
Abstract
Background:
Hem-o-lok® clips (HOLC) (Weck Surgical Instruments, Teleflex Medical, Durham, NC) are commonly used to achieve athermal hemostasis and control the lateral vascular pedicles of the prostate, especially in nerve-sparing surgery during robot-assisted laparoscopic radical prostatectomy (RALP). However, an increasing number of studies have demonstrated intravesical HOLC migrations. This study aims to describe the clinical presentation, symptoms, management, and outcomes of intravesical HOLC migration to the vesicourethral anastomotic site (VUAS).
Methodology:
A retrospective analysis was conducted on 386 RALP procedures performed by an experienced surgeon at a tertiary care center between November 2017 and November 2024. The data of all patients who have experienced intravesical HOLC migration during long-term follow-up and were treated for this reason were compiled. Cystoscopy findings, HOLC localizations, the number of HOLCs removed, procedures, and patient follow-up data were analyzed.
Results:
Of 386 patients, 5 (1.2%) experienced intravesical HOLC migration at follow-up. Two of these patients received adjuvant radiotherapy. The mean time to identify HOLC migration was 27.8 ± 18.3 months. Following a single cystoscopic intervention, none of the patients’ HOLC migration-related symptoms recurred, and no further procedures were required. During follow-up, bladder neck stenosis occurred in 2 patients.
Conclusion:
In long-term follow-up of RALP, the lower urinary tract symptoms and persistent dysuria may be related to intravesical HOLC migration. In surgical practice, avoiding using HOLC close to the VUAS and reducing the number of HOLC utilized may help prevent complications.
Introduction
The advantages of robot-assisted laparoscopic radical prostatectomy (RALP) include relatively simple vesicourethral anastomosis, great exposure to the operating field, precise anatomical dissection, and a rapid recovery period following surgery. 1 However, RALP is associated with several postoperative morbidities, including de novo urinary incontinence, erectile dysfunction, urethral stricture, and vesicourethral anastomotic stenosis. 2 An uncommon and underreported morbidity in long-term follow-up is intravesical Hem-o-lok® clip (HOLC) (Weck Surgical Instruments, Teleflex Medical, Durham, NC) migration. The growing body of evidence shows that the incidence of this condition is increasing along with the global adoption of robotic systems and nerve-sparing surgical techniques.
Since their first introduction in 1999, HOLCs, made of a permanent, nonabsorbable, and nonconductive polymer, have been widely used in laparoscopic and robot-assisted laparoscopic surgery.3,4 It provides urologists with the additional benefits of simple ligation of vascular structures and prevention of thermal damage. However, due to their proximity to the vesicourethral anastomotic site (VUAS), these foreign bodies can migrate and settle at the anastomotic junction or into the bladder. HOLC migration can lead to various clinical scenarios such as hematuria, recurrent urinary tract infections, lower urinary tract symptoms, bladder stones, and bladder neck stenosis (BNS). 5
There are limited case series published in the literature, and there are no evidence-based recommendations in the guidelines on the classification and management of this condition. To contribute to accumulating knowledge in the literature, we aimed to share our experience and describe the clinical presentation, symptoms, management, and outcomes of intravesical HOLC migration following RALP based on data from a single high-volume tertiary care center.
Materials and Methods
All patients’ medical records of those who underwent RALP by the same experienced surgeon (B.O.) in our tertiary center between November 2017 and November 2024 were retrospectively analyzed. Demographic and clinical data of patients who experienced intravesical HOLC migration were compiled. Ethical approval for the study was granted by the institutional review board of Istanbul University-Cerrahpasa, Cerrahpasa Faculty of Medicine (Approval No: E-21263603-601.01-1095190). Informed consent was obtained from all patients prior to inclusion in the study.
The da Vinci Xi Surgical System (Intuitive Surgical, Sunnyvale, CA) was used in all operations. A standard approach of four 8-mm robotic reusable trocars and one 10-mm and one 5-mm assistant trocar were used. The vesicourethral anastomosis was carried out with a running 3-0 barbed V-LocTM suture (Covidien, Mansfield, MA) using the previously described technique by Van Velthoven et al. 6 Pelvic lymph node dissection was also performed in all patients with a 2018 Briganti nomogram of 7% or greater and those with a 2012 Briganti nomogram of 5% or greater.
Indwelling catheters of all patients were removed on the postoperative day 10. The patients were followed up at 3-month intervals for up to 2 years, followed by annual lifelong outpatient clinic controls. For up to 2 years, patients were monitored at 3-month intervals, followed by lifetime yearly outpatient clinic visits. Appropriate imaging was performed on patients who came repeatedly with atypical or prolonged complaints, such as hematuria, recurrent urinary tract infection, and persistent dysuria. Patients who showed signs of possible intravesical HOLC migration on imaging underwent cystoscopic examination. Cystoscopic evaluations of all patients were recorded on video and documented.
Results
Of 386 patients, 5 (1.2%) experienced intravesical HOLC migration at follow-up. None of these patients had any perioperative complications. Two patients received adjuvant radiotherapy combined with androgen deprivation therapy due to lymph node positivity in the final pathology. The characteristics of all patients with intravesical HOLC migration are summarized in Table 1.
Characteristics of 5 Patients with Intravesical Hem-o-Lok Clip Migration After Robot-Assisted Laparoscopic Radical Prostatectomy
ADT, androgen deprivation therapy; AJCC, American Joint Committee on Cancer; BNS, bladder neck stenosis; ISUP, International Society of Urological Pathology; PSA, prostate-specific antigen; VUAS, vesicourethral anastomotic site; TUI, transurethral incision.
The predominant symptoms in the patients were irritative lower urinary tract symptoms such as dysuria and hematuria, while 1 patient had spontaneous micturition of HOLC, and 1 patient had storage symptoms. The mean time to identify HOLC migration was 27.8 ± 18.3 months.
Patient 2 had a total of six clips on the VUAS. The noncalcified clips were removed with an endoscopic grasper, and coagulation was performed with bipolar energy. The patient was included in the urethral dilatation program, in which no recurrence was observed to prevent BNS. In Patient 4, the clip could be removed by transurethral resection as the clip was planted in the mucosa (Fig. 1). In the other three cases, the clips were calcified and were removed after holmium laser lithotripsy to avoid mucosal erosion during their removal (Fig. 2). Two patients with a history of adjuvant radiotherapy (Patients 3 and 5) also developed BNS on cystoscopy, which was resolved by transurethral incision and dilatation and did not recur during follow-up.

Cystoscopy image of Patient 4.
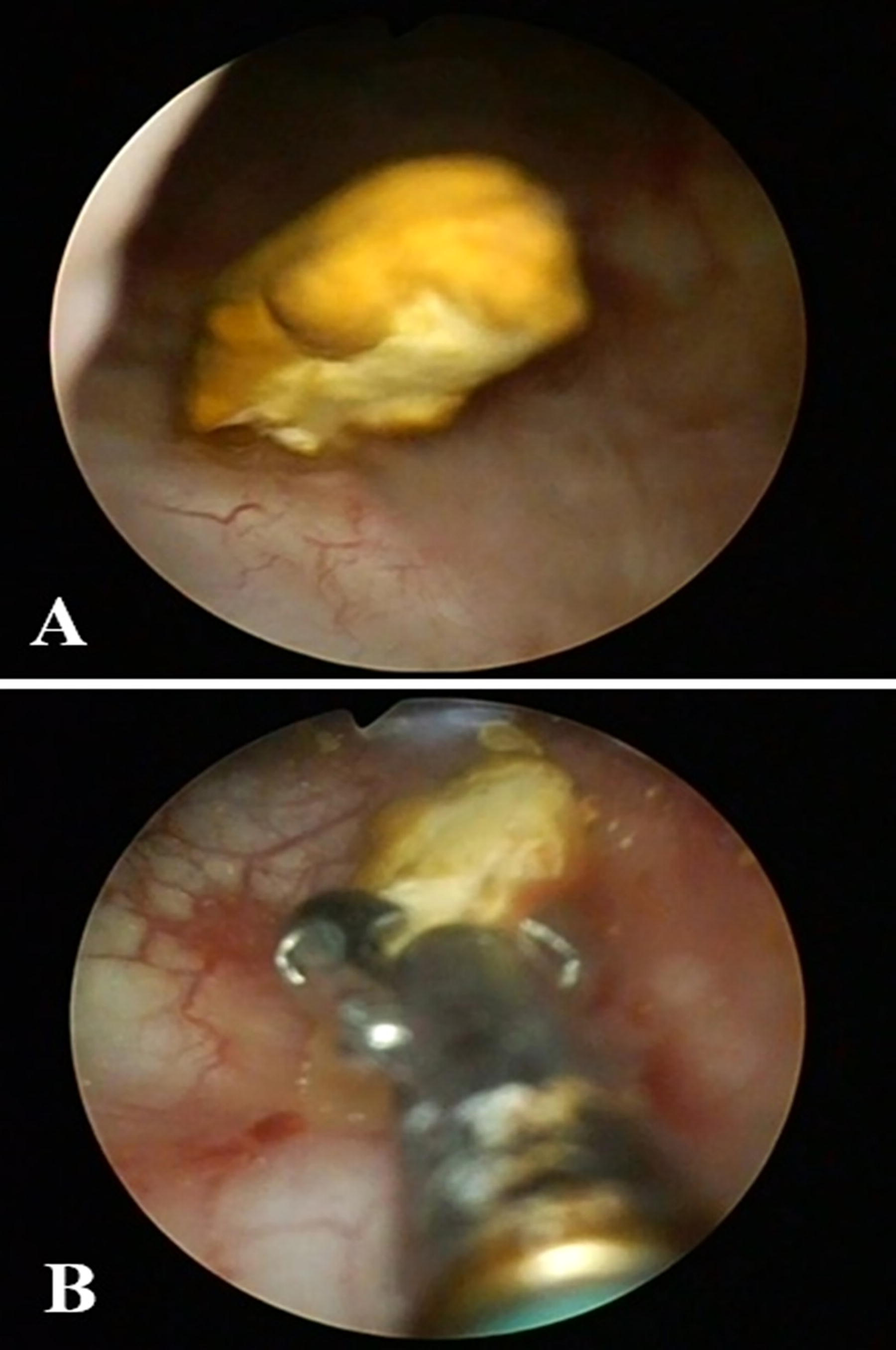
Cystoscopy image of Patient 1.
Indwelling catheters were removed on postoperative day 1 after cystoscopic interventions of all patients. Following the intervention, the patient’s symptoms disappeared promptly and did not recur. No patient required a repeat endoscopic procedure.
Discussion
HOLC clips have been widely utilized in RALP for vascular control due to their proven safety and effectiveness. They minimize the need for electrocautery and reduce the risk of neurovascular bundle injury while offering ease of application and secure clamping, especially in nerve-sparing surgical techniques. 7 Despite their reliable hemostatic properties, there have been reports of clip migration into the urinary tract, sometimes occurring years after surgery. 8 In our RALP cohort, conditions associated with intravesical HOLC migration were observed in 1.2% of patients undergoing RALP in a mean time of 27.8 ± 18.3 months, similar to the limited case series in the literature.
Several studies, mostly small case series, have documented instances of HOLC migration leading to complications such as urethral erosion, recurrent urinary tract infections, BNS, spontaneous expulsion, and bladder stone formation.7–16 The most frequently reported issues involve clip migration and BNS, both of which can be distressing for patients and may necessitate additional surgical intervention. However, HOLC migration into the lower urinary tract remains a relatively rare long-term complication of RALP, typically described in case reports and small case series. Considering the global adoption of robotic systems and the widespread use of HOLC in minimally invasive surgeries, it is conceivable that complications related to intravesical HOLC migration are likely to continue to be seen, and their incidence may be expected to increase. The management and prevention of this condition will be further improved with more material to be contributed to the literature.
In our case series, patients with intravesical HOLC migration presented with both irritative and obstructive lower urinary tract symptoms (LUTS). The development of new voiding symptoms in post-RALP patients should raise suspicion of potential clip-related issues. Nearly all clips were encrusted and located in the bladder trigone region. Each patient required a single intervention, with no recurrence of symptoms or additional procedures needed. Based on these findings, we recommend that surgeons avoid placing HOLC clips near the vesicourethral anastomosis and remove any loose clips at the end of the procedure to mitigate the risk of long-term complications.
Yu et al. classified HOLC migration into three categories based on the clinical presentation of their 6 patients
15
:
Type I: Erosion at the VUAS, causing LUTS. Type II: Erosion occurring further from the urethra at the reconstructed tennis racket closure site, leading to stone formation and hematuria without obstruction. Type III: Loose clips unintentionally drop into the bladder during surgery, leading to spontaneous expulsion in the weeks following the procedure.
Although there have not yet been enough cases reported in the literature to make a meta-analysis, classification, or evidence-based management scheme, we think that this long-term complication, which has an incidence ranging from 0.8% to 1.3% in the current case series, will be further investigated in the future.
BNS is one of the most complicated consequences of HOLC migration, though its precise etiology is poorly understood. While some cases of BNS have been linked to HOLC migration, most occur independently of it. The incidence of BNS following RALP ranges between 0.6% and 3%, which is lower compared to open prostatectomy. 2 Blumenthal et al. suggested that running an anastomosis may promote better mucosal edge approximation than a simple interrupted anastomosis, potentially reducing urethral distraction and expediting anastomotic healing. 10 Their study reported that 50% of their HOLC migration cases (2/4) developed BNS. Similarly, in our study, BNS was detected in 2 of our patients (40%) who received adjuvant radiotherapy and androgen deprivation treatment. The fact that it did not recur following clip removal suggests that this may be related to HOLC migration rather than a predisposition to fibrosis due to radiation-induced vasculopathy.
The precise mechanism of HOLC migration remains unclear, though the weaker tissue at the VUAS may predispose it to erosion and subsequent migration. While HOLCs are valuable in laparoscopy, their use near the VUAS should be limited to minimize the risk of complications. Kadekawa et al. reported a case of metal clip migration following radical retropubic prostatectomy, theorizing that local inflammation around the VUAS could contribute to clip erosion and subsequent migration. 16 That highlights the importance of careful clip placement during RALP, particularly when performing nerve-sparing dissections, where balancing HOLC use and alternative methods like low-energy bipolar coagulation remains challenging. 17 Although HOLC clips prevent thermal damage, their potential to migrate and contribute to urinary retention, stone formation, or BNS has led some surgeons to favor short-term, low-energy monopolar cauterization in their practice.18,19 As demonstrated by Hefermehl et al., cautery may be of concern due to lateral temperature spread, causing potential damage to sensitive structures, including nerves. 20 Prospective randomized or comparative studies could help clarify whether electrocautery poses greater risks than clip use. However, due to numerous confounding factors, animal model studies employing modern robotic techniques—with and without clips—may provide more controlled insights.
Despite the retrospective and single-center nature, the presentation of this significant case series may be a noteworthy contribution to future studies that will shed light on the prevention and management of this long-term underreported complication, considering the limited data in the literature.
Conclusion
Intravesical HOLC migration is one of the conditions that physicians should consider when a patient has persisting obstructive and/or irritative LUTS that occur after RALP. This late-onset complication can be safely treated using endoscopic procedures and is not likely to recur. To lower the risk of long-term complications, surgeons should avoid placing HOLCs close to the vesicourethral anastomosis and ensure that any loose clips are removed at the end of the surgery.
Footnotes
Authors’ Contributions
B.O.: Writing—review and editing, writing—original draft, software, methodology, investigation, and conceptualization. A.V.: Writing—review and editing, writing—original draft, methodology, investigation, and resources. K.C.S.: Writing—review and editing, data curation, visualization, and investigation. F.I.: Validation, methodology, and investigation. H.K.: Formal analysis and validation. E.A.K.: Writing—review and editing, formal analysis, and validation. E.A.: Writing—review and editing, conceptualization, and supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
There is no funding source.