
Abstract
Background:
Near-infrared spectroscopy (NIRS) has been developed to monitor cerebral oxygenation. Various studies have investigated its utility in measuring somatic tissue oxygenation and in noncardiac surgeries.
Aims:
The aim of this study was to determine the effect of pneumoperitoneum on the abdominal wall.
Study Design:
A prospective, case-control study.
Methods:
This study included 70 patients who had elective laparoscopic cholecystectomy. A regional oximetry sensor was placed on the anterior abdominal wall in all patients. Primary outcome measures included preoperative regional tissue saturation (rSO2) values. For secondary outcome measures, we recorded visual analogue scale (VAS) scores and tramadol usage at postoperative hours 2, 6, 12, and 24: intraoperative end-tidal CO2 values; peripheral oxygen saturation (spo2); and abdominal subcutaneous fat tissue thickness.
Results:
The initial rSO2 value (T1: 75.6 ± 6.64) was significantly higher than those measured at the predetermined time intervals during pneumoperitoneum (T4: 73.4 ± 6.3, T5: 68 ± 8.9, T6: 68 ± 8.9, T7: 66.6 ± 9.4, T8: 65.81 ± 10.2, T9: 65.6 ± 8.8) (P < .05). The mean change in rSO2 between preoperative measurements (T1) and mid-pneumoperitoneum measurements (T8) was −12.9 ± 11%. This change was found to be negatively correlated with postoperative VAS scores and 24-hour tramadol consumption amounts.
Conclusion:
The results of the present study show that changes in abdominal wall tissue oxygenation during pneumoperitoneum can be measured with NIRS.
Introduction
Near-infrared spectroscopy (NIRS) employs a modified Beer-Lambert law to measure the concentration of a substance according to the absorption and scattering of light that is sent. The NIRS devices provide a noninvasive assessment of tissue oxygenation by quantitatively evaluating the color of hemoglobin in the blood. During the measurement of cerebral/somatic regional oxygen saturation with NIRS, it is expressed that the infrared light sent shows the saturation of a region with a depth of approximately 2–3 cm beneath the sensor through the detector. 1
Such an effect allows the use of NIRS in a wider series of tissues other than fingers, toes, and earlobes, as is the case with pulse oximetry. This technology is currently FDA-approved for the noninvasive, continuous monitoring of regional perfusion of cerebral and somatic tissues. 2 NIRS is often used during cardiac surgery to assess cerebral oxygenation, the regional cortical oxygenation (rSO2) over the frontal region of the patient. 3
Even though NIRS was developed to monitor cerebral oxygenation, various studies have tried to use it during noncardiac surgery besides cardiac surgery and for the assessment of somatic tissues. 4 Some of these various areas are abdominal organs, especially in the pediatric age group, and muscle tissues in the adult age group.5–7
The aim of such studies that used NIRS for areas other than cerebral tissues is to detect and monitor ischemia. Currently used for laparoscopic surgical methods, pneumoperitoneum may cause compression and decreased blood flow due to the pressure effect of the abdominal wall, abdominal organs, and vascular structures. Although it is tried to reduce the pressures of insufflated gases, there may be effects due to the increased intraabdominal pressure.8–9
The aim of this study was to determine the effect of pneumoperitoneum on the abdominal wall. To this end, we hypothesized that the ischemic effect of pneumoperitoneum on the abdominal wall could be determined through NIRS.
Materials and Methods
Patient selection
After obtaining the local ethics committee approval and registering in the clinical trials, this prospective study evaluated 100 patients who were scheduled for laparoscopic cholecystectomy (Bursa Yüksek İhtisas Training and Research Hospital Ethics Committee App. No: 2018-1/32, ClinicalTrials.gov identifier: NCT03589404). The study included consenting patients aged 18–65 years who were scheduled for laparoscopic cholecystectomy and in the risk class of ASA (American Society of Anesthesiologist) Score I-II. Exclusion criteria were established as previous abdominal surgery, mental disorders, allergic reactions to the medications used, and a body mass index (BMI) above 30.
The study included 72 patients based on inclusion and exclusion criteria. Prior to the induction of anesthesia, an abdominal wall ultrasonography (10–18 MHz, MyLab30; Esaote, Florence, Italy) was performed on all patients between the mid-clavicular line and anterior axillary line at the level of the umbilicus in the abdominal region; the distance from muscle tissue to abdominal adipose tissue was measured and recorded; and the area was marked. (Fig. 1) Upon site cleaning suitable for the marked area, the regional oximetry probe (Medtronic Quick Asist INVOS TM 5100C Cerebral/Somatic Oximeter) was placed. The probe was covered in a sterile way. (Fig. 2) For the induction of anesthesia, all patients were administered propofol and rocuronium bromide. The maintenance of anesthesia was ensured by delivering sevoflurane at a flow of 2.5–3 L/min in a mixture of air and O2. A volume-controlled mode was used for mechanical ventilation. Ventilation was set to 0.8 mg/kg, and intraoperative CO2 values were anesthesia device’s end-tidal CO2 module values. Analgesia was provided by administering a single-dose NSAID before the end of the operation and postoperative tramadol using a PCA (patient-controlled analgesia) device (a saline solution with 5 mg tramadol per ml, lock-out time 30 minutes, demand dose 25 mg, for PCA protocol).

Sonoanatomy of the abdominal adipose tissue in the lateral abdominal area.

NIRS sensor application area. NIRS, near-infrared spectroscopy.
Outcome measures
Primary outcomes: Peripheral tissue oxygenation (Medtronic Quick Asist INVOSTM 5100C Cerebral/Somatic Oximeter) values at T1: preoperative, T2: during intubation, T3: 5 minutes after intubation, T4: start of pneumoperitoneum, T5: 5 minutes pneumoperitoneum, T6: 10 minutes pneumoperitoneum, T7: 20 minutes pneumoperitoneum, T8: 30 minutes pneumoperitoneum, T9: termination of pneumoperitoneum, T10: 5 minutes after pneumoperitoneum, T11:10 minutes after pneumoperitoneum, T12: during extubation, T13: 5 minutes after extubation, and T14: 10 minutes after extubation. Secondary outcomes: VAS scores and tramadol usage at postoperative hours 2, 6, 12, and 24; intraoperative end-tidal CO2 values; peripheral oxygen saturation (spo2); and abdominal subcutaneous fat tissue thickness.
Statistical analysis
Data analysis was done using SPSS 22.0 statistical software; the chi-square 2 test and descriptive statistical method were used for categorical variables. The Shapiro-Wilk test was used for distribution normality of data. Repeated measures one-way ANOVA test and Bonferroni test were used for post-hoc analysis. Pearson’s correlation test was performed for the relationship between NIRS measurement values and abdominal fat thickness, VAS scores, and tramadol consumption. A value of P < .05 was considered significant.
Results
The study was completed with a total of 70 patients since it was proceeded with open surgery in 1 patient, and a device problem occurred in another patient during follow-up. Demographic data of patients are presented in Table 1. The initial rSO2 values (T1: 75.6 ± 6.64) were found to be statistically significantly lower when compared with the rSO2 measurements at predetermined time intervals during pneumoperitoneum (T4: 73.4 ± 6.3, T5: 68 ± 8.9, T6: 68 ± 8.9, T7: 66.6 ± 9.4, T8: 65.81 ± 10.2, T9: 65.6 ± 8.8) (P < .05) (Fig. 3). The rSO2 values during intubation (T2: 78.6 ± 0.6), at 5 minutes after intubation (T3: 78.4 ± 5.5), during extubation (T12: 76.8 ± 8.8, at 5 minutes after extubation (T13: 77.2 ± 6.4) and at 10 minutes after extubation (T14: 77.5 ± 6) were found to be statistically significantly higher when compared with the initial measurement values (P < .05) (Fig. 3).
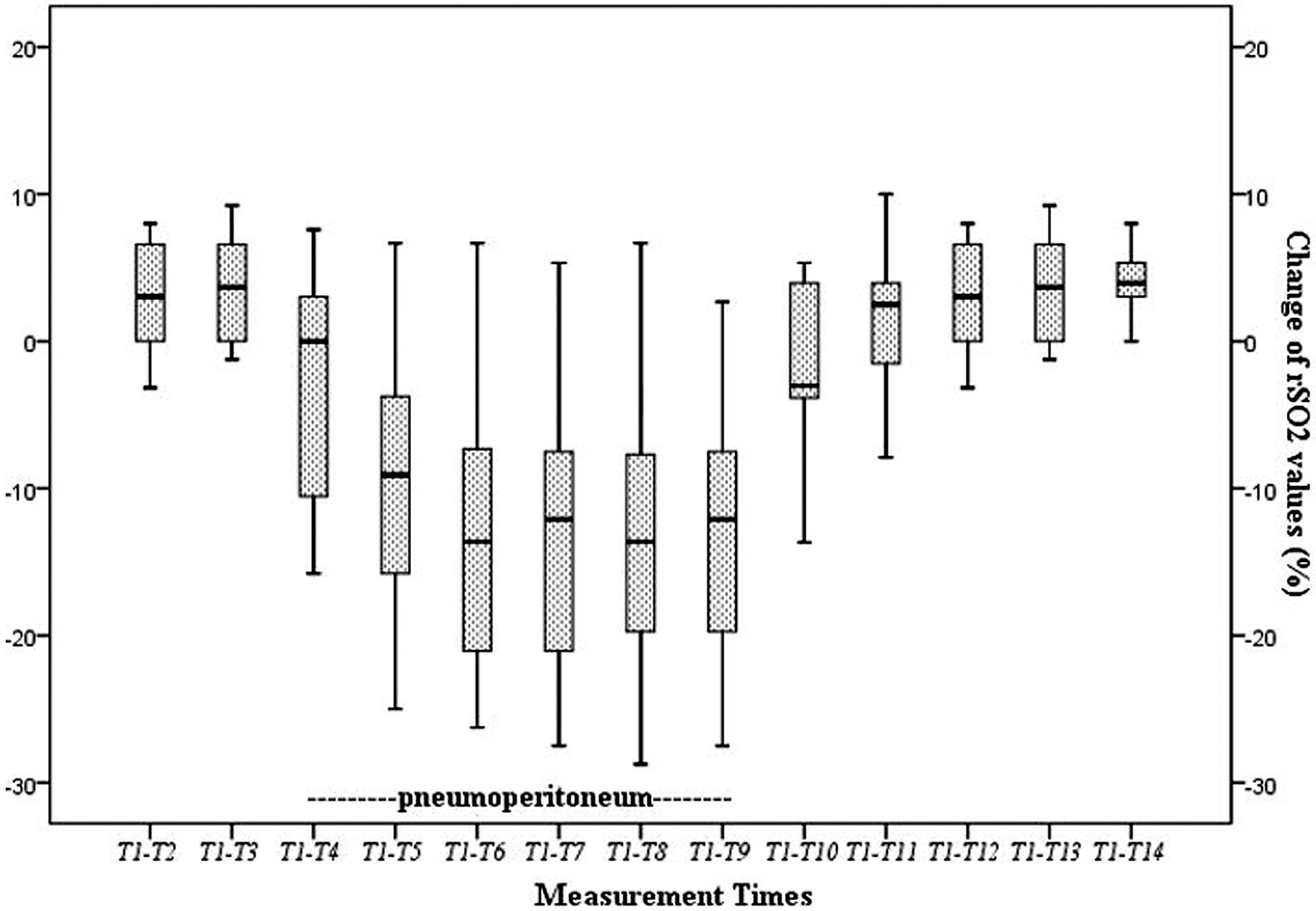
rSO2 percentage changes. rSO2, regional tissue saturation.
Comparison of the Demographic Characteristics of the Patients
Median (min; max) values.
BMI, body mass index; M, male; F, female; ASA, American Society of Anesthesiologists; min, Minute.
The mean rate of change in rSO2 values between preoperative measurement (T1) and mid-pneumoperitoneum measurement (T8) was found to be −12.9% ± 11 (Fig. 2). Such rate of change was found to be negatively correlated with postoperative VAS scores and the 24-hour tramadol consumption amounts (Table 2).
Correlation between Postoperative VAS Scores, 24-Hour Tramadol Consumption Amounts and Mean Change rSO2 Measurements (between T1-T8)
Pearson’s correlation test.
VAS, visual analogue scale.
No statistically significant difference was established in the end-tidal CO2 values recorded at all measurement timepoints, including pneumoperitoneum throughout the operation (P < .05). (Table 3) There was a low-level negative correlation between abdominal adipose tissue thickness at the NIRS measurement site and initial rSO2 measurements (Fig. 4).

Correlation between initial rSO2 measurements and abdominal subcutaneous fat thickness. rSO2, regional tissue saturation.
Intraoperative rSO2, ETCO2, and SpO2 Measurements
Discussion
Findings of the present study demonstrated that the rSO2 values obtained over the abdominal wall during pneumoperitoneum in laparoscopic cholecystectomy with NIRS can measure the changes in tissue oxygen saturation in a noninvasive way.
There are studies demonstrating that the NIRS system, which was manufactured to detect the changes in brain tissue oxygenation by placing it on the frontal region, is currently applicable to somatic tissues other than cerebral tissues.5–7 The literature involves prominent studies that evaluate the perfusion of abdominal organs among patients in the pediatric age group other than cerebral tissues. Evaluated the circulation of the intestinal system in the neonatal period; such studies reported that NIRS might be a predictor. 5 Muscle is another tissue used in studies that assessed oxygenation in organs other than brain.6–7 Studies, which used NIRS to detect the oxygenation of muscle tissues in a noninvasive way, in turn, aimed to assess oxygenation mostly in cases of ischemia. Fellaini et al. tried to establish the effects of vascular occlusion induced on the lower extremity using NIRS detectors among 20 healthy volunteers. The normal peripheral rSO2 values at the lower extremity after the induced vascular occlusion differed from the other extremity with normal flow. The authors indicated that the NIRS technology should be taken into account in further diagnostic and prognostic clinical trials. 10
Another study with healthy participants used the thenar area of the hand as the NIRS measuring site. The aim was to determine the tissue oxygenation through ischemia and reperfusion induced on the hand. The authors compared two different NIRS devices and reported that NIRS could be used to assess and monitor microcirculation. 11 Two different studies that used NIRS to measure regional oxygen saturation beside ischemia, in turn, evaluated patients who had nerve blocks within this scope. A statistically significant increase was found in rSO2 values after the block in patients who received popliteal block for foot surgery, while the study by Tighe et al. evaluated the impact of three different types of peripheral nerve block. The authors demonstrated that the rSO2 values obtained using the Somanetics Invos NIRS system detected the changes in tissue oxygen saturation in a non-invasive way.12,13 For the oxygenation of the abdominal region, the literature contains a limited number of studies that use NIRS, except for newborns. An animal study by Varela et al. investigated the effects of abdominal compartment syndrome on the changes in mesenteric and systemic perfusion using an NIRS probe that was invasively placed on the gastric tissue. The authors established that the NIRS-derived gastric tissue oxygenation was associated with mesenteric perfusion parameters. 14 Another study, which used an NIRS probe in an anatomical site similar to the one used in the present study, was conducted by Widder et al. Conducted with 9 intensive care patients, the study found a significant negative correlation between increased intraabdominal pressure and abdominal wall tissue oxygenation. The authors reported that an increased intraabdominal pressure might cause increased abdominal wall tension, which, in turn, might result in reduced perfusion. 15
This study found the rSO2 values in the abdominal muscle tissue during pneumoperitoneum to be statistically significantly lower than the initial values. Several studies have demonstrated variability in blood flow in the intraabdominal tissues due to the pressure effect caused by gas insufflation during pneumoperitoneum.
NIRS measurements support that it can show the effect of these pressure changes on the abdominal wall muscle tissue. The present study also established results similar to the decrease in rSO2 values measured at the extremity muscles when ischemia was induced. In addition, such results are in parallel with the study by Widder et al. that reported the changes caused by increased intraabdominal pressure on peripheral tissue oxygenation of the abdominal wall. 15 Another remarkable finding of our study was the elevated abdominal wall rSO2 values measured at room air that we believed to be due to the increased amount of oxygen inhaled during and after the induction of anesthesia.
The postoperative VAS scores and tramadol consumption amounts determined as the secondary outcomes were positively correlated with rSO2 values measured during pneumoperitoneum. Likewise, Gentillelo et al. found reduced tissue oxygen saturation and increased VAS scores. 16
NIRS sensors seem to be sensitive to the changes in somatic tissue oxygen, despite certain limitations (melanin concentration in skin, adipose tissue amount, etc.). 17
Recommended as a trend monitor instead of single measurements, NIRS measurements can be used as a noninvasive method for tissue oxygenation.17,18
In addition, especially in cases when repeated measurements are required, it has been reported to be valuable for the follow-up of patients with limited test options. 17
Limitations
The primary limiting factors included the measurement site’s adipose tissue thickness, cutaneous blood flow, skin pigmentation (melanin content), and the hemoglobin, myoglobin, and cytochrome oxidase content of skeletal muscle tissue. The adipose tissue thickness (ATT) under the measurement site appears to be one of the limitations. As a common problem for all studies measuring the somatic tissue oxygenation, the adipose tissue is believed to reduce the contribution of the skeletal muscle desired to be measured to the NIRS signals. As both the numerator and the denominator will be affected to a similar extent, when rSO2% is a primary NIRS outcome variable, it is reported that corrected measurements for ATT may not be required. 17 By measuring the adipose tissue thickness at the abdominal wall using an ultrasound at the measurement site, we tried to use the NIRS probe in the region with the least adipose tissue. Our study established a negative correlation between abdominal fat thickness and NIRS, suggesting that the adipose tissue at the measurement site is of a limiting nature. 17
Another limiting factor for the use of NIRS is the levels of hemoglobin, myoglobin, and cytochrome oxidase in the muscle tissue. It was reported that the contribution of cytochrome oxidase to the NIRS signals can be ignored due to its relatively low concentration.17–19
Nevertheless, the failure to detect the effect of hemoglobin and myoglobin on the measurements was a limitation of this study. Other limitations included the failure to detect the effect of patients’ skin pigmentation level and cutaneous blood flow on NIRS measurements and the BMI group that involved the patient group being not representative of the general population.
Conclusion
The findings of the present study demonstrated that changes in muscle tissue oxygenation can be established through measurements with NIRS over the abdominal wall during pneumoperitoneum. Despite its limitations, we believe that the increased tissue oxygenation at 100% O2 delivery during intubation should be taken into account for the reliability of the measurement as much as the change the occurred during the increased abdominal pressure.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.