
Abstract
Background:
This study aimed to contribute to the ongoing debate regarding the optimal age to initiate colorectal cancer (CRC) screening by evaluating adenoma detection rates (ADRs) across different age and sex groups and to explore whether national screening guidelines should be revised in line with international trends.
Methods:
In this single-center, retrospective observational study, 1216 average-risk patients who underwent colonoscopy between January and December 2024 were analyzed. The patients were stratified into three age groups: Group 1 (40–44 years), Group 2 (45–49 years), and Group 3 (50–54 years). ADR, advanced neoplasia detection rate (ADNR), ADR by sex, Boston Bowel Preparation Scale (BBPS) score, and withdrawal times were evaluated. Patients with a history of polypectomy, family history of CRC, incomplete colonoscopy, or inadequate bowel preparation (BBPS score <6) were excluded. Group comparisons were performed using Chi-square or Fisher’s exact tests, with P < .05 considered statistically significant.
Results:
Overall ADR and ADNR were 20.8% and 2.6%, respectively. ADRs by group were 7.6%, 15.8%, and 18.9% in Groups 1, 2, and 3, respectively. A significant difference was found between Groups 1 and 2 (P = .032) but not between Groups 2 and 3 (P = .55). ADR was significantly higher in males (30.2%) than in females (13.1%; P < .001). ADNR was also higher in males (3.7%) than in females (1.8%; P = .048). All patients had withdrawal times >6 minutes.
Conclusion:
ADR significantly increased from age 45, supporting the potential need to lower the CRC screening age and consider sex-specific strategies. Further prospective multicenter studies are warranted.
Introduction
Colorectal cancer (CRC) is a major cause of morbidity and mortality worldwide. 1 Screening programs are effective in reducing mortality rates through the detection of premalignant lesions and early-stage CRC. 2 As most cases originate from adenomatous polyps, early detection and timely management of these lesions are of critical importance. Colonoscopy is considered the gold standard for CRC screening and plays an important role in polyp detection and removal. 3 The adenoma detection rate (ADR), a basic parameter used to evaluate the effectiveness of colonoscopy, may vary according to age groups. Therefore, the age at which colonoscopy screening is initiated is important in screening programs.4,5
In our country, for individuals without a family history, screening is recommended starting at the age of 50 years, with colonoscopy every 10 years and fecal occult blood testing every 2 years. However, owing to the increasing incidence of CRC in younger age groups in recent years, the American Cancer Society has recommended lowering the screening age from 50 to 45 years. 6 This recommendation emphasizes that initiating colonoscopy screening at the age of 45 years is important for the early detection of CRC and for reducing mortality.
In Turkey, current guidelines recommend initiating CRC screening at the age of 50 years for individuals at an average risk. However, considering global trends and updated international guidelines, discussions on reducing screening age in Turkey are ongoing. This study aimed to analyze ADR according to age groups and sex in order to assess the appropriate age for CRC screening and the influence of sex and to compare the findings with existing guideline recommendations.
Materials and Methods
Ethical approval for this single-center, retrospective, and observational study was obtained from the Clinical Research Ethics Committee of the University of Health Sciences Antalya Training and Research Hospital (Ethics Committee number: 2025-98, date: March 13, 2025). Colonoscopy procedures performed by five endoscopists at the General Surgery Department of Antalya Training and Research Hospital between January 2024 and December 2024 were retrospectively evaluated. This study was conducted in accordance with the principles of the Declaration of Helsinki. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines for patient enrollment and allocation were followed.
This study included patients aged 18–95 years who underwent colonoscopy at the General Surgery Department of Antalya Training and Research Hospital between January and December 2024, had adenomas detected, had a complete and valid colonoscopy report, and had an available pathology report. Patients with a history of polypectomy, personal or family history of CRC, incomplete colonoscopy procedures, colonoscopy due to inflammatory bowel disease, inadequate bowel preparation, or missing pathology reports were excluded.
Patients who underwent colonoscopy and met the inclusion criteria were evaluated retrospectively. Patients in whom adenomas were detected during the procedure were categorized into three age groups: Group 1 (40–44 years), Group 2 (45–49 years), and Group 3 (50–54 years). ADR across all age groups, ADR by sex, Boston Bowel Preparation Scale (BBPS), and withdrawal time were evaluated. In addition, the demographic characteristics (age and sex) of the included cases, colonoscopy-related parameters, indications, total number of polyps, diameter of the largest polyp, histological subtypes of the polyps, overall ADR, and advanced neoplasia detection rate (ADNR) were retrospectively evaluated using the hospital database.
ADR is defined as the rate at which a physician detects at least one precancerous adenoma during a colonoscopy. ADR was calculated as the percentage of patients in whom at least one adenoma was detected divided by the total number of colonoscopies completed with adequate bowel preparation. 7 A polyp is defined as proliferative growth of tissue projecting from the colonic mucosa into the lumen, whereas an adenoma is considered a polyp that arises from the normal colonic epithelium and carries precancerous potential. 8 In the present study, adenomas detected during colonoscopy, including biopsy samples obtained and polypectomies performed, were recorded in detail, and the total number of lesions was thoroughly documented. Lesions classified as advanced neoplasia were defined as those ≥1 cm and/or high-grade dysplasias.
In the present study, the BBPS was used to assess the quality of bowel preparation in patients who underwent colonoscopy. The BBPS assesses bowel cleanliness by individually scoring three colonic segments (right, transverse, and left colon) on a scale from 0 to 3. 9 In the present study, bowel preparation scores during colonoscopy were documented by the endoscopist, and the total BBPS score was calculated on a scale from 0 to 9. Patients with a BBPS score <6 and/or any colon segment score <2 were classified as having inadequate bowel preparation and excluded from the study.
Colonoscopy and Polypectomy Procedure
Patients who underwent bowel cleansing and received sedoanalgesia were placed in the left lateral decubitus position, followed by a perianal examination and digital rectal inspection. Subsequently, the colonoscope was advanced through the anus and navigated through the rectum, sigmoid colon, descending colon, transverse colon, and ascending colon to the cecum. Luminal distension was achieved by insufflation to provide optimal visualization conditions. During withdrawal, the entire colonic mucosa was thoroughly examined and retroflexion was performed to evaluate the rectal ampulla and anal region. A minimum withdrawal time of 6 minutes was ensured for all procedures. Small pedunculated polyps detected during the procedure were excised using cold forceps biopsy, whereas larger pedunculated or sessile polyps were removed using hot snare polypectomy.
Statistical analysis
All statistical analyses were performed using Jamovi software version 2.6.26. Descriptive statistics are presented as frequency (n) and percentage (%) for categorical variables and as mean ± standard deviation for continuous variables. To assess the differences between groups, the Chi-square test was used for the comparison of categorical variables, and Fisher’s exact test was applied when the expected cell frequencies were low. Statistical significance was set at P < .05.
Results
Data from 1852 patients who underwent colonoscopy between January and December 2024 were reviewed, and 636 patients were excluded from the study. The exclusion criteria were history of polypectomy (224 patients), family history of CRC (210 patients), incomplete colonoscopy (76 patients), colonoscopy performed due to inflammatory bowel disease (24 patients), and inadequate bowel preparation (BBPS <6; 102 patients). A total of 1216 patients who met the eligibility criteria, regardless of age group, were included in the final analysis (Fig. 1).
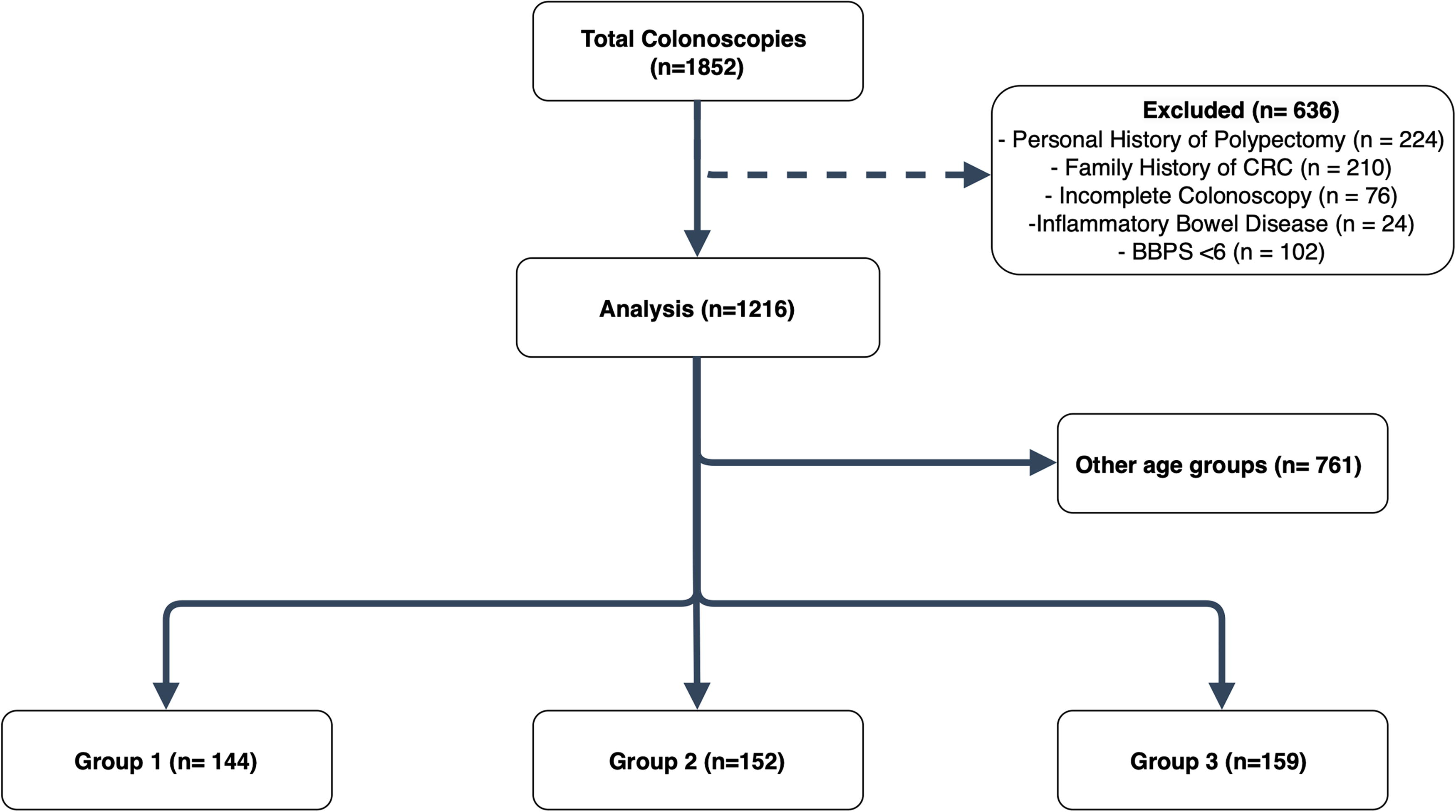
Flowchart.
Demographic data
Among the patients included in the study, 44.9% were male (546 patients) and 55.1% were female (670 patients). The mean patient age was 55 ± 13.1 years. The patients included in the study presented with various indications, the most common of which were constipation, screening, abdominal pain, anemia, and rectal bleeding. Among patients under the age of 50, constipation was the most frequent indication (51.2%), whereas in those aged 50 and above, the most common indications were constipation (43.2%) and screening (23.5%). The mean withdrawal time for all patients was calculated as 412.11 ± 45.22 seconds, and the mean BBPS score was 7.97 ± 1.1 (Table 1).
Demographic Data
Values presented as mean ± SD and number (%).
BBPS, Bowel Boston Preparation Scale; SD, standard deviation.
Pathological data
In the present study, 253 patients (20.8%) had at least one adenoma, whereas advanced neoplasia was detected in 32 patients (2.6%), including 24 with high-grade dysplasia and 8 with polyps larger than 1 cm. A total of 503 polyps were detected, most of which were adenomatous. Tubular adenomas were found in 50.3% of the patients, tubulovillous adenomas in 18.1%, and villous adenomas in 2.6%. Additionally, 8 tubular adenomas and 10 tubulovillous adenomas were found to have high-grade dysplasia, with 1 lesion from each group identified as intramucosal carcinoma. High-grade dysplasia was detected in 30.7% (4 13) of villous adenomas. Among the other types of polyps, hyperplastic polyps accounted for 16.9%, inflammatory polyps for 4.4%, sessile serrated adenomas for 1.4%, and both fibroepithelial polyps and lymphoid hyperplasia for .8% (Table 2).
Pathological Data
Values presented as number (%).
ADR analysis in age groups
A total of 144 patients in Group 1, 152 patients in Group 2, and 159 patients in Group 3 who met the eligibility criteria were included in the analysis. When ADR rates were analyzed by the age group, they were 7.6% (11 patients), 15.8% (24 patients), and 18.9% (30 patients) in the 40–44, 45–49, and 50–54 age groups, respectively. The mean BBPS score was 7.18 ± 1.10 in Group 1, 7.41 ± 1.04 in Group 2, and 7.59 ± 1.08 in Group 3. The mean withdrawal times were calculated as 439.03 ± 35.60 seconds, 457.04 ± 38.12 seconds, and 445.03 ± 39.10 seconds, respectively. Statistical analysis revealed a significant difference in ADR between the 40–44 and 45–49 age groups (P = .032); however, no statistically significant difference was found between the 45–49 and 50–54 age groups (P = .55; Table 3).
ADR by Age Groups and Statistical Analysis Results
Values presented as number (%).
Group 1 = 40–44 age group; Group 2 = 45–49 age group; Group 3 = 50–54 age group.
Chi-square and Fisher’s exact test were used for comparisons.
P < .05 was considered statistically significant.
ADR, adenoma detection rate.
Sex-based analysis of ADR and ADNR
When ADR was evaluated by sex, it was calculated to be 30.2% (165 patients) in males and 13.1% (88 patients) in females, with a statistically significant difference between groups (P < .001). The ADNR was 3.7% (20 patients) in males and 1.8% (12 patients) in females, with a statistically significant difference between the groups (P = .048). When the age groups were evaluated by sex, the ADR in males was 12.7% (8 patients) in the 40–44 years age group, 24.6% (16 patients) in the 45–49 years age group, and 23.2% (16 patients) in the 50–54 years age group. In females, the corresponding ADRs were 3.7% (3 patients), 9.2% (8 patients), and 15.6% (14 patients), respectively. A statistically significant difference in ADR between male and female patients was observed in Groups 1 and 2 but not in Group 3 (P = .044, P = .01, and P = .223, respectively; Table 4).
ADR Analysis by Gender
Values presented as % (number).
Group 1 = 40–44 age group; Group 2 = 45–49 age group; Group 3 = 50–54 age group.
Chi-square and Fisher’s exact test were used for comparisons.
P < .05 was considered statistically significant.
ADR, adenoma detection rate; ADNR, advanced neoplasia detection rate.
Discussion
The current study evaluated ADR across different age groups in average-risk individuals, aiming to contribute data that may guide recommendations on the appropriate age to initiate CRC screening. In the current study, a notable difference in ADRs was observed across age groups, with a statistically significant increase between the 40–44 and 45–49 age groups. However, the ADR was comparable between the 45–49 and 50–54 age groups. Among all the patients included in our study, the overall ADR was 20.8%, whereas the ADNR was 2.3%. When stratified by sex, the ADR was 30.1% in male patients and 13.1% in female patients, which was statistically significant.
ADR is one of the most important parameters in determining the effectiveness and quality standards of colonoscopy and has been shown in numerous studies in the literature to be a critical quality indicator reflecting an endoscopist’s success in detecting polyps and adenomas. 10 Several studies have demonstrated that ADR increases with age. 5 In a retrospective cohort study conducted by Karsenti et al., ADR was reported to be significantly lower in individuals under the age of 45 but showed a marked increase after age 45. 11 Similarly, in a retrospective study by Mitsuhashi et al., a comparison between the 45–49 and 50–54 age groups revealed no statistically significant difference in ADR. 4 Based on these findings, it has been suggested that lowering the starting age of CRC screening programs to 45 years may be appropriate. The results of the present study are consistent with the literature, demonstrating that ADR rates were low, particularly in the 40–44 years age group, but showed a significant increase after the age of 45 years. However, a study by Karsenti et al. showed that the ADR was 25% in the 45–49 years age group and over 30% in the 50–54 years age group. According to the guidelines of the European Society of Gastrointestinal Endoscopy (ESGE), excluding emergency colonoscopies, the target ADR in individuals aged ≥50 years was set at 25%. 12 This rate was higher than the ADR values observed in our study, and this discrepancy is thought to be attributable to various factors. First, geographical and ethnic differences may play a significant role in the development of colorectal neoplasia. In Western populations, factors such as dietary habits, high consumption of processed foods, high-fat diets, and sedentary lifestyles are more prevalent, which may have contributed to the lower ADR observed in our study. Additionally, the inclusion of results from five different endoscopists in our study may be another contributing factor to this outcome.
When calculating ADR, it is important to include only appropriate patient populations to ensure accurate and meaningful assessment of quality. The ESGE and the American College of Gastroenterology recommend that ADR be measured in individuals at an average risk of undergoing screening colonoscopy. 13 Accordingly, in the present study, individuals with a personal history of polypectomy or a family history of CRC were excluded. These patients are typically excluded from the screening protocol and placed under surveillance, which may be associated with increased ADR. This consideration may affect the generalizability of the findings obtained from the overall population; therefore, exclusion criteria were carefully defined. Indeed, in a multicenter randomized controlled trial conducted by Liu et al., patients with inflammatory bowel disease, family history of CRC, or history of polypectomy were also excluded from the study. 14 However, in a study conducted by Karsenti et al., no significant difference in ADR was found between high-risk individuals and those at average risk, aged 45 years and above. 11 In this context, the exclusion of high-risk individuals in our study was intended to ensure that the data more accurately reflected the average-risk population.
Although age is considered the most important determining factor in CRC screening programs, no clear prioritization has been established regarding the impact of sex. In a study by Regula et al., the rates of adenoma and advanced neoplasia were reported to be higher in male patients than in female patients across different age groups. 15 The literature supports that the risk of CRC is higher in men than in women, as demonstrated in several studies.16,17 In this study, male patients exhibited higher ADR than female patients in all age groups except the 50–54 age group. These findings support the need to re-evaluate current CRC screening recommendations by considering sex.
Withdrawal time during colonoscopy is an important indicator of procedural quality and is directly associated with ADR. In a study conducted by Wong et al., the ADR was reported to be 11% among endoscopists with a withdrawal time of <6 minutes compared with 28% in procedures lasting 6 minutes or longer.18,19 These results indicate that adequate withdrawal time is associated with a significant increase in ADR. Another study reported that a longer withdrawal time increased ADRs and enhanced the effectiveness of colonoscopic screening. 19 In the present study, the mean withdrawal time was calculated to be over 6 minutes for all patients and age groups. Our findings were consistent with those reported in the literature. This may be a factor that enhances the reliability of the observed ADR rates and suggests that comparisons between age groups yield more accurate results.
In the present study, bowel preparation quality was assessed using BBPS. The BBPS is a standardized scale developed to evaluate the adequacy of bowel cleansing during colonoscopy, and it is well established that adequate bowel preparation is essential for high-quality colonoscopy. 9 Although Lai et al. did not establish a specific threshold for adequacy, subsequent studies have widely adopted a total BBPS score ≥6 as an indicator of sufficient bowel preparation.9,20 This threshold is based on evidence indicating that a BBPS score of <6 is associated with suboptimal visualization of the colonic mucosa and may potentially lead to reduced adenoma and polyp detection rates. 21 However, although some studies have reported no significant correlation between bowel preparation quality and ADR, 22 in our study, patients with a total BBPS score <6 and/or a segmental score <2 in any colon segment were classified as having inadequate bowel preparation and excluded from the analysis. This approach is considered to have contributed to the more reliable and accurate results in the group comparisons in our study.
The retrospective design of the study and use of retrospectively collected data may introduce certain observational biases. Additionally, the single-center nature of this study may limit the generalizability of our findings to other populations. Although bowel preparation quality was assessed using the BBPS score, the lack of analysis of other variables such as dietary habits, lifestyle factors, and genetic risk limits the comprehensive interpretation of the results. Finally, unless supported by prospective and multicenter studies, the applicability of these findings in national screening programs remains limited.
Conclusion
In our study, a marked increase in ADR was observed beginning at age 45 years, reaching levels comparable with those observed in the 50-year-old age group. Sex-based analyses revealed that the ADR was higher in males than in females. These findings support the need to consider lowering the CRC screening age to 45 years and incorporating sex into screening strategies. However, these results should be validated in large-scale, prospective studies.
Footnotes
Authors’ Contributions
B.S.: Conceptualization; O.C. and T.C.Y.: Methodology; A.C. and B.S.: Data curation; B.S. and U.D.: Formal analysis and investigation; B.S., O.C., and O.Z.O.: Writing—original draft preparation; B.S. and O.I.D.: Writing—review and editing; B.S.: Supervision. All authors commented on the previous versions of the article. All authors have read and approved the final article.
Data Availability Statement
All data generated and analyzed during this study are included within the article and are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
The authors declare no financial support for this study.