
Abstract
Abstract
Background:
The knowledge of where does excess tissue fluid accumulate in obstructive lymphedema is indispensable for rational physical therapy. However, it has so far been limited to that obtained from lymphoscintigraphic, ultrasonographic, and MR images. None of these modalities provide composite pictures of dilated lymphatics and expanded tissue space in dermis, subcutis, and muscles. So far, only anatomical dissection and histological processing of biopsy material can visualize the tissue lymphatic network and the sites of accumulation of the excess of mobile tissue fluid.
Methods and Results:
We visualized the “tissue fluid and lymph” space in skin and subcutaneous tissue of foot, calf, and thigh in various stages of lymphedema in specimens obtained during lymphatic microsurgical procedures or tissue debulking, using special staining techniques. The volume of accumulated fluid was calculated from the densitometric data of stained tissue sections. We found that lymph was present only in the subepidermal lymphatics, whereas the collecting trunks were obliterated in most cases. Mobile tissue fluid accumulated in the spontaneously formed spaces in the subcutaneous tissue, around small veins and above and underneath muscular fascia. Deformation of subcutaneous tissue by free fluid led to formation of interconnecting channels. The volume of subcutaneous free fluid ranged around 50% of total tissue volume and there were no significant differences in various stages of lymphedema. This could be explained by the presence of thick layers of subcutaneous fat tissue even in the most advanced stage of lymphedema.
Conclusions:
In lymphedema caused by obliteration of collecting trunks, lymph is present only in the subepidermal lymphatics, whereas the bulk of stagnant tissue fluid accumulates in the subcutaneous tissue and above and beneath muscular fascia. These findings should be useful for designing pneumatic devices for limb massage as well as for rational manual lymphatic drainage in terms of sites of massage and level of applied external pressures.
Introduction

Typical image of damaged lymphatics and nodes and histological pictures of biopsy of these structures in obstructive lymphedema. Left panel: a lymphoscintigram of lower limbs in a patient after hysterectomy because of cancer and removal of iliac lymph nodes. The tracer injected into toeweb is poorly absorbed, it spreads in the dilated superficial lymphatic plexus. No collecting trunks are visible. A small solitary lymph node in the inguinal area. Right panel: histological picture of the biopsied node shows distorted architecture with remnants of lymphoid tissue (arrow) (mAb against CD3 lymphocytes staining, magn. X200). Below a picture of a collecting trunk almost totally obliterated (H-E staining, magn.x 200). Bottom picture depicts irregular network of subepidermal lymphatics (Paris Blue staining, magn. X100).
Our image of the limb lymphatic network in physiological as well lymphedema conditions is based on lymphographic or lymphoscintigraphic pictures depicting the superficial and deep systems and lymph nodes.7,8 This technique does not allow visualization of minor lymphatic structures located under the epidermis. Direct lymphangiography with fluorescent tracers may be helpful for delineating minor dermal lymphatics but it is rarely used as requiring special equipment. 9 Ultrasonography, computer-assisted tomography, and magnetic resonance imaging provide pictures of tissue spaces filled up with stagnant tissue fluid, however, they do not show lymphatics.10–12 Thus, none of the listed methods provide images to give us an idea how does the entire “tissue fluid and lymph space,” comprising interstitial space and lymphatics, look in reality. It remains difficult to imagine how does tissue fluid, in the areas with obstructed lymphatics, find its way to the normal noncongested tissue regions and gets absorbed there. So far, only anatomical dissection and histological processing of biopsy material can visualize the tissue lymphatic network and the sites of accumulation of the excess of mobile tissue fluid.
It would be useful for reasons of rational manual and pneumatic physiotherapy and pharmacological treatment to visualize and calculate the volume of the “tissue fluid and lymph space,” that is of the lymph vessel network of skin, subcutis, and lymph nodes, as well as the expanded interstitial space between subcutaneous collagen bundles, around blood vessels, in and around muscular fascia.
In this study, we visualized the “tissue fluid and lymph” space in skin and subcutaneous tissue of foot, calf, and thigh in various stages of lymphedema in specimens obtained during lymphatic microsurgical procedures or tissue debulking. The volume of fluid accumulating in the tissue space was calculated from densitometric data of the microscopic sections.
Material and Methods
Tissue specimens
Groin, calf, and foot skin and subcutaneous tissue and inguinal lymph node specimens were obtained from randomly selected 25 patients with lower limb obstructive lymphedema stage I to IV, successively as they came to our out-patients clinic to undergo elective lympho-venous shunt or debulking surgery. Control specimens were obtained from 10 patients with normal limbs operated upon for correction of fracture malunion. Fragments of inguinal lymph nodes were harvested during the lympho-venous shunt operations.
Lymphedema either developed spontaneously or after an episode of dermatitis or following infected foot abrasion. The average duration period of swelling was at the time of admission 6 ± 1 years. Sixty-five percent of patients experienced at least one attack of recurrent dermato-lymphangio-adenitis (DLA) over the last year and were treated with antibiotics. Staging of edema was based on own classification. 13 Excluded were patients with acute DLA, skin ulcers, chronic venous insufficiency, limb ischemia, limb lipedema, and rheumatoid arthritis. The study was approved by the Ethics Committee of the Warsaw Medical University and the Indian Council for Medical Research. Oral informed consent of patients was obtained.
Tissue staining for visualizing the tissue fluid and lymph space
Sites of accumulation of stagnant tissue fluid in the interstitial space and lymphatics were visualized by injecting the composite skin, subcutaneous tissue, and fascia blocks with Paris blue dye in chloroform suspension13–15 (Fig. 2). Fragments of lymph nodes were injected under the capsule. Large particles of this dye specifically enter lymphatics but not blood vessels. They are retained in dilated free tissue spaces and color their walls. The injected tissue fragments were placed in 5% formaldehyde, then treated with increasing concentrations of ethyl alcohol from 70% to 96%. To become translucent they were processed in methyl-salicylate solution. One hundred to three hundred thick fragments were sectioned and investigated under the light transmission microscope. The surface area of colored structures was measured under light microscope, magnification x100, using the Olympus Microimage software (Olympus, Japan) and expressed in percentage of the area of the microscopic field. The longitudinal and vertical length of stained spaces was measured to calculate their volume and expressed as percentage of tissue fragment volume.

Specimen of skin and subcutaneous tissue obtained during debulking surgery from lower limb with lymphedema stage IV. Paris Blue dye was injected intradermally and stained the tissue at the depth of 5 cm (thick arrow). The stained fragments were made translucent for stereomicroscopic evaluation of subepidermal lymphatics and tissue spaces filled with fluid and immunohistochemistry. The thin arrows show “blisters” containing tissue fluid.
In order to prove that the stained spaces were not blood vessels, 5 × 5 mm thick fragments of Paris Blue injected tissues were snap frozen at 70°C and sectioned for immunohistochemical evaluation of the bluish stained structures. They were stained with monoclonal antibodies to lymphatic endothelial cell hyaluronan receptor LYVE 1 (R&D, Europe) and FVIII and CD31 (Dako, Glostrup, Denmark) to identify blood endothelial cells.
Measuring water content of lymphedematous tissues
Fragments of lymphedematous and normal skin and subcutaneous tissue were weighted and placed in an electric oven at 240°C for 24 h. The dried specimens were weighted and differences in the fluid and dry mass between lymphedema and normal tissues were calculated.
Statistical evaluation
Differences between investigated groups were evaluated using Student's t-test with significance at P < 0.05.
Results
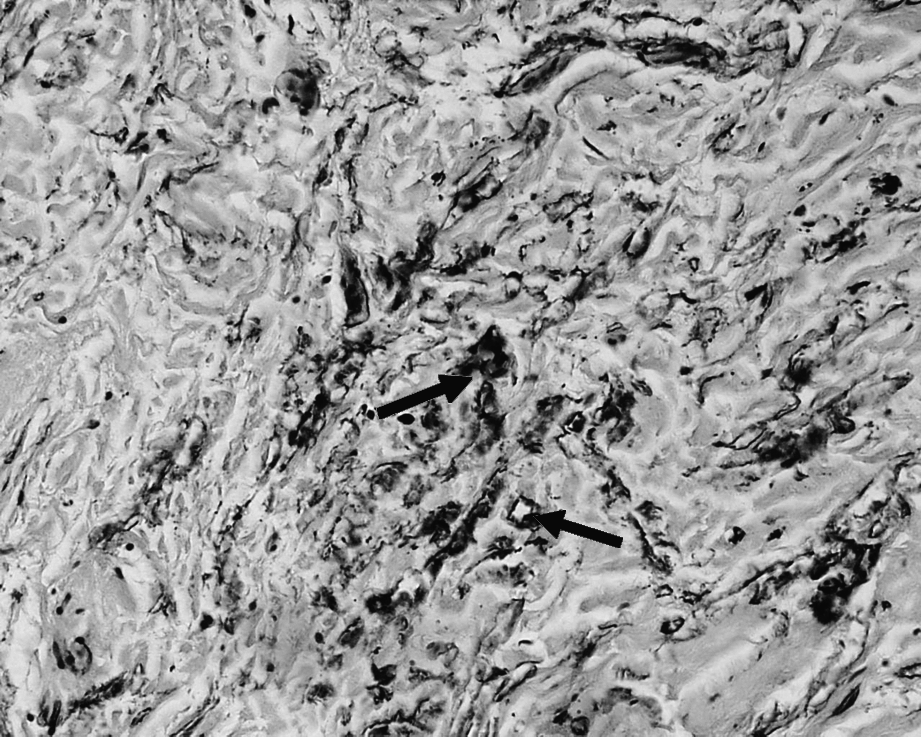
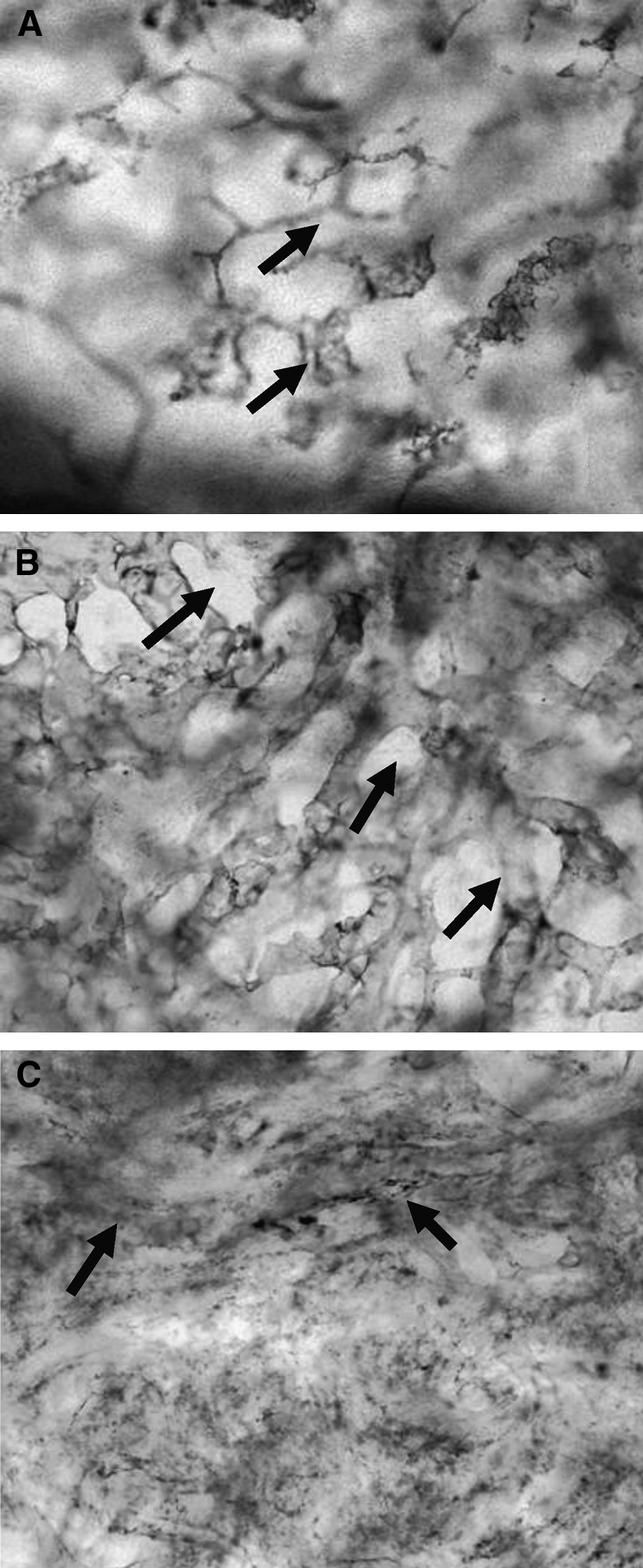
Obstruction of lymph flow by damage to the lymphatic collectors caused dilatation of the subepidermal lymphatics and formation of tissue fluid spaces in the subcutaneous tissue, around small veins, and in the muscular fascia (Fig. 3). In order to analyze where does lymph and tissue fluid accumulate, three anatomical regions as dermis, subcutaneous tissue, and muscular fascia were investigated. The subepidermal lymphatic plexus was found dilated and could be easily discriminated from blood vessels by positive staining against LYVE1 and by their shape (Fig. 4). This plexus was also visualized by intradermal injection of Paris Blue in chloroform suspension (Fig. 5). The architecture of arteries and veins in the same skin region looked different from lymphatics (Fig. 6). In the course of lymphedema, the subepidermal plexus undergoes gradual destruction and its deeper vessels become obstructed (Fig. 7). Most of the stagnant tissue fluid was found accumulating in the subcutaneous space composed of fibrous and fat tissue. Excess tissue fluid brought about deformation of tissue structures, leading to formation of irregular shape channels (Fig. 8). Their walls were not lined up by lymphatic endothelial cells and did not stain with mAb against LYVE 1. With progression of lymphedema, the subcutaneous space becomes enriched in fibrous structures, newly formed channels close down, and fluid accumulates in narrow spaces between collagen bundles (Fig. 9). Mobile tissue fluid finds its place also in the perivascular areas (Fig. 10). Interestingly, tissue fluid accumulated also in the thickened fascia forming multiple narrow longitudinal channels (Fig. 11). The main lymphatic collectors remained obstructed and could not be visualized.

Histological picture of calf skin and subcutaneous tissue in obstructive lymphedema stage III. Specimen stained with Paris Blue and H-E. Thick epidermis protruding into dermis. Minor structures in the papillary dermis are multiple small dilated subepidermal lymphatics (arrows). In the reticular layer of dermis, wide spaces filled with fluid are seen (arrows). Deeper in subcutis, these spaces become larger. The nonstained spaces between collagen bundles are presumably not connected with other tissue spaces (magn. X200).
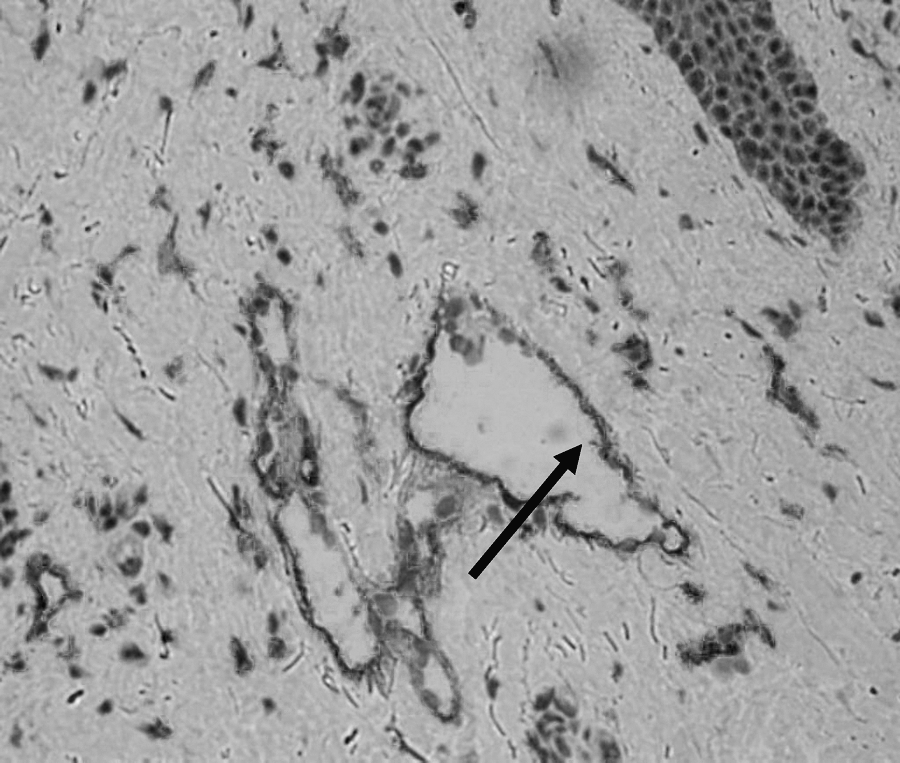
The reticular dermis showing LYVE 1 positive lymphatic vessels (the same patient as on Fig. 2) (arrow). Free spaces between collagen bundles filled with fluid are LYVE1-negative, having no lymphatic endothelial lining. Stain mAb against LYVE1, H-E, magn. X200.

Dilated calf skin subepidermal lymphatics stained with Paris Blue in a patient with lymphedema stage II. Upper panel, epidermis, lower panel, papillary dermis. A network of lymphatics still has competent valves. Some lymphatics are almost piercing epidermis. The stained area occupies 68% of the surface and 53% of the specimen volume (magn. X100).

Arteries and veins of calf skin of the patient as in Figure 2 stained by intravascular injection of Paris Blue. (
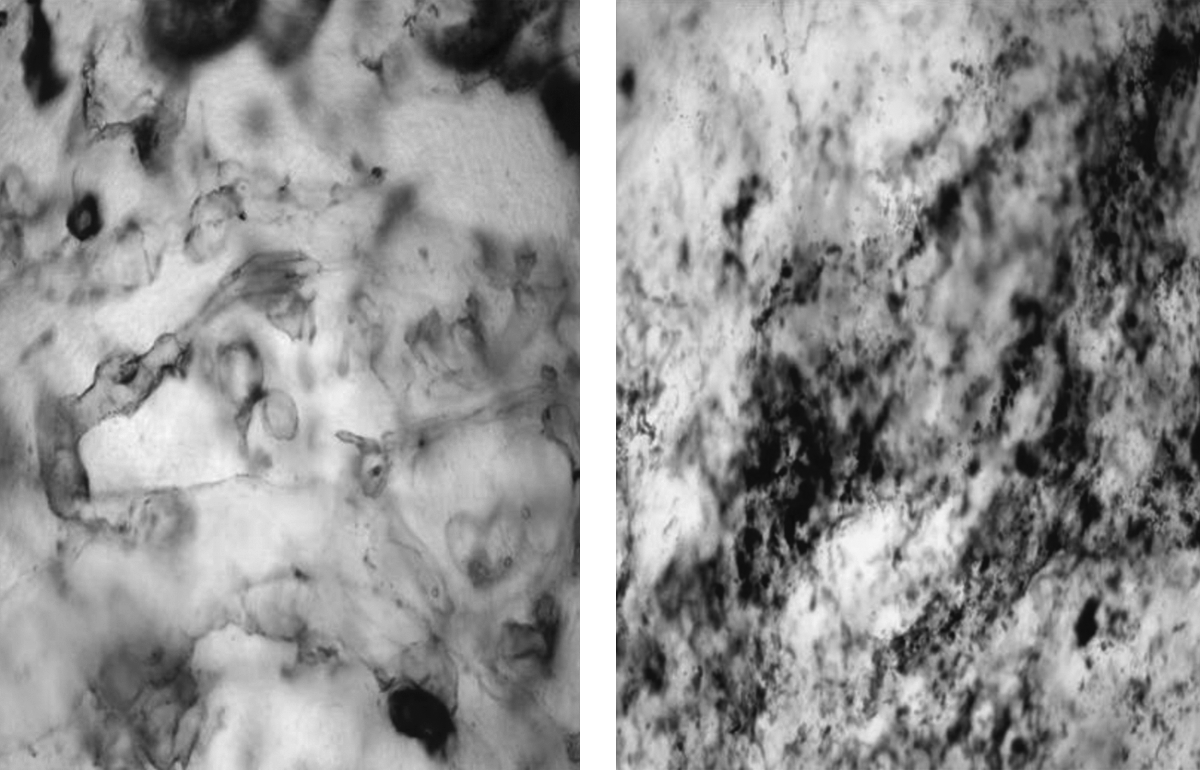
Groin skin in lymphedema stage III/IV. Left panel, dilated subepidermal irregular network of lymphatics. Right panel, deeper in the reticular layer; no lymphatics. Multiple miniscule “lakes” of injected dye depict sites of accumulation of stagnant tissue fluid. Paris Blue stain, magn. X100.
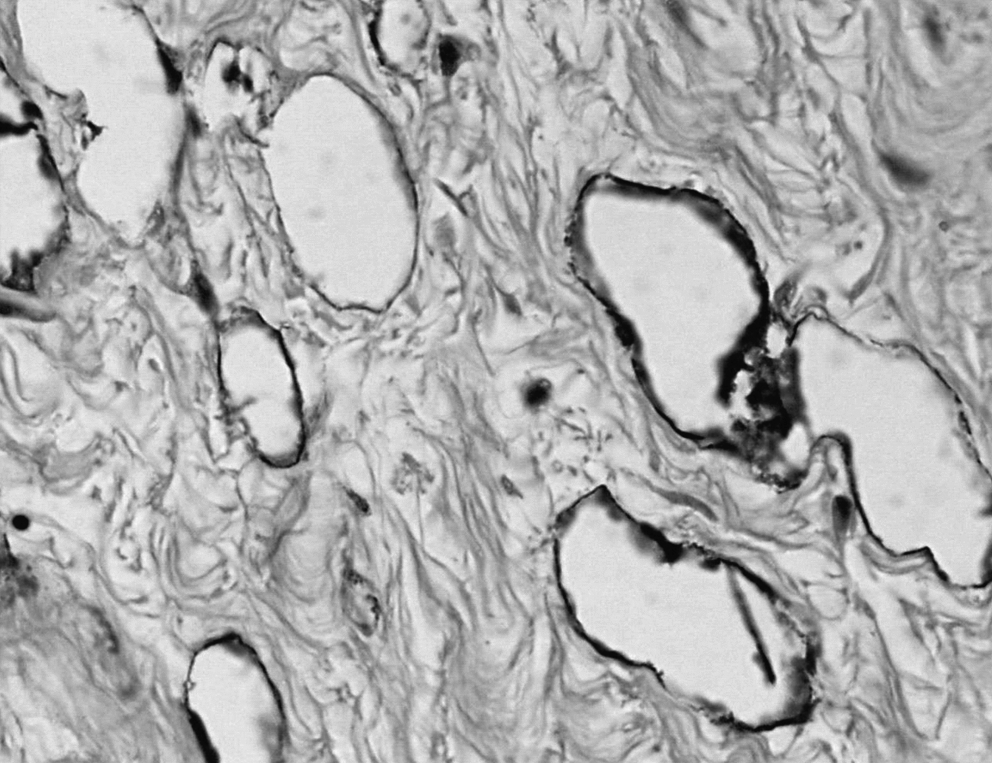
Calf subcutaneous tissue at the border with muscular fascia (same patient as in Fig. 2). Large oval structures are dilated artificial tissue spaces. They are not lined by lymphatic endothelial cells (LYVE1-negative). Paris Blue + H-E stain, magn. X400.

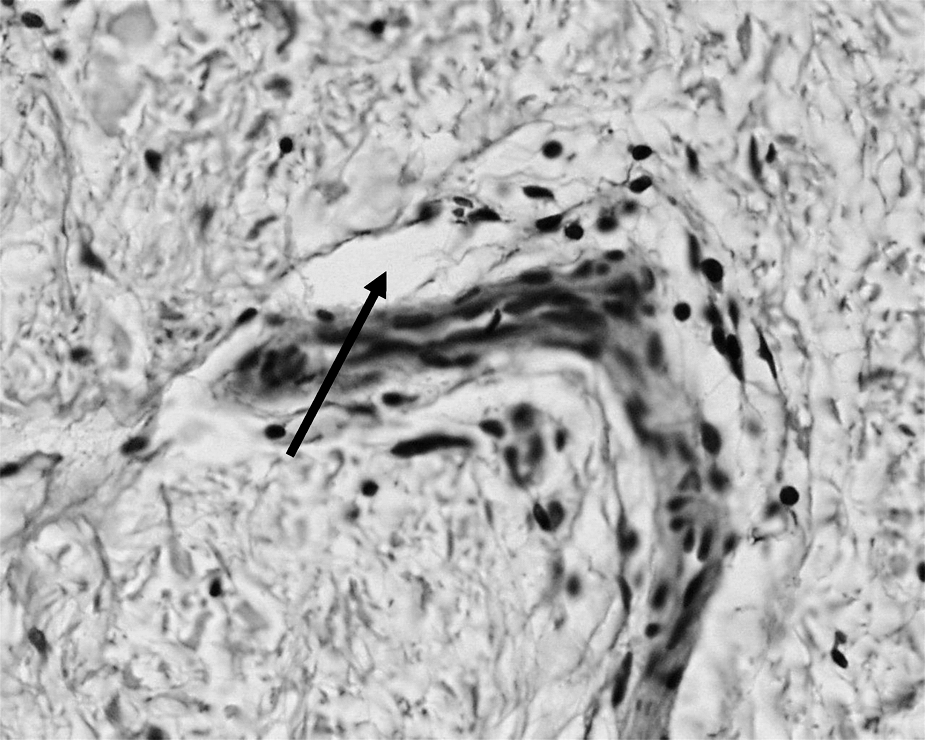
Calf subcutaneous tissue in lymphedema stage IV. Narrow longitudinal structures are remnants of small lymphatics (arrow). The injected dye stains spaces between fibrous structures and fat tissue. Paris Blue stain, magn. X100.
A medium size vascular bundle in the subcutaneous tissue. A stained space around the vein formed by stagnant fluid (arrow) (Paris Blue staining, magn. X100).
Muscular fascia in calf lymphedema (same patient as in Fig. 2). Multiple irregular collagen bundles separated by free spaces filled with fluid (arrows). Many of them stained with Paris Blue. H-E, X100.
Quantitative evaluation of the surface and volume of dilated subepidermal lymphatics and spontaneously formed tissue spaces revealed that up to 60% of tissue volume was occupied by stagnant lymph and tissue fluid. Interestingly, no significant differences between the foot, calf, and thigh skin and subcutaneous tissue with respect to the percentage of accumulated fluid per tissue volume were found (Fig. 12). However, there was less fluid in very advanced stages of lymphedema, although the differences between early and late stages were statistically nonsignificant (Fig. 13).

The percentage of skin area occupied by dilated subepidermal lymphatics (first three bars) and tissue spaces in the subcutaneous tissue in the groin, calf, and foot in lymphedema stage II to IV. N = 18, mean values ± SD. Note even distribution of accumulation of lymph in subepidermal lymphatics and tissue fluid in the subcutaneous tissue of foot, calf, and groin.
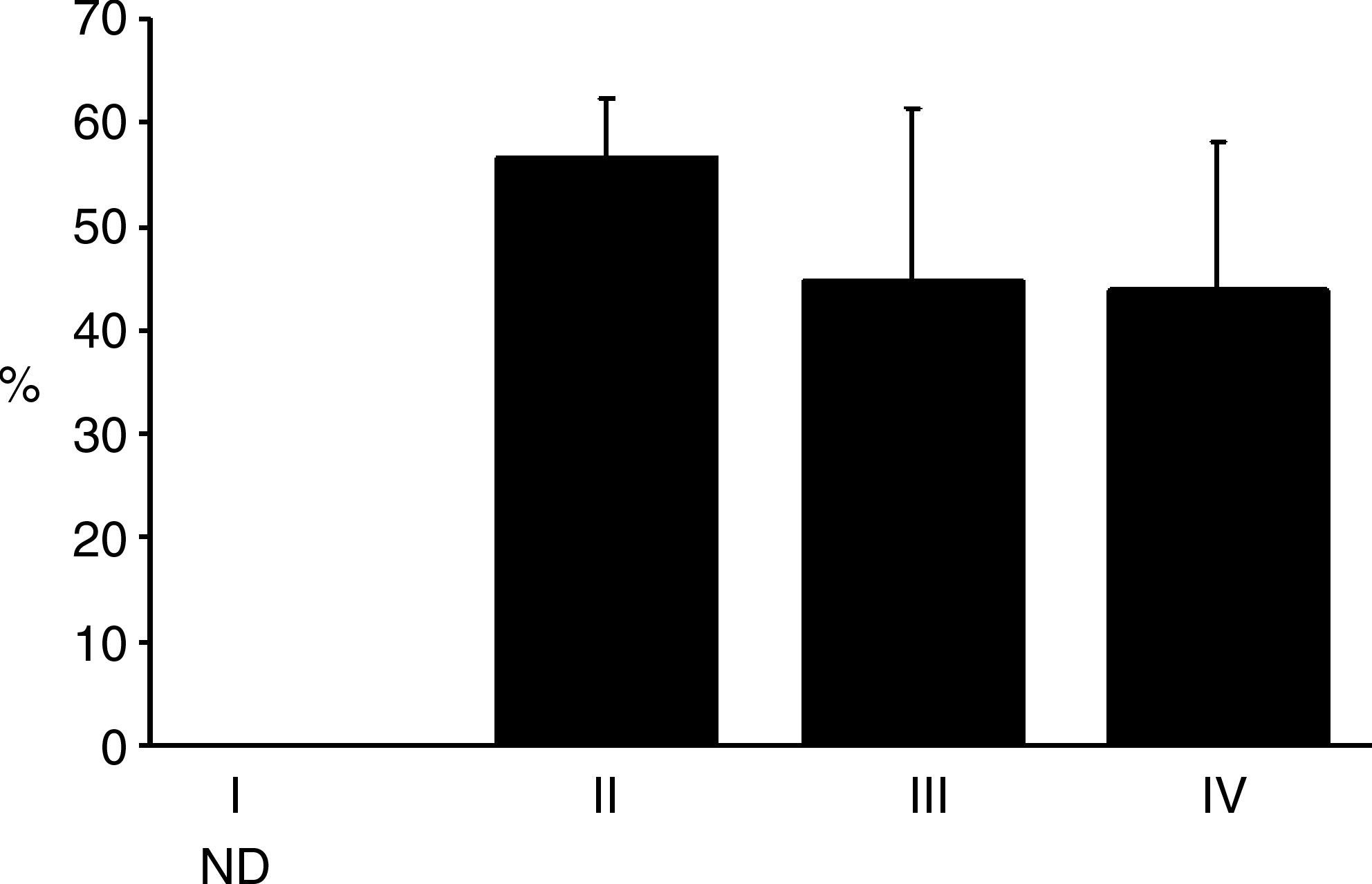
The percentage of skin area occupied by dilated subepidermal lymphatics and tissue spaces in the subcutaneous tissue lower limb in lymphedema stage II to IV. Note lack of differences in various stages of lymphedema. N = 18, mean values ± SD. This could be explained by the presence of thick layers of subcutaneous fat tissue in all stages.
Measuring water content of the lymphedematous tissues revealed an increase by 60 ± 6% compared with control, whereas the dry mass increased by 12 ± 2%.
Inguinal lymph nodes revealed obliterated lymphatic sinuses. Their endothelial cells did not stain with antibodies against LYVE1 (Fig. 14). No extrasinusoidal accumulation of fluid was seen.
Lymphatic sinuses of the inguinal lymph in normal condition and obstructive lymphedema stained with Paris Blue dye. (
Discussion
Our studies are the first in the literature visualizing sites of accumulation of stagnant lymph and tissue fluid in tissues with obstructive lymphedema and providing data on their volume. We found that lymph was present only in the subepidermal lymphatics, whereas mobile tissue fluid accumulated in the spontaneously formed spaces in the subcutaneous tissue, around small veins, and around and in the muscular fascia. Foot, calf, and thigh subcutaneous tissue contained similar volumes of fluid reaching on the average 50% of the total tissue volume.
The most superficial layer accumulating fluid was the subepidermal lymphatic plexus occupying a 200–300 μ thick papillary and reticular dermis. The volume of fluid in this plexus is negligible, compared with the volume of the subcutaneous tissue fluid and does not exceed 2%–3% of total tissue fluid retained in soft tissues (own measurements). Some vessels of the subepidermal plexus pierced epidermis and formed small surface blisters. The reason why subepidermal lymphatics remain patent while the collecting trunks are obstructed remains unclear. In advanced stages of lymphedema, progressing fibrosis of dermis brought about gradual obliteration of the plexus.
The bulk of mobile tissue fluid accumulated in the subcutaneous tissue forming artificial partly interconnected spaces. These spaces were located between fat globules, fibrous bundles, and around small veins. Interestingly, we did not find statistically significant differences between the rate of fluid accumulation in foot, calf, and thigh, and the stage of disease. This may be accounted for by the fact that although skin was thicker in the foot and lower calf than in the thigh, the structure of the subcutaneous tissue remained similar in all parts of the limb with dominance of adipose tissue. Formation of large perivascular spaces by tissue fluid could be explained by the presence of lax connective tissue in these regions, its high compliance, and subsequently low resistance to flow.
A new finding was formation of tissue fluid channels around and in the hypertrophic muscular fascia of the calf, reaching in some areas 2 cm in thickness. These were narrow longitudinal spaces between the normal fascial fibrous elements. The hydraulic conductivity of these structures was certainly high because of linear positioning of fibers.
The volume of fluid accumulating in the tissue spaces and calculated from densitometric readings of the stained tissues was reaching 50%–60% of tissue volume. Our data on water concentration in harvested specimens remained in accordance with these figures.
The inguinal lymph nodes revealed major changes in the sinuses as obliteration and formation of blind spaces and depletion of lymphoid elements. High resistance to lymph flow in the fibrotic nodes may be a factor causing stagnation of lymph in the rudimentary patent afferent lymphatics.
Measuring tissue water content and its topographical distribution may be done using noninvasive methods such as MRI. However, the resolution power of MR is still to low to show minor lymphatics, small tissue fluid “lakes” and thin fluid layers above and under fascia. Fumiere et al. found that normal subcutaneous septa are seen as hyperechogenic lines in ultrasound and hyposignal lines in MRI and that hyperechogenic subcutis in ultrasonography can be due to interlobular and intralobular water accumulation and/or to interlobular and intralobular fibrosis. 16 However, they advised multiple imaging modalities to delineate precisely the nature of tissue water accumulation in lymphedema. Idy et al. demonstrated water retention diffusely spreading over the entire dermis and fluid retention located in the interlobular spacing and beside the superficial fascia. 11 Inside the subcutis, they identified superficial fat lobules but not so much fluid accumulation. Bioimpedance analysis provides an index of volume of the affected and nonaffected limb but does not give insight into topography of free fluid accumulation. 17
This being so, our observations, based on studies of harvested tissue, supplement the knowledge obtained from the noninvasive imaging on the topography of mobile fluid accumulation and shape of channels in the edema-deformed tissue. The knowledge of where the tissue fluid is located should be useful for designing pneumatic devices for limb massage, as well as for rational manual lymphatic drainage.