
Abstract
Purpose:
Esophageal squamous cell carcinoma (ESCC) located at the cervicothoracic junction (CTJ-ESCC), approximately 18–21 cm from the incisors, poses unique surgical difficulties given its proximity to the trachea and recurrent laryngeal nerves. This investigation evaluated a new approach that avoids cervical incisions by combining the EGIARADMT™ curvilinear stapling method with OrVil™-based three-dimensional suspension anastomosis (TriSAS) to achieve R0 resection.
Methods:
A retrospective analysis was performed on 11 consecutive cases of CTJ-ESCC treated between February 2019 and March 2024, with follow-up data available until February 2025.
Results:
All patients underwent R0 resection without cervical incisions, achieving a proximal margin of 1–4 cm. The median operative time was 350 minutes (range: 275–605) with a blood loss of 100 mL (range: 20–700). Lymphadenectomy resulted in a median of 21 nodes (range: 9–38) being retrieved. The median duration of hospitalization was 49 days (range: 42–67). There were no occurrences of anastomotic leaks, strictures, or recurrent laryngeal nerve injuries. Transient gastric stasis was observed in 18.2% of cases and resolved with conservative management. One postoperative mortality was attributed to pulmonary infection. The median overall and disease-free survival were 25 months.
Conclusion:
Integrating EGIARADMT curvilinear stapling with OrVil-TriSAS anastomosis enables cervical incision-free R0 resection for CTJ-ESCC, achieving precise oncologic control with functional preservation. Adjuvant therapy may further improve survival despite clear margins.
Introduction
Despite a decline in the occurrence and death rates of esophageal cancer in China, the significant disease burden persists due to the country’s large population. In 2022, there were approximately 224,000 new cases and 187,500 deaths, underscoring the persistent challenges in combating this disease. 1 Surgical intervention remains the primary approach for curative management of resectable esophageal carcinoma. 2 Minimally invasive esophagectomy (MIE) for esophageal cancer has demonstrated lower postoperative complications compared with open esophagectomy, resulting in improved short-term health-related quality of life. 3
The surgical treatment of esophageal squamous cell carcinoma (ESCC) located at the cervicothoracic junction (CTJ-ESCC), situated approximately 18–21 cm from the incisors, poses unique challenges due to its proximity to critical anatomical structures, including the trachea and recurrent laryngeal nerves near the thoracic inlet. 4 The conventional approach, known as the McKeown esophagectomy, which entails cervical incisions, is associated with notable risks, such as anastomotic leakage (with an incidence ranging from 2.4% to 31.7%) and recurrent laryngeal nerve damage (up to 44.4%).5,6 Notably, McKeown’s esophagectomy has been identified as an independent predictor of combined postoperative morbidity and mortality. 7
In contrast, the minimally invasive Ivor-Lewis approach reduces complications such as anastomotic leakage and 90-day mortality rates.8–10 The integrated approach utilizes curvilinear stapling (EGIARADMT™) and OrVil™ three-dimensional suspension anastomosis (OrVil-TriSAS), known as Chai’s Supra-Thoracic Apex (CSTA) technique, to enable non-transected tubular gastric reconstruction with R0 resection margins. This technique facilitates complete intrathoracic esophageal dissection without cervical incisions. This study aims to evaluate the efficacy and safety of the CSTA technique in a cohort of patients with CTJ-ESCC treated between 2019 and 2024.
Materials and Methods
Study design
This retrospective cohort study examined 11 patients diagnosed with CTJ-ESCC who underwent surgical intervention between February 2019 and March 2024, with follow-up completed by February 2025. Inclusion criteria stipulated that the upper margins of the tumor were situated 18–21 cm from the incisors. Within the cohort, 63.6% of patients (n = 7) chose not to undergo neoadjuvant therapy and proceeded directly to surgery. Conversely, 1 patient was ineligible for neoadjuvant therapy due to hypersplenism. This two-center study comprised 11 consecutive patients with CTJ-ESCC: 10 patients were managed at the Department of Thoracic Surgery, North District, First Affiliated Hospital of Anhui Medical University (Anhui Provincial Clinical Center for Public Health) in Hefei, China, while 1 patient was treated at the Department of Thoracic Surgery, Nanjing Lishui People’s Hospital, Zhongda Hospital Lishui Branch, Southeast University in Nanjing, China.
Surgical technique
Preoperative assessment, anesthetic protocol, and incisional strategy
Preoperative assessments involved comprehensive staging modalities, such as endoscopy, chest CT scans, and abdominal CT scans with both oral and intravenous contrast. The diagnosis was confirmed via gastroscopy and biopsy before surgery, with preoperative assessments verifying the absence of distant metastases. A standardized anesthesia protocol was implemented, and a thoracoabdominal incision was performed according to the method described by Cao et al. 11
Laparoscopic dissection and lymphadenectomy technique
In laparoscopic surgeries, certain patients exhibited adhesions impacting various anatomical locations. Meticulous dissection of posterior adhesions along the greater curvature and pancreas was undertaken before addressing the lesser curvature to prevent thermal injury to the pancreas and colonic flexures when utilizing energy devices such as ultrasonic shears and LigaSure™.
Abdominal vascular control and lymphadenectomy
The left gastric artery was securely ligated distally using a large Hemolock™ clip, supplemented by LigaSure thermal sealing to prevent postoperative hemorrhage. The preservation of the vascular arcade along the greater curvature was meticulously maintained. A systematic three-phase lymphadenectomy was conducted: (1) targeting perigastric stations around the left gastric and splenic arteries; (2) addressing stations at the hepatoduodenal ligament and common hepatic artery; and (3) focusing on stations around the celiac axis. This sequential approach, performed after gastric mobilization and displacement to the right, improved visibility and facilitated en bloc resection of lymph nodes in the hepatic and celiac regions.
Esophageal dissection and vascular management
Esophageal dissection extended from the hiatus to the azygos vein arch along the spinal border. Three esophageal arteries and two bronchial arteries arising from the proximal descending aorta were identified, ligated at their origins using medium-sized Hemolock clips, and then transected distally with an ultrasonic scalpel to reduce the risk of hemorrhage. 12 A hybrid dissection approach, utilizing a combination of blunt dissection and energy devices (such as an ultrasonic scalpel or LigaSure) under dual-channel suction guidance, was employed to precisely mobilize the esophagus near the azygos arch while safeguarding these venous structures.
Tumor resection and bronchial involvement
In instances of tumor infiltration into the left main bronchus, meticulous dissection at a millimeter scale was conducted employing the “longitudinal axis traction principle,” aided by dual suction devices and an ultrasonic scalpel. This technique, completed in under 20 minutes, led to a thorough R0 resection at a macroscopic level, minimizing the likelihood of tracheal membrane injury or tracheopleural fistula formation.
Cervical-sparing esophagectomy: Integrated EGIARADMT-OrVil TriSAS platform for R0 resection
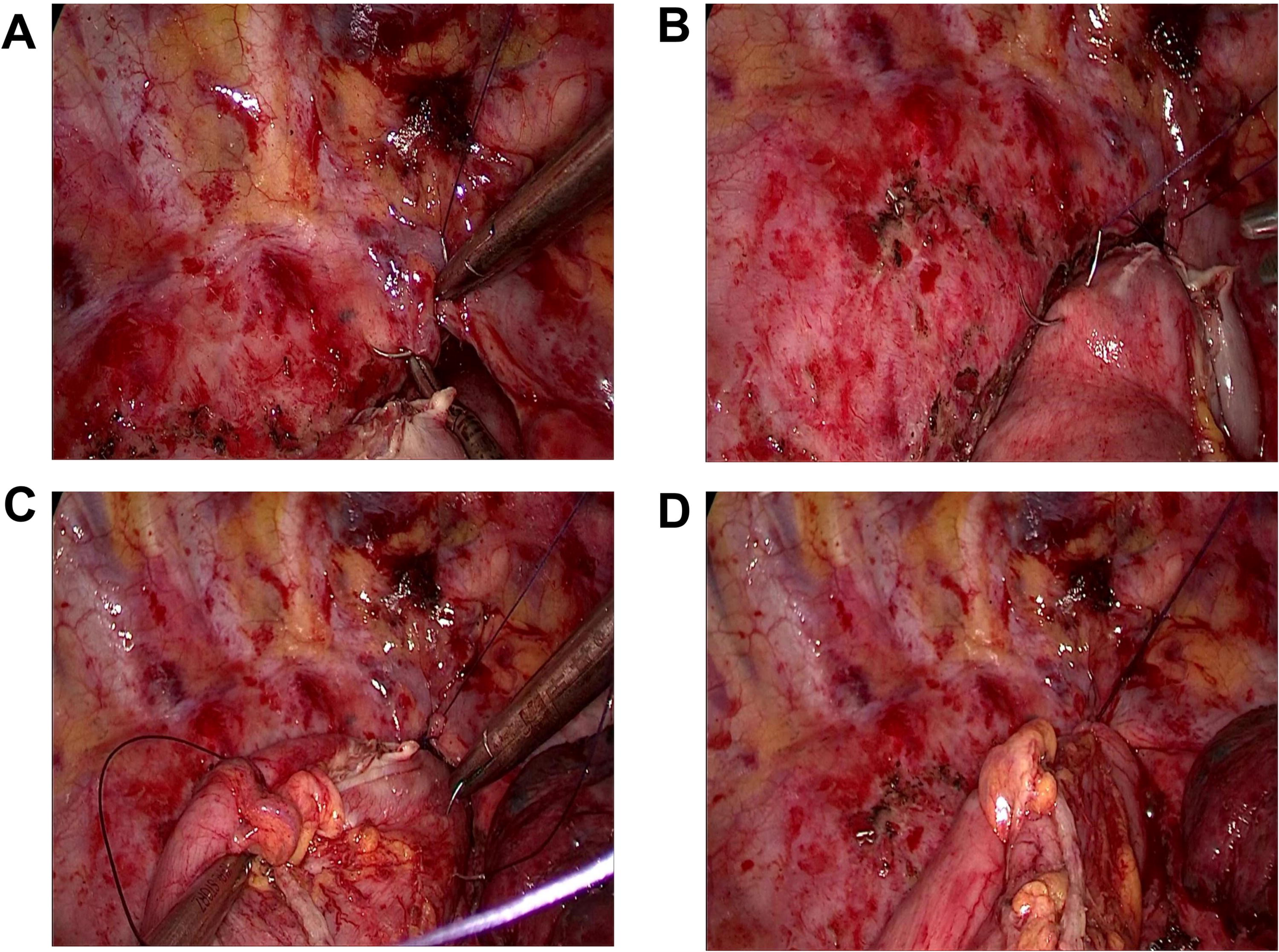
Cervical esophagus mobilization was performed up to the thyroid cartilage level using a hybrid dissection technique, retracting it at least 4 cm into the right thoracic cavity, shown in Figure 1A and B. Prophylactic ligation of the thoracic duct was carried out in 1 patient to prevent postoperative chylothorax. Thoracoscopic methods enabled the accurate excision of enlarged lymph nodes near the right inferior pulmonary ligament, paraesophageal region, subcarinal area, station 4R, and bilateral recurrent laryngeal nerves, ensuring thorough nodal dissection.

The movement of the cervical esophagus into the thoracic cavity, the use of a curved endoscopic stapler (EGIARADMT), and the transection of the esophagus at the thoracic inlet after retraction into the thoracic cavity. Panel
Cervical esophageal transection was conducted at the thoracic inlet, 1–4 cm proximal to the tumor, using a curved endoscopic stapler (EGIARADMT) to ensure clear margins, shown in Figure 1C and D. Due to the tumor’s superior location, the OrVil device (EEAORVIL25A; Covidien) anvil head was positioned at the proximal esophageal stump following the technique outlined by Zhang et al. 13 The stomach was transected just below the esophagogastric junction. Subsequently, the OrVIL circular stapler was inserted through the gastrotomy site created below the cardia for esophagogastric anastomosis at the right thoracic apex. The subcardiac gastric stump was closed using an EndoGIA™ stapler (3.5 mm blue cartridge).
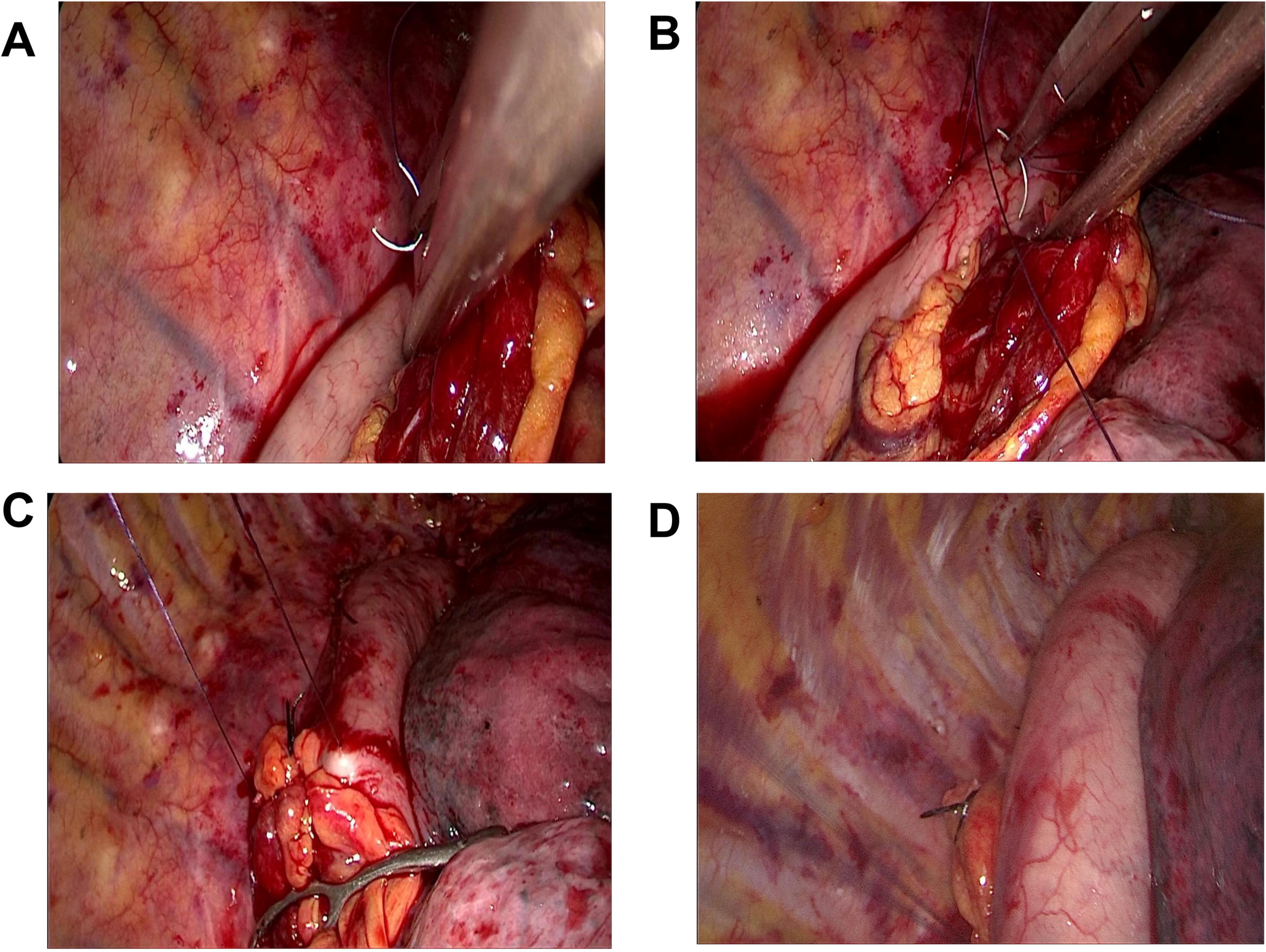
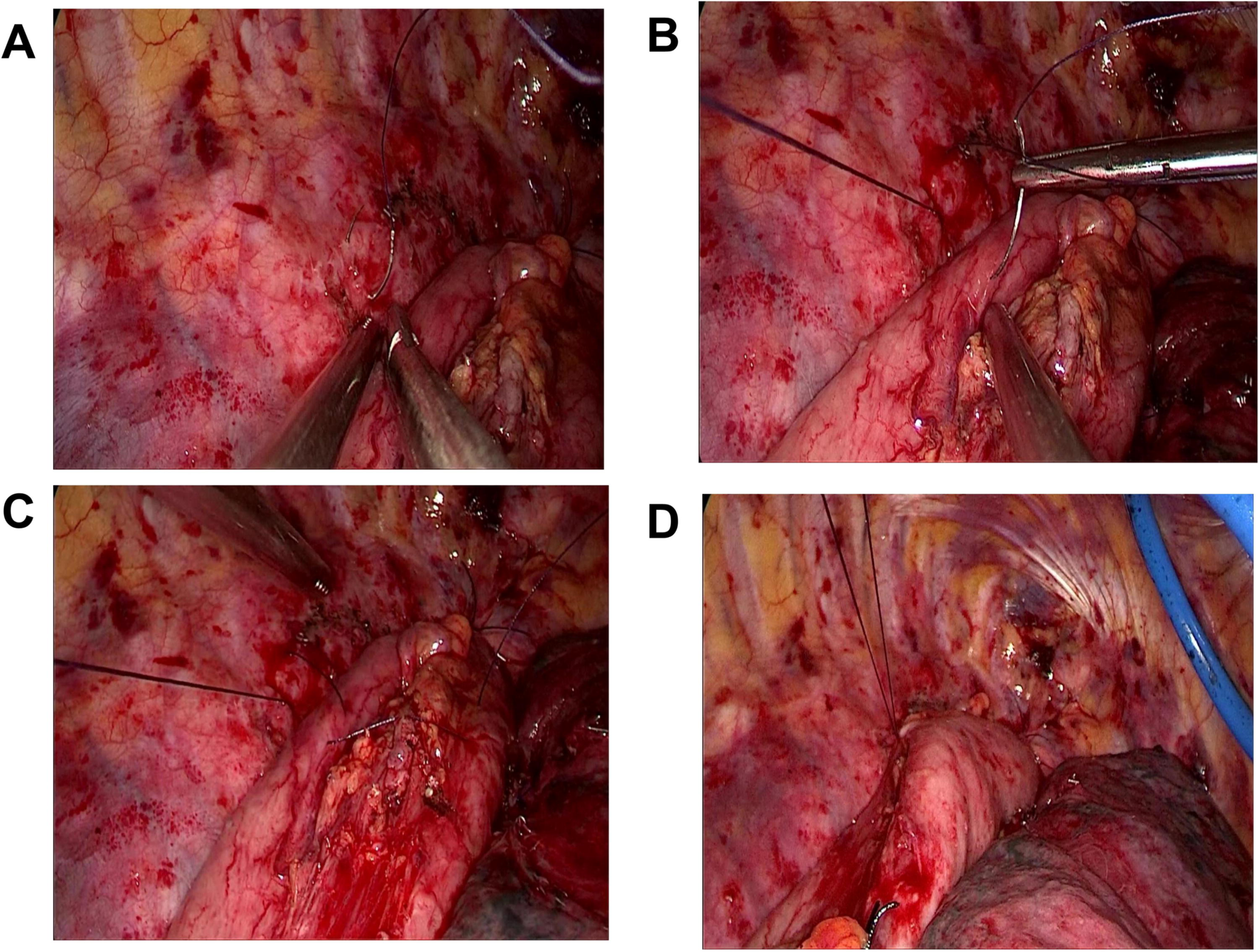
To mitigate anastomotic tension and reflux, a triple-point suspension technique was implemented, as shown in Figures 2–5. This technique comprised three primary steps: (1) securing the gastric fundus to the apical pleura with two 8-strand polypropylene seromuscular sutures to establish a triangular knotting system akin to the His angle; (2) transforming the stomach into a “mini flare” shape characterized by fundus constriction and body expansion to generate an anti-reflux pressure gradient; and (3) utilizing a modified chest wall fixation approach involving a small-angle fishhook-shaped needle to maintain a 2 cm elevation disparity between the gastric conduit and the chest wall, leading to a 30-minute prolongation of the surgical duration. A non-cutting gastric conduit, 4–5 cm in width, was fashioned without a longitudinal incision, following the methodology outlined by Sheng et al. 14
The initial three-point suspension technique. In panel
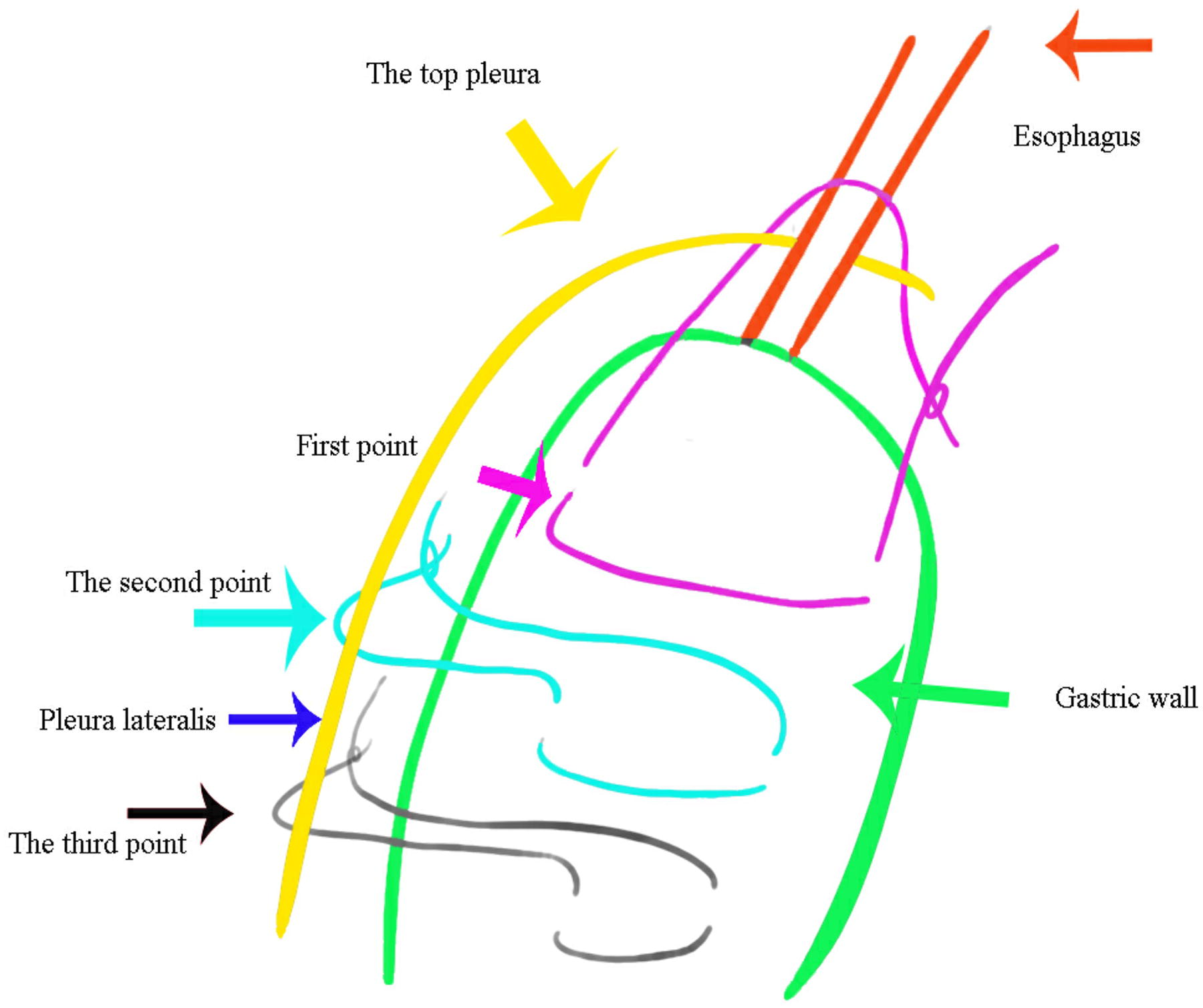
Aa detailed schematic of the three-point suspension system based on the work of Sheng et al. 14 The figure shows the main fixation point at the cupula of the pleura (purple arrow), the secondary suspension of the gastric body (dark green arrow), and the tertiary stabilization of the greater curvature (black arrow).
Hypersplenism management
A laparoscopic splenectomy was performed on a patient with hypersplenism, following the protocol described by Sheng et al. 14
Postoperative management
Following the surgery, no signs of active bleeding were observed at the esophageal bed or carina. Two pulmonary parenchymal injuries in the right upper and lower lobes were meticulously repaired using 3-0 continuous polypropylene sutures. Given the prolonged surgical duration and the inherent risk of recurrent laryngeal nerve injury, prophylactic tracheostomy was routinely performed in most cases after obtaining informed consent. 15 This approach mitigated risks from prolonged operations and potential laryngeal nerve injury. Subsequently, the patient was closely monitored in the intensive care unit and mechanically ventilated. The patient opted out of recommended adjuvant therapies, and consequently, no further such interventions.
Statistical analysis
Descriptive statistics were computed using SPSS version 22 (IBM Corp., Armonk, NY, USA). Normally distributed continuous variables were summarized as mean ± standard deviation, while non-normally distributed variables were presented as median (range). Categorical variables were reported as counts and percentages [n (%)]. Kaplan–Meier analysis was employed to assess overall survival (OS) and disease-free survival (DFS) rates.
Ethics approval
Approval for the study was granted by the Institutional Review Board of the Anhui Provincial Public Health Clinical Centre (North District, First Affiliated Hospital of Anhui Medical University) under Approval No. PJYX2025011.
Results
Preoperative patient characteristics
The median age of the study cohort was 72 years, with 54.5% being male. The patients had proximal esophageal tumors consistently situated 18–21 cm from the incisors. Common comorbidities included hypertension (18.2%), diabetes mellitus (9.1%), and a history of tobacco/alcohol use (45.5%). It is noteworthy that none of the patients had chronic pulmonary disease, and there were no documented cases of Chronic Obstructive Pulmonary Disease (Table 1).
Baseline Clinical and Pathological Characteristics (N = 11)
AJCC, American Joint Committee on Cancer; BMI, body mass index; COPD, Chronic Obstructive Pulmonary Disease; ICU, intensive care unit.
Perioperative outcomes
Surgical procedures had a median operative duration of 350 minutes (range 275–605) with minimal blood loss (median 100 mL). All cases achieved histologically confirmed R0 resection, maintaining proximal margins of 1–4 cm through hybrid dissection techniques.
The median hospital stay of 49 days primarily resulted from extensive preoperative preparation, with a median duration of 11 days for advanced disease management. Prophylactic tracheostomy was employed in 81.8% (9/11) of cases, while 1 patient (9.1%) required an unplanned tracheostomy due to refractory respiratory failure. Postoperative complications were limited to self-resolving gastric stasis in 18.2% of cases, which were effectively managed conservatively without the need for surgical intervention.16,17 There were no instances of anastomotic complications such as leaks or strictures, nor were there any occurrences of recurrent laryngeal nerve dysfunction following the surgery (Table 1).
Median tumor length was 4.5 cm (range 2.0–6.0 cm). Histopathological analysis revealed predominantly moderately differentiated tumors (81.8%), with equal distribution of well-differentiated (9.1%) and poorly differentiated (9.1%) subtypes. According to American Joint Committee on Cancer staging, a majority of cases exhibited advanced local disease (63.6% T3). 18 Lymph node dissection revealed a median of 21 nodes per case (range: 9–38), with 72.7% categorized as N0 and 27.3% as N1. The final pathological staging predominantly classified patients as stage IIB (36.4%) or IIIB (18.2%) (Table 1).
One patient succumbed on postoperative day 21 secondary to withdrawal of life-sustaining treatment following refractory pneumonia precipitating respiratory failure. Kaplan–Meier analysis revealed median OS and DFS of 25 months, as presented in Supplementary Table S1. Survival probabilities exhibited a gradual decline from the initial rates of 91% for OS and 100% for DFS to 53% and 75%, respectively, at 19 months, after which they remained relatively stable throughout the 25-month observation period.
Discussion
Background and objectives
This research assesses a new surgical technique for treating CTJ-ESCC by retrospectively analyzing 11 patients with tumors positioned 18–21 cm from the incisors. Our results highlight the delicate interplay among technical advancements, oncological accuracy, and systemic treatment hurdles in addressing this intricate cancer. The outcomes indicate that contemporary stapling methods facilitate achieving R0 resection via a thoracic-exclusive strategy, successfully circumventing cervical complications—a noteworthy progress considering that 81.8% of patients received surgery as the monotherapy. 19
Technical innovations and anatomical precision
The integration of the EGIARADMT endoscopic stapling system and OrVil TriSAS platform enabled en bloc resection through exclusive thoracic access, achieved through three pivotal advancements:
The 60-mm curved EGIARADMT stapler with 135° bidirectional articulation enabled precise esophageal transection below the thoracic inlet, overcoming spatial limitations that previously contraindicated thoracoscopic resection for tumors <22 cm from incisors.
20
This innovative system ensured the preservation of ideal esophageal axis alignment during the traversal of constricted mediastinal spaces.
End-to-side anastomotic integrity was effectively achieved by the EEA OrVil circular stapler due to its unique curved handle design and progressive compression mechanism, resulting in enhanced leak resistance in comparison to traditional systems.
13
Our three-point suspension technique preserved physiological anatomy through:
Fundal preservation: Reduced postoperative reflux incidence Force distribution: Minimized axial traction via multidirectional load sharing Vascular preservation: Maintained submucosal perfusion networks (Indocyanine Green angiography-confirmed)
21
Clinical implementation and oncological outcomes
Due to the intricate anatomy of the CTJ and the elevated risk of recurrent laryngeal nerve injury, 22 prophylactic tracheostomy was performed in 81.8% (9/11) of cases.
Transient gastric stasis, affecting 18.2% (2 out of 11) of cases, was likely due to vagal denervation, 23 resolving spontaneously within 28 days after surgery. This finding suggests that routine pyloroplasty may not be required during gastric conduit preservation. 24
All patients achieved R0 resection with a median proximal margin of 3 cm (range: 1.0–4.0 cm), pathologically confirmed through serial 3-mm sections. Systematic lymphadenectomy yielded a median of 21 nodes (range: 9–38), surpassing National Comprehensive Cancer Network quality benchmarks. 18 Notably, no anastomotic complications (leakage/stricture) or neurological sequelae were observed during follow-up.
Comparative surgical outcomes
T-shaped anastomosis: Mandated ≥19.5 cm or 21cm proximal tumor margin from incisors for 45 or 60 mm stapler deployment.
26
Critical observation
Notably, the sole mortality linked to respiratory failure (9.1%) highlights the heightened vulnerability of this demographic to pulmonary issues, underscoring the necessity for improved perioperative respiratory protocols. 27
Survival analysis and therapeutic implications
In the CTJ-ESCC cohort comprising 11 individuals, 72.8% (8/11) underwent initial resection, with one case being ineligible for neoadjuvant treatment due to hypersplenism. These patients achieved comparable outcomes: median OS and DFS were both 25 months. Notably, 63.6% (7/11) presented with advanced T3-stage disease. Analysis of survival curves revealed distinct trends: OS rates decreased from 91% at baseline to 53% at 19 months before stabilizing until 25 months, while DFS rates remained at 100% until 11 months, subsequently dropping to 88% at 11 months and 75% at 19 months before stabilizing. The observed 11-month survival gap (DFS 88% versus OS 70%) indicates a higher incidence of recurrence or disease progression preceding delayed mortality events.
Comparative survival analysis
Our findings are consistent with two distinct reference points:
In surgical cohorts of pT3 ESCC, the 2-year OS rate was 72.8%, accompanied by a DFS rate of 69.4%.
28
Trials focusing on adenocarcinoma as the predominant histology reported a 24-month OS in the surgery-alone arm of the ChemoRadiotherapy for Oesophageal cancer followed by Surgery Study trial, with histological distribution as follows: 75% adenocarcinoma, 23% squamous cell carcinoma, and 2% large cell undifferentiated carcinoma.
29
Critical surgical-pathological findings
All R0 resections, with margins ranging from 1 to 4 cm, did not achieve the recommended threshold of >5 cm for T3 disease, 30 which may help explain the observed recurrence patterns. The insufficient margin width highlights the need for more aggressive adjuvant strategies in both treatment-naïve (81.8%) and neoadjuvant-exposed subgroups. 27
Translational implications
The evolving treatment approach presents two key optimization strategies:
Perioperative immunotherapy: Building upon the favorable outcomes demonstrated of KEYNOTE-590 in unresectable advanced ESCC (median OS 13.9 versus 8.8 months for PD-L1 CPS ≥10; hazard ratio [HR] 0.57, P < .0001) 31 and the DFS advantage observed in resected disease in the CheckMate 577 trial (HR 0.69, encompassing mixed histology). 32
Limitations
This study is limited by its retrospective design, particularly due to a small sample size (n = 11), which reduces statistical power and generalizability. The lack of neoadjuvant therapy in most cases adds to data variability. Utilizing archival records may introduce selection and recall biases, potentially affecting data precision.
Future directions
Future multicenter prospective studies should be conducted to compare cervical incision with incision-free thoracic surgery for CTJ-ESCC. Additionally, investigations comparing neoadjuvant therapy plus surgery versus surgery alone, and surgery alone versus postoperative adjuvant therapy, could help overcome these limitations. Stratifying patients based on biomarkers, particularly leveraging the consistent PD-L1 expression patterns observed across different disease stages, could offer valuable guidance for sequencing immune-chemotherapy treatments.
Conclusion
CSTA technique enables transcervical-avoidant R0 resection for CTJ-ESCC, achieving precision oncologic control while preserving functional anatomy. Although R0 margins were consistently achieved, the implementation of adjuvant therapy and improved critical care strategies may enhance long-term survival outcomes, especially in cases of node-positive disease.
The third suspension, which involves a three-point suspension and an intact tubular stomach postprocedure. Panel
The second phase of the three-point suspension technique. In panel
Footnotes
Acknowledgments
The authors would like to acknowledge the surgical, anesthesia, and nursing teams for their valuable contributions. They extend special gratitude to Dr. Hui-Kang Zhang from the Department of Orthopedics at Nanjing First Hospital for his guidance in employing artificial intelligence to enhance academic articles.
Authors’ Contributions
W.Z.: Investigation (lead), data curation (equal), and writing—original draft (supporting). Y.S.: Formal analysis, visualization (lead), and methodology (supporting). S.Y.: Conceptualization (lead), supervision (lead), project administration (lead), and writing—review and editing (equal). C.Z.: Data curation, investigation (equal), and software (supporting). H.C.: Resources (lead), conceptualization (supporting), and supervision (supporting). F.L.: Methodology and formal analysis (supporting). S.Z.: Validation and visualization (supporting). W.D.: Data curation. All authors: Writing—review and editing (equal).
Data Availability
Data is available upon request.
Disclosure Statement
The co-author “Yaoyao” has been removed from the author list at her request. All authors confirm they have no personal interests related to this article and declare “no conflicts of interest to disclose.” No competing financial interests exist.
Funding Information
No funding was received for this article.