
Abstract
Background:
Incidental gallbladder cancer (IGBC) is often diagnosed unexpectedly during or after cholecystectomy performed for presumed benign gallbladder disease. Accurate preoperative prediction of lymph node (LN) metastasis is critical for guiding surgical re-resection strategies but remains challenging. This study aimed to develop and validate a nomogram to predict LN metastasis in IGBC patients prior to re-resection.
Methods:
We retrospectively analyzed 745 IGBC patients who underwent re-resection between August 2019 and October 2024. Clinical data, including demographics, comorbidities, laboratory tests, imaging findings, and histopathological features, were collected. Univariate and multivariate logistic regression analyses were performed to identify independent risk factors for LN metastasis. A nomogram was constructed based on these factors. The predictive performance of the nomogram was evaluated using receiver operating characteristic (ROC) curve analysis, calibration plots, and decision curve analysis (DCA).
Results:
Multivariate analysis identified tumor size > 1 cm, advanced T stage, poor differentiation, positive LN status on preoperative computed tomography imaging, and elevated serum levels of carcinoembryonic antigen and carbohydrate antigen 19-9 as independent predictors of LN metastasis. The nomogram demonstrated good discriminative ability, with an area under the ROC curve (AUC) of 0.827. Calibration plots showed good agreement between predicted probabilities and observed outcomes. DCA indicated the clinical usefulness of the nomogram.
Conclusions:
The nomogram based on preoperative clinical, imaging, and pathological factors provides an effective tool for predicting LN metastasis in IGBC patients before re-resection. It can assist clinicians in risk stratification and optimizing surgical strategies, potentially improving patient outcomes.
Introduction
Gallbladder cancer (GBC) is a rare but highly aggressive malignancy, often diagnosed at an advanced stage due to its asymptomatic nature in early development and the lack of effective screening methods. 1 A significant proportion of GBC cases are discovered incidentally during or after cholecystectomy performed for presumed benign gallbladder diseases, such as gallstones or cholecystitis. 2 These incidental GBCs (IGBCs) present a unique clinical challenge regarding diagnosis, staging, and management.
Lymph node (LN) metastasis is a critical prognostic factor in GBC, significantly impacting disease staging and overall survival outcomes. 3 Accurate assessment of LN status is essential for guiding surgical decision-making, including the necessity for extended re-resection and lymphadenectomy. 4 However, predicting LN involvement preoperatively in patients with IGBC remains challenging due to the limitations of current diagnostic modalities and nonspecific clinical presentations.
In this study, we aimed to develop and validate a nomogram to predict the risk of LN metastasis in patients with IGBC before re-resection.
Materials and Methods
Patients
This retrospective study included patients who were diagnosed with incidental GBC and underwent surgical treatment at First Central Hospital of Baoding between August 2019 and October 2024. The inclusion criteria were (1) patients aged 18 years or older; (2) underwent re-resection for incidental GBC; and (3) had complete clinical and operative data available. Exclusion criteria included (1) patients with preoperatively diagnosed GBC; (2) those who received neoadjuvant therapy; (3) severe comorbidities contraindicating surgery; (4) presence of distant metastasis at the time of initial surgery; and (5) incomplete medical records.
The study was approved by the Institutional Review Board of First Central Hospital of Baoding, and the requirement for informed consent was waived due to the retrospective nature of the study.
Data collection
Clinical, laboratory, imaging, and histopathological data were retrospectively collected from the electronic medical records of all patients included in the study. Demographic information recorded for each patient included age, sex, body mass index (BMI), and American Society of Anesthesiologists (ASA) physical status classification. Comorbid conditions such as hypertension and diabetes mellitus were documented, along with the presence of gallstones, cholecystitis, and jaundice.
Preoperative laboratory evaluations encompassed measurements of white blood cell (WBC) counts and levels of tumor markers, including carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and carbohydrate antigen 125 (CA125). These laboratory parameters provided insights into the patients’ baseline hematological status and potential indicators of malignancy.
Imaging data were obtained from preoperative computed tomography (CT) scans. CT reports were reviewed to assess LN status, with LNs classified as positive or negative for metastatic involvement based on radiographical criteria.
Histopathological data were extracted from the pathology reports of resected specimens. Tumor size was measured and categorized as ≤1 cm or >1 cm. The pathological T stage was determined according to the American Joint Committee on Cancer (AJCC) staging system, with tumors classified as T1a, T1b, or T2. Tumor differentiation was assessed and categorized as well-differentiated, moderately differentiated, or poorly differentiated.
All collected data were reviewed and verified by two independent researchers to ensure accuracy and completeness. Discrepancies were resolved through discussion or consultation with a third researcher. The comprehensive dataset facilitated a thorough analysis of potential risk factors associated with LN metastasis in patients with incidental GBC.
Statistical analysis
Statistical analyses were conducted using GraphPad Prism 8.0 (GraphPad Inc., CA, USA) and IBM SPSS Statistics 23.0 (IBM Corp., Armonk, NY, USA). Results are reported as mean ± standard deviation or in terms of counts and percentages (n, %). Depending on the nature of the data, appropriate statistical tests such as the chi-square test, Student’s t-test, or Mann–Whitney U test were utilized. Receiver operating characteristic (ROC) curve analyses were applied to evaluate the predictive ability of continuous variables for postoperative weight regain and to determine optimal cutoff values. Risk factors for weight regain were examined through binary univariate and multivariate logistic regression analyses using the “Enter” method. A nomogram incorporating the identified risk factors was developed and assessed using R software (version 4.0.1) with the “rms” package. Significance was determined at a P value less than .05.
Results
Patient characteristics
A total of 745 patients with incidental GBC were included in the study, comprising 405 males (54.4%) and 340 females (45.6%), with a mean age of 59.5 ± 8.5 years. The majority of patients were classified as ASA II (51.7%), followed by ASA I (31.2%) and ASA III (17.1%). The mean BMI was 24.6 ± 3.1 kg/m2. Comorbid conditions included hypertension in 250 patients (33.6%) and diabetes mellitus in 130 patients (17.4%). Gallstones were present in 205 patients (27.5%), and cholecystitis was observed in 285 patients (38.3%). Jaundice was present in 45 patients (6.0%).
Preoperative laboratory tests showed mean WBC counts of 6.55 ± 1.45 × 109/L. Elevated levels of tumor markers were noted in some patients: 55 patients (7.4%) had elevated CEA, 95 patients (12.8%) had elevated CA19-9, and 45 patients (6.0%) had elevated CA125. On preoperative CT imaging, positive LN status was reported in 545 patients (73.2%).
Histopathological examination revealed that 400 patients (53.7%) had tumors ≤1 cm in size, while 345 patients (46.3%) had tumors >1 cm. The distribution of T stages was as follows: T1a in 260 patients (34.9%), T1b in 300 patients (40.3%), and T2 in 185 patients (24.8%). Tumor differentiation was categorized as well-differentiated in 430 patients (57.7%), moderately differentiated in 245 patients (32.9%), and poorly differentiated in 70 patients (9.4%).
Univariate analysis of risk factors for LN metastasis
LN metastasis was identified in 265 patients (35.6%). Univariate logistic regression analysis indicated that elevated levels of CEA (P = .031), CA19-9 (P < .001), and CA125 (P = .045) were significantly associated with LN metastasis (Table 1). Tumor size >1 cm was correlated with a higher risk of LN involvement compared to tumors ≤1 cm (62.3% versus 37.7%, P = .033). Advanced T stage was significantly associated with increased LN metastasis (P < .001). Poor differentiation was also linked to a higher incidence of LN metastasis (P = .012). In addition, patients with positive CT-reported LN status had a greater likelihood of LN metastasis (P = .017).
Univariate Logistic Regression Analysis of Risk Factors for Lymph Node Metastasis
ASA, American Society of Anesthesiologists; BMI, body mass index; CEA, Carcinoembryonic Antigen CA199, Carbohydrate Antigen199; CA125, Carbohydrate Antigen 125; WBC, white blood cell.
Other factors such as age, sex, ASA classification, BMI, hypertension, diabetes, gallstones, WBC count, cholecystitis, and jaundice were not significantly associated with LN metastasis (P > .05 for all).
Multivariate analysis of risk factors for LN metastasis
Multivariate logistic regression analysis identified six independent risk factors for LN metastasis (Table 2, Fig. 1):

The forest plot of multivariate logistic regression analysis for lymph node metastasis.
Multivariate Logistic Regression Analysis of Risk Factors for Lymph Node Metastasis
CT, computed tomography; LN, lymph node.
Tumor size >1 cm: patients with tumors larger than 1 cm had a significantly higher risk (odds ratio [OR] = 5.55; 95% confidence interval [CI]: 1.60–10.12; P = .004). Advanced T Stage: higher T stages were associated with increased risk (OR = 3.95; 95% CI: 1.55–7.55; P = .005). Poor Differentiation: Poorly differentiated tumors were linked to a higher risk (OR = 5.05; 95% CI: 1.50–9.80; P = .026). Negative CT-Reported LN Status: positive LN findings on CT were associated with increased metastasis risk (OR = 2.55; 95% CI: 1.85–5.45; P = .031). Elevated CEA Levels: elevated preoperative CEA levels were a significant risk factor (OR = 6.04; 95% CI: 2.80–9.10; P = .002). Elevated CA19-9 Levels: elevated CA19-9 levels were strongly associated with LN metastasis (OR = 8.27; 95% CI: 3.40–15.50; P = .016).
Development of the nomogram
Based on the identified independent risk factors, a nomogram was constructed to predict the probability of LN metastasis in patients with incidental GBC before re-resection (Fig. 2). Each predictor was assigned a score proportional to its regression coefficient from the multivariate model. The sum of the scores corresponded to an individual patient’s risk of LN metastasis.
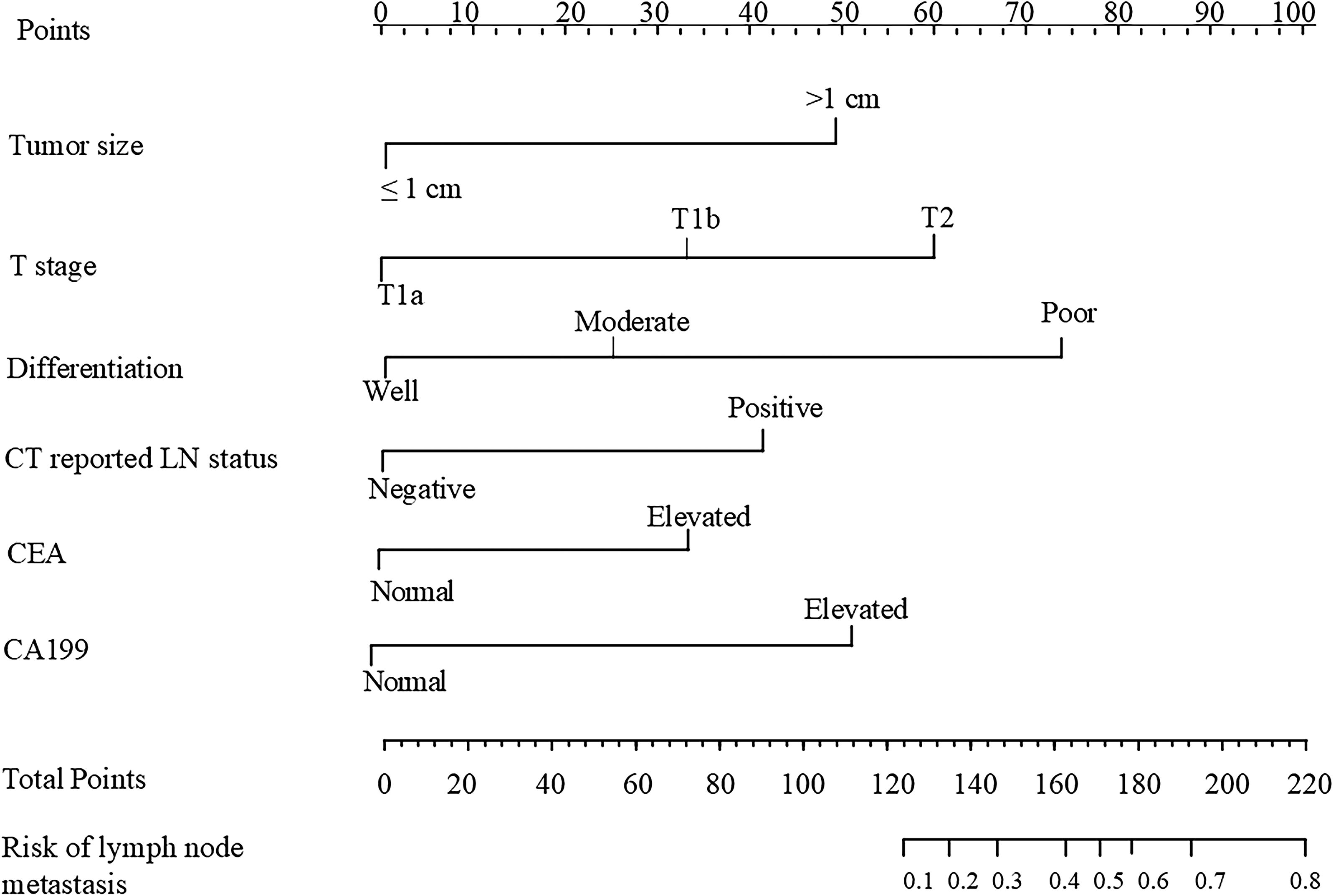
Nomogram for predicting the risk of lymph node metastasis in incidental gallbladder cancer before re-resection.
Validation of the nomogram
The predictive performance of the nomogram was evaluated using ROC curve analysis (Fig. 3). The nomogram demonstrated good discrimination ability for predicting LN metastasis. Calibration plots showed good agreement between the predicted probabilities and the actual observed outcomes (Fig. 4), indicating that the nomogram was well-calibrated. Decision curve analysis demonstrated that the nomogram provided a net clinical benefit across a range of threshold probabilities for LN metastasis (Fig. 5), suggesting its potential utility in clinical decision-making.

Receiver operating characteristic (ROC) curve for the nomogram. ROC, receiver operating characteristic.

Calibration plot for the nomogram.

Decision curve analysis (DCA) for the nomogram. DCA, decision curve analysis.
Discussion
In this study, we developed and validated a nomogram to predict the risk of LN metastasis in patients with IGBC prior to re-resection. By integrating six independent risk factors—tumor size >1 cm, advanced T stage, poor tumor differentiation, negative LN status on preoperative CT imaging, and elevated serum levels of CEA and CA19-9—our nomogram demonstrated robust predictive performance. The area under the ROC curve indicated excellent discrimination, while calibration plots showed good agreement between predicted and observed outcomes.
Our findings are consistent with previous studies emphasizing the importance of LN metastasis as a critical prognostic factor in GBC. Several studies have demonstrated that LN involvement significantly impacts overall survival and recurrence rates in GBC patients.5–7 Accurate preoperative prediction of LN status remains challenging due to the limitations of imaging modalities and the asymptomatic nature of early-stage disease.
The association between larger tumor size and increased risk of LN metastasis aligns with existing literature. Larger tumors are more likely to exhibit aggressive behavior and infiltrate lymphatic vessels.8,9 Similarly, advanced T stage, reflecting deeper invasion into the gallbladder wall, correlates with a higher likelihood of lymphatic spread.10,11 Poor tumor differentiation indicates a more aggressive histological phenotype, which is associated with increased metastatic potential.12,13
Positive LN status on preoperative CT imaging emerged as a significant predictor of LN metastasis in our study. Patients with LNs reported as positive on CT scans had a higher likelihood of pathological LN involvement than those with negative CT findings (OR = 2.55; 95% CI: 1.85–5.45; P = .031). This association underscores the utility of preoperative CT imaging in identifying patients at increased risk of lymphatic dissemination. Our findings are consistent with previous studies suggesting that enlarged or morphologically suspicious LNs on imaging are indicative of metastatic disease in GBC patients.5,14,15
The integration of CT-reported LN status into our nomogram enhances its clinical applicability. By combining imaging findings with other significant predictors, clinicians can better stratify patients based on their risk profiles. This is particularly relevant for IGBC patients, as the decision to pursue extended re-resection and lymphadenectomy depends heavily on the estimated likelihood of LN metastasis. Accurate preoperative assessment can thus optimize surgical planning and potentially improve patient outcomes.
Elevated serum levels of CEA and CA19-9 were significant predictors of LN metastasis in our cohort. These tumor markers are widely used in gastrointestinal malignancies, including pancreatic and colorectal cancers, as indicators of tumor burden and disease progression.16–18 In GBC, elevated CA19-9 levels have been associated with advanced disease stages and poorer prognoses. Our findings support the utility of these biomarkers in risk stratification and underscore their potential role in preoperative assessment.
Several studies have attempted to develop predictive models or nomograms for LN metastasis in GBC. For instance, Yang et al. developed a model incorporating factors such as tumor size, depth of invasion, and vascular invasion, demonstrating reasonable predictive accuracy. 19 However, most existing models are based on intraoperative or postoperative pathological findings, limiting their utility in preoperative planning. Our nomogram, based on preoperative clinical, laboratory, and imaging data, offers a practical tool for surgeons to identify high-risk patients prior to re-resection.
The clinical implications of our study are significant. Accurate prediction of LN metastasis can guide surgical decision-making, particularly regarding the extent of re-resection and lymphadenectomy. Current guidelines recommend extended cholecystectomy with regional lymphadenectomy for patients with T1b or higher-stage IGBC. However, the necessity and extent of lymphadenectomy remain subjects of debate due to the potential morbidity associated with more extensive surgeries. Our nomogram can assist in selecting patients who are more likely to benefit from aggressive surgical approaches.
There are limitations to our study that should be acknowledged. First, the retrospective design may introduce selection bias. Second, variations in imaging quality, interpretation, and laboratory assays could affect the applicability of the nomogram in other institutions. Third, while we included relevant and available preoperative variables, there may be other factors influencing LN metastasis that were not captured in our dataset, such as molecular or genetic markers. Future prospective, multicenter studies are needed to validate our nomogram and potentially incorporate additional predictive variables.
Conclusion
Our study provides a validated nomogram based on readily available preoperative variables to predict LN metastasis in IGBC patients. This tool can aid clinicians in preoperative risk stratification, surgical planning, and personalized patient management, potentially improving prognostic outcomes.
Footnotes
Acknowledgments
The authors thank the medical staff of our hospital for database management.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.