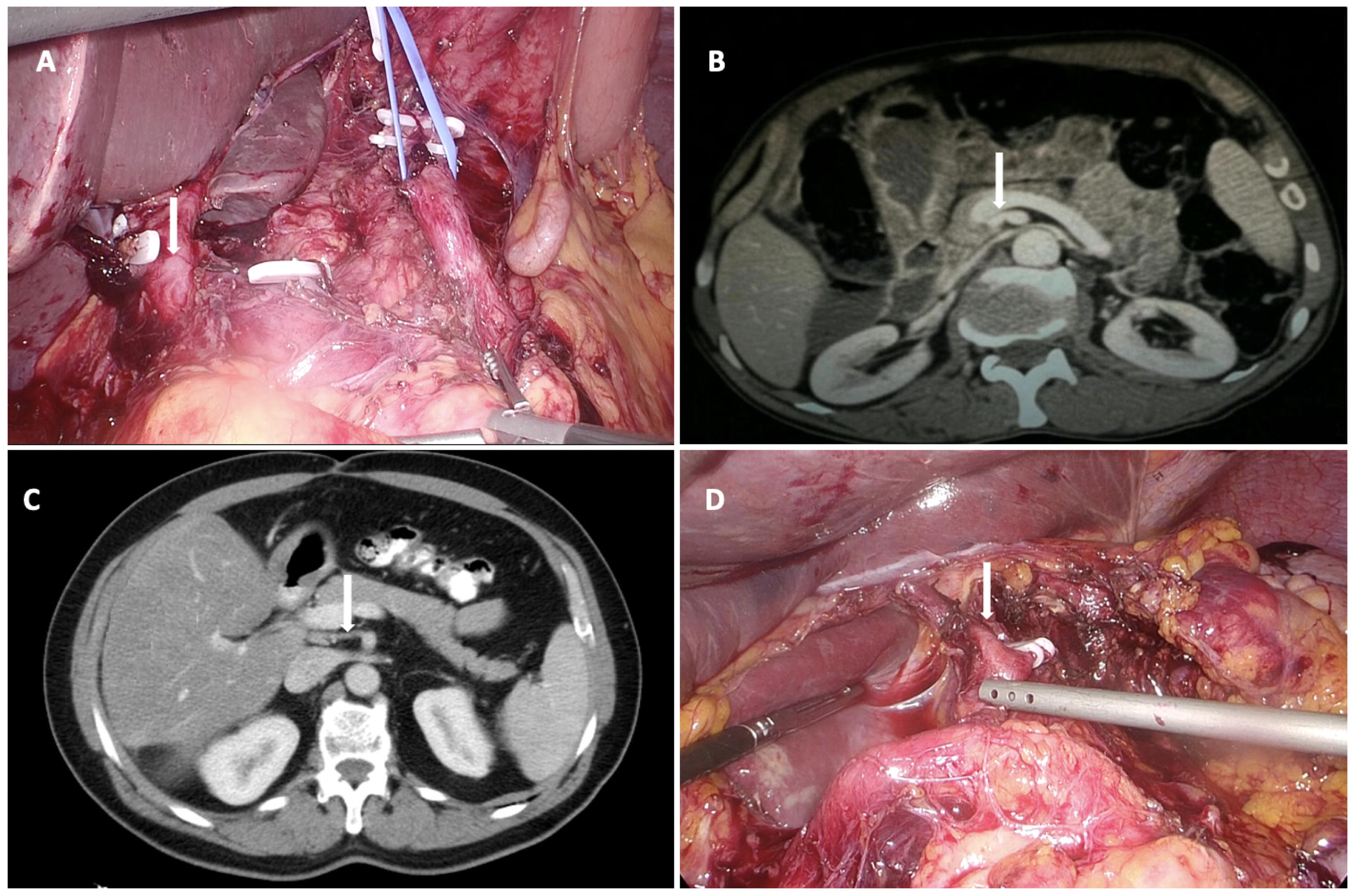
MDCT and laparoscopy images of vascular variations.
The study identified several notable variations that could be classified as Hiatt’s type 6, which are listed below:
Splenic artery originating from the SMA and an RHA passing behind the portal vein. CHA and splenic artery (SA) originating separately from the aorta, with the LGA arising from the splenic artery. LHA, middle hepatic artery, and right gastric artery originating as a trifurcation from the proper hepatic artery. Isolated trifurcation with aLHA. LGA and SA originating from the aorta, with aLHA arising from the LGA and aRHA from the SMA. Celiac trunk and SMA originating from the aorta as a single trunk.
In the cohort exhibiting arterial variations, operation time (P < .001; 203 minutes [195–220] versus 191 minutes [180–202]), intraoperative blood loss (P < .001; 100 mL [70–150] versus 50 mL [40–80]), and the total number of dissected lymph nodes (P = .006; 24 [20–34] versus 21 [17–29]) were found to be significantly higher, with statistically significant differences observed between the groups (Table 2).
Results of Univariate Analysis Between Groups
The bolded p-values in Table 2 indicate statistically significant differences between the variation and nonvariation groups.
BMI, body mass index; CD, Clavien–Dindo classification; LN, lymph node; tx, transfusion.
A subsequent investigation, employing Kruskal–Wallis analysis, was conducted on the 69 patients with arterial variations. The investigation revealed that intraoperative blood loss was most substantial in the aLHA from the LGA variation group, with a median of 150 mL (100–200; P < .001). The total number of dissected lymph nodes was found to be highest in the aCHA variation group, with a median of 27 (20–36; P = .042). Furthermore, the operation time was found to be longest in the other variation group, with a median of 217 minutes (210–230; P < .001; Table 3).
Vascular Variations According to Hiatt’s Classification and Subgroup Analysis
aCHA, aberrant common hepatic artery; aLHA, aberrant left hepatic artery; aRHA, aberrant right hepatic artery; LGA, left gastric artery; SMA, superior mesenteric artery.
Discussion
A plethora of classifications have been proposed over the course of history with respect to the vascular anatomy of the celiac trunk. Notable classifications include those proposed by Michels and Hiatt, which are employed in the context of hepatic artery variations.8,11 In the present study, the Hiatt classification was utilized to assess hepatic vascular variation, yielding a rate of 37.1%, which is slightly elevated in comparison with the rates reported in extant literature.12,13 As indicated in the extant literature, aLHA, the most prevalent variation anomaly in our study, is located in the hepatogastric ligament and may be inadvertently missed and ligated during surgery. While this may result in an elevation of postoperative liver enzymes and an extended hospital stay, spontaneous resolution is typically observed in the majority of cases. 14 However, it has been demonstrated that this may result in hepatic ischemia, particularly in patients with chronic liver disease and decreased liver function reserves. 15
In this study, we examined the effects of hepatic artery variations on surgical outcomes in patients undergoing laparoscopic gastrectomy for gastric cancer. The existing literature has employed a variety of methodologies to evaluate vascular variations, including autopsy series, angiography, and MDCT angiography. Angiography is widely regarded as the gold standard for documenting arterial anatomy. However, recent technological advances and the advent of advanced MDCT equipment have rendered it possible to obtain high-resolution and detailed images using a less invasive method. 16 Given the guidelines’ recommendation of computed tomography for preoperative clinical staging in patients with gastric cancer, all patients diagnosed with gastric cancer in our institution undergo MDCT imaging, which is then archived.17,18 Consequently, MDCT was employed to detect hepatic artery variations in the present study.
A study of 238 patients with gastric cancer undergoing radical gastrectomy found that hepatic artery variations increased operative time and intraoperative bleeding but did not significantly impact hospital stay. 19 In our study, it was observed that the amount of intraoperative blood loss and the duration of the operation were higher in patients with vascular variations. However, no relationship was identified between vascular variations and the need for intraoperative blood transfusions or perioperative complications. However, subgroup analysis of patients with arterial variations revealed significant differences in surgical outcomes. Subgroup analysis highlighted that aLHA from the LGA caused the most significant blood loss, while Hiatt type 6 variations led to the longest operation times. These findings imply that different arterial variations may present different challenges during gastric cancer surgery. In our institution, a collaborative approach is used to ensure optimal evaluation of tomography images of patients with gastric cancer. This evaluation is conducted preoperatively by a team comprising an experienced surgeon and a radiologist, with a focus on the identification of vascular variations. The treatment process of the patients is planned by a multidisciplinary team. We believe that this approach explains why complication rates are not high in patients with vascular variations.
The correlation between hepatic artery variations and the number of lymph node dissections is a salient issue that has the potential to impact surgical planning and treatment outcomes in patients with gastric cancer. A study was conducted to determine whether vascular variations affect the number of lymph nodes dissected during gastric cancer surgery. The study’s findings indicated that such variations do not have a significant impact on the number of lymph nodes dissected. 19 A subsequent study, conducted four years later at the same institution, provided further insight into the subject. The investigation revealed a decrease in the number of dissected lymph nodes among patients diagnosed with celiac artery variation. 13 However, our study revealed a noteworthy finding: patients with variations, particularly aCHA (Hiatt type 5), exhibited a significantly higher number of dissected lymph nodes when compared with those without variations. This may be attributable to the fact that vascular variations are routinely detected preoperative in our institution, and surgical planning is performed accordingly. In addition, the absence of the replaced CHA in the suprapancreatic region in patients with Hiatt type 5 variation may have enabled more effective suprapancreatic lymphatic dissection.
The aCHA, which reaches the hepatic hilus through diverse anatomical courses, may increase the likelihood of injury during laparoscopic gastrectomy. In the aCHA variation, the absence of the CHA in its normal anatomical location results in the elimination of the protective effect of the hepatic artery anterior to the portal vein. Consequently, fatal venous injuries may occur. Replaced CHA originating from the SMA has been observed with a rate of 0.4% to 4.5% in the literature.20,21 In our study, this rate was observed as 5.9%. In another study conducted in the Turkish population, aCHA was reported as 6.6%. 22 The observed rates were marginally elevated in comparison with the extant literature. Moreover, the study population exhibited a paucity of intraoperative vascular injury in patients with aCHA. It is hypothesized that this variation is more prevalent among the Turkish population. Caution should be exercised in terms of intraoperative complications.
Our study has some limitations that may affect the results. The retrospective nature of the study, the single-center setting, and the relatively small number of patients constitute the most salient limitations of the present study. Furthermore, a thorough imaging investigation of the celiac trunk and its branches was not conducted using preoperative computed tomography angiography. It is imperative that these limitations be considered during the interpretation of the study’s findings. However, the extant literature contains a paucity of studies that directly evaluate the relationship between vascular anatomical variations and laparoscopic radical gastrectomy outcomes in patients with gastric cancer. This contributes to an enhancement of the value of our study. It is hypothesized that the value of vascular variations on surgical outcomes will be confirmed by examining more homogeneous and larger patient groups undergoing laparoscopic radical gastrectomy.
Conclusions
The present study revealed that hepatic artery variations are prevalent. Patients with variations exhibited significantly longer operation times, greater intraoperative bleeding, and a higher number of dissected lymph nodes. A comprehensive evaluation of preoperative imaging and identification of variations are crucial for optimal surgical outcomes in patients undergoing laparoscopic gastric cancer surgery.
Footnotes
Authors’ Contributions
S.Ç. and S.T. contributed to protocol/project development and data analysis. M.Ş.B. and S.Ç. assisted with data collection or management and article writing/editing. S.T. and M.Ş.B. carried out article writing/editing. C.C. and İ.C.T. contributed to data analysis and data collection or management. E.A. assisted with protocol/project development and article writing/editing. A.E.Ü. and S.D. contributed to protocol/project development and data collection or management. G.G. and F.T. performed data collection or management. All authors read and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.