
Abstract
Abstract
Background:
Following treatment for breast cancer 12%–60% develop breast cancer-related lymphedema (BCRL). There are several ways of assessing BCRL. Circumference measurement (CM) and water displacement (WD) for volume measurements (VM) are frequently used methods in practice and research, respectively. The aim of this study was to evaluate CM and WD for VM of the BCRL arm and the contralateral arm, comparing the results with regional dual energy X-ray absorptiometry (DXA).
Methods and Results:
Twenty-four women with unilateral BCRL were included in the study. Blinded duplicate VM were obtained from both arms using the three methods mentioned above. CM and DXA were performed by two observers. WD was performed by a group of observers. Mean differences (d) in duplicated volumes, limits of agreement (LOA), and 95% confidence intervals (CI) were calculated for each method. The repeatability expressed as d (95% CI) between the duplicated VM of the BCRL arm and the contralateral arm was for DXA 3 ml (-6–11) and 3 ml (1–7), respectively. For CM and WD, the d (95% CI) of the BCRL arm were 107 ml (86–127) and 26 ml (-26–79), respectively and in the contralateral arm 100 ml (78–122) and −6 ml (-29–17), respectively.
Conclusions:
DXA is superior in repeatability when compared to CM and WD for VM, especially for the BCRL arm but also the contralateral arm.
Introduction
BCRL is a progressive condition defined as clinical chronic swelling, almost exclusively of the ipsilateral arm. Diagnostic criteria for BCRL varies in literature.3–7 The edema develops when the microvascular (capillary and venules) filtration rate exceeds lymph drainage, either because the filtration rate is high or because lymph drainage is low, or a combination of the two. 8 There is agreement that the fluid accumulation and swelling of the BCRL arm is due to reduced lymph transport capacity.9,10 However, the underlying mechanism is not fully understood. Damage to lymphatic vessels are most often caused by axillary lymph node dissection (ALND) and radiotherapy to the axilla, but wound infection, tumor stage, and obesity may also contribute to BCRL development.1,10–15
In addition to the functional and cosmetic impairments, BCRL can cause disturbed sensitivity of the arm, ulcerations, skin changes, increased risk of squamous cell carcinoma, as well as the rare (less than 1%) highly malignant lymphangiosarcoma, also known as Stewart–Treves angiosarcoma. 16
There is a variety of ways of diagnosing and measuring BCRL.3,5–7,13,15,17–19 However, no standardized methods to monitor BCRL progression or the effect of treatment exist. 5 Therefore varying measurement techniques and definitions are used in studies evaluating lymphedema.
Circumference measurement (CM) and water displacement (WD) for volumetric measurements are inexpensive, safe, and painless methods, although time consuming, difficult to perform, and with considerable intra- and inter-rater variation. Neither of these two methods are able to provide information about the tissue composition of the arm. CM is unsuitable for volume assessment of the hand. WD using Archimedes' principle (i.e., measuring the volume of an object by assessing the amount of water displaced) for volume measurement has a high logical validity and is at present widely recognized as the gold standard.5,20 However, it is far from being a bedside test and cannot be performed on patients who are unable to cooperate by holding their arms completely still. Furthermore, WD is unsuitable immediately after surgery due to wounds and dressings, as well as in the presence of severe skin disorders. Moreover, specially designed volumeters are needed.5,21 Therefore, CM has in our clinical setting been chosen as our clinical standard for diagnosing and monitoring BCRL. In contrast to CM, WD provides volume measurements of arms and hands.
Dual energy X-ray absorptiometry (DXA) is a method providing data on tissue composition given as fat mass (FM), fat-free mass (FFM), and bone mineral content (BMC).20,22–24 DXA can be performed on patients immediately after surgery as well as on patients with severe skin disorders, elderly, and very ill patients. It is easy and quick to perform, including computer-based registration and comparison with previous data. Furthermore, it is possible to analyze data for separate regions from one scan using anatomical landmarks from x-ray images of the scanned arm. Disadvantages include radiation dose, albeit negligible, inter-rater variations in drawing the regions of interest (ROI), and the relative contraindication of scanning pregnant women. The attenuation of X-rays depends on the positioning of the subject, thus DXA can be difficult to perform on patients who cannot cooperate.
There are other methods for assessing the volume of the arm such as perometry and bioimpedance which are based on infrared light and electric impedance respectively.19,25 These techniques are not available in our department and subsequently not included in the present study.
Aims of study
The primary aim of our study was to compare DXA as a new method for volume measurement of BCRL with the clinical standard of our clinic (CM) and the gold standard water displacement (WD).
Secondary duplicate measurements were performed to assess intra- and inter-observer variation of each method before being compared with the other methods.
Materials and Methods
Subjects
Twenty-four Caucasian females with unilateral BCRL were recruited from the Department of Physiotherapy where they were receiving or had recently received treatment for BCRL (Table 1).
On the day of the study.
After the primary operation.
At the time of the study.
Consisting of 2 Gy, 24 F, 5 F/w following surgery.
ALND; axillary lymph node dissection, BMI; body mass index.
The patients were initially diagnosed with BCRL on the basis of clinical symptoms consistent with BCRL (clothing or jewelry becoming tighter, feeling of heaviness, tightness, fullness or stiffness, aching, observable swelling), as well as a CM of two or more centimeters higher on the breast cancer-related arm than the contralateral arm in at least two points as measured by a trained physiotherapist at the time of diagnosis and initiation of treatment. The definition of BCRL as a CM increase of 2 cm or more between the BCRL arm and the contralateral arm at any given point is commonly used. 3 However, in our clinic, BCRL is defined as a CM increase of 2 cm or more between the BCRL arm and the contralateral in at least two points. The subjects' baseline characteristics were based on review of their medical files as well as from a questionnaire regarding their BC and BCRL arm. The subjects filled in the questionnaire prior to the study. On the day of the measurements, the questionnaire was looked through with the subjects along with the first author.
Exclusion criteria were conditions or medications known to affect body composition except if BC related, skin disorders that would not allow the subjects to immerse their arms into water or disorders affecting the subjects' ability to cooperate. No eligible subjects were excluded due to these criteria.
All subjects wore compression garments on a daily basis, but were instructed not to wear it on the day of the measurements. All measurements were for practical reasons performed consecutively within the same day in the following order: CM, WD, and DXA. The primary author reconfirmed which arm was the BCRL arm on the day of the study.
Ethics
The study was approved by the Danish National Committee on Biomedical Research Ethics and the Danish Data Protection Agency (registration No. 13792). Written informed consent was obtained prior to the study from all subjects. The study was performed in accordance with the principles set forth in the Declaration of Helsinki.
Circumference measurements
Circumference measurements were obtained using a tape measure by two experienced physiotherapists who work with BCRL patients on a daily basis (CM1 and CM2). Prior to the study the physiotherapists agreed upon and practised uniformity when performing CM measurements. The subjects were seated with their arms vertically along the truncus for CM. The first physiotherapist marked 6 points (C1–C6) with a 1 mm thick waterproof pen as described by Taylor et al. 26 Five of these points (C1–5) were used for CM (Fig. 1). Three of the points were at the following anatomical landmarks; the crease at the anterior distal end of the styloid process of the ulnae, the crease at the cubital fossa, and the anterior distal lateral part of acromion, with the latter only used for calculating the position of two other measurement points. The remaining three points were calculated as 50% respectively 65% of the distance from one anatomical landmark to the next. Both physiotherapists measured the circumferences of the arm twice consecutively at the measurement points. The first set of measurements was always blinded to the physiotherapist prior to the second set of measurements as well as to the second physiotherapist. The geometric volume of each segment of the arm was calculated using the formula for a truncated cone; V = h (C12 + C1C2 + C22)/12 π with V = volume; h = height of the segment; C1 and C2, = circumference at each end of the segment. The volumes of the four segments were summed and the sum referred to as the volume of the arm.
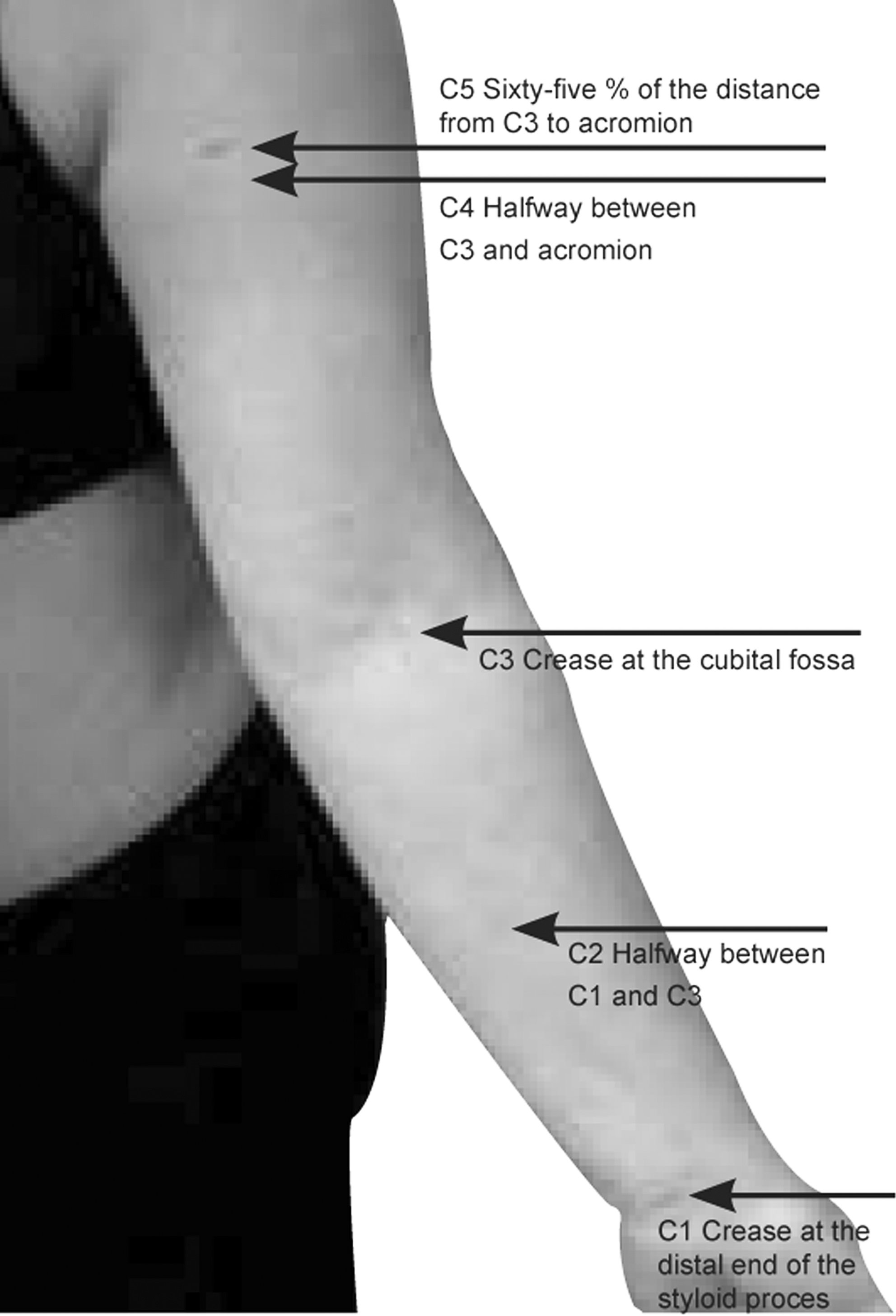
Five marks used by physiotherapists for circumference measurements.
Water displacement
The patients wore no clothing or jewelry except for two patients who wore a finger ring that could not come off.
Two specially designed volumeters were used: one for the hand only and one for the hand and arm. Both volumeters were cylindrical with an inner diameter of 19.5 and 12.5 cm, respectively, with heights at the overflow spout of 69 and 22 cm, respectively. Water temperature was measured before each WD with the mean temperature ± s of 30 ± 2°C.
Following careful instructions, the subjects were seated comfortably for the WD of the arm. The patients slowly immersed their arms into the volumeters until a horizontal line through C5 was seen flush with the water surface. The displaced water was collected in a separate container which was weighed (to the nearest g) before and after each WD using a calibrated kitchen scale (OBH Nordica type 9860, OBH Nordica Denmark). The subjects were stood up for WD measurement of the hand. Similarly, the patients immersed their hands to C1, the measurement point at the crease at the anterior distal end of the styloid process of the ulnae. The subjects were asked to rest their fingertips against the inside of the volumeter in order to keep the hand and arm as steady as possible until only few drops of water were dripping from the overflow spout for 5 seconds. The arm was then removed and dried. The WD procedure was performed twice for each arm and hand. The weight (g) of the displaced water was converted into ml using the standard conversion of 1 kg of water being equal to 1000 ml.
The volume of the arm was calculated as the mean of the duplicate measurements of the volume of the arm and hand subtracted by the mean of the duplicate measurements of the volume of the hand.
Dual energy X-ray absorptiometry
DXA is a method based on measurement of the tissue attenuation of an X-ray beam with two energy peaks. It accurately estimates the weight of the fat mass (FM), fat-free mass (FFM), and bone mineral content (BMC). Using the known densities of FM (0.9 g/cm3 = g/ml), FFM (1.1 g/cm3 = g/ml), and BMC (about 1.85 g/cm3 = g/ml), it is possible to estimate the volume of the arm.20,27 The same DXA scanner (Lunar Prodigy DXA mini fan beam scanner serial number DF + 13189, GE Medical Systems, Madison, WI) and software version (Small Animal Programme version 8.1027, individual analysis version) was used for all the scans and analyses. Before the scan, a thin lead armband was attached to the arm 1 cm above C5 (marked by the physiotherapists). The subjects were lying supine on the scan table with the arm distal to the lead armband separated from the truncus. If necessary, a thin elongated air filled balloon was used to ensure space between the arm and the truncus. The subjects were instructed to lie completely still during the scans. Each arm was scanned twice without repositioning. Scanning time was 3 min per scan.
When going through the DXA scans, it was noted that in some patients some of the soft tissue of the upper arm was marked as bone by the software. Subsequently, two examiners (DXA1 and DXA2) had to point type all scans. The results of each point typing were blinded both between the examiner's first and second point typing as well as between the two examiners. Regions of interest (ROIs) were drawn around the hand and the arm by each examiner on every scan. The results of each ROIs were blended between the examiner's first and second ROI. Results of the first examiners' ROIs were blinded to the second examiner. Both examiners agreed upon a uniform way of drawing the ROIs. The ROIs of the hand were drawn with an upper horizontal line through the distal end of the styloid process of ulnae. The ROIs of the arms were drawn using the above mentioned line as well as a line orthogonal to a point one cm distal along the lateral edge of humerus from the distal edge of the lead band.
For all three methods we did not redo any possibly fallacious readings or scans. No outliers were excluded before statistical analysis. All tests were for practical reasons done consecutively.
Statistical analysis
Duplicate measurements
For the duplicate volume measurements, the data are presented for both the BCRL arm and the contralateral arm as mean difference in volume (d), standard deviation of the difference (s), limits of agreement (LOA (d ± 2 s)), absolute and relative technical error of measurements (TEM), and intra-rater and inter-rater correlation coefficient (ICC). For inter-rater assessment of the two physiotherapists (CM1 and CM2) and the two DXA examiners (DXA1 and DXA2), a corrected standard deviation was calculated since the s of these mean of means were underestimated, because some of the effect of duplicate measurement error had been removed. 28 Bland and Altman plots of the difference against the average of the duplicate volume measurements (CMm and DXAm) arm are used to compare the duplicate volume measurements.28,29
Method comparison
The means of CM1 and CM2 (CMm), as well as the mean of DXA1 and DXA2 (DXAm), and the mean of the duplicate WD were used as our best estimates of the unknown true value of the volume of the BCRL arm and the contralateral arm with each method. The data are presented as mean difference in volume (d), standard deviation (s), and limits of agreement (LOA). Bland and Altman plots of the difference against the average of the methods compared (DXAm vs. CMm, DXAm vs. WD, and CMm vs. WD) are used for methods comparision.28,29
Results
Patients' characteristics are given in Table 1.
Duplicate measurements
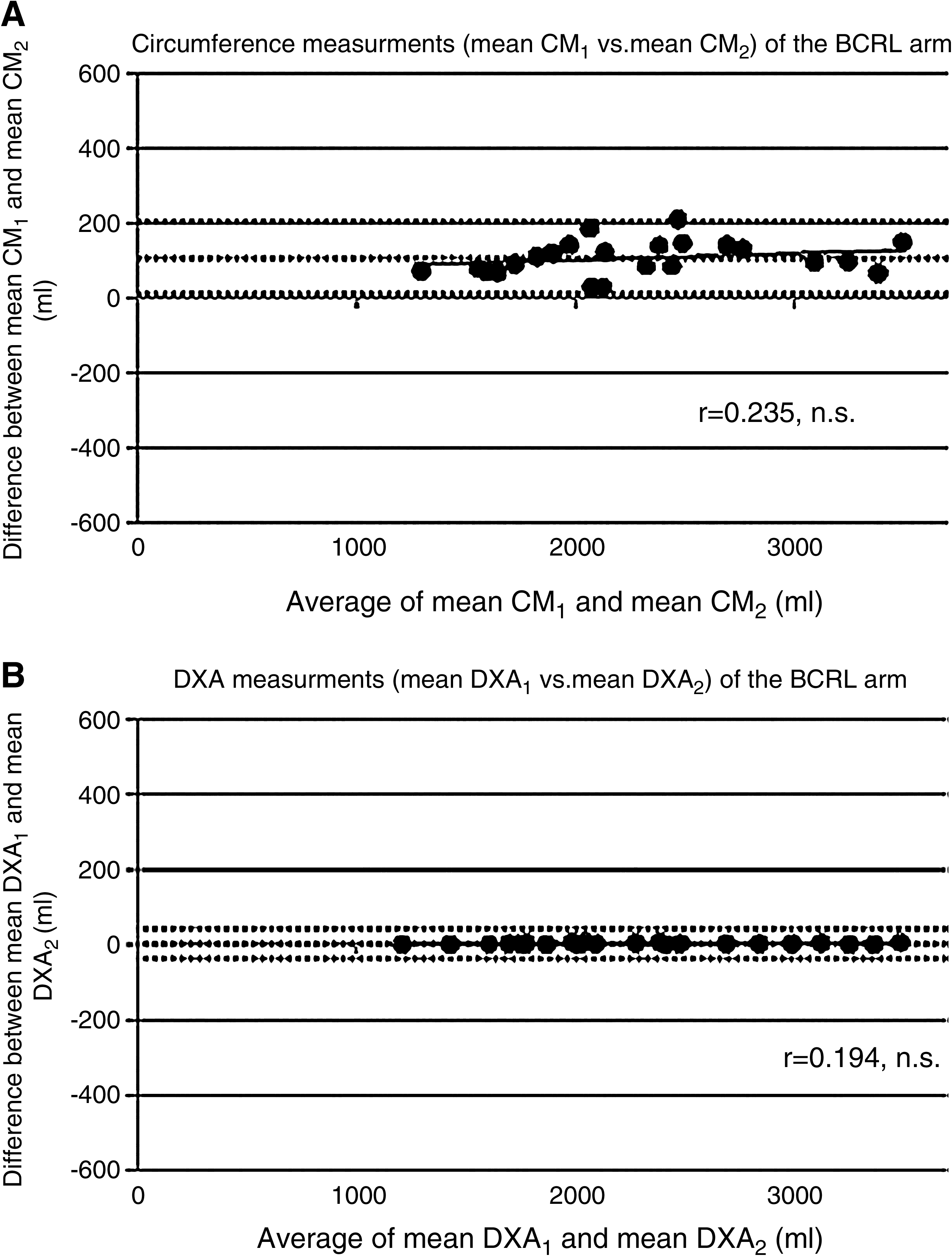
Intra-rater mean volume of the BCRL and the contralateral arm, LOA, TEM, TEM%, and ICC for CM, WD, and DXA are given in Table 2. LOA are widest for WD as compared to DXA and CM for both the BCRL and the contralateral arm. This is supported by higher TEM and TEM% values and lower ICC for WD. Table 3 shows the inter-rater mean volume, LOA, TEM, TEM%, and ICC. DXA has the narrowest LOA compared to CM and subsequent lower TEM, TEM% and higher ICC. Figures 2A and 2B illustrate the LOA for inter-rater agreement for CMm and DXAm (results from Table 3) and show that there is a systematic bias between CM1 and CM2, which is also supported by the higher TEM and TEM% and lower ICC for CM compared to DXA. There was no significant correlation between either CM or DXA with increasing arm volumes.
(
Method comparison
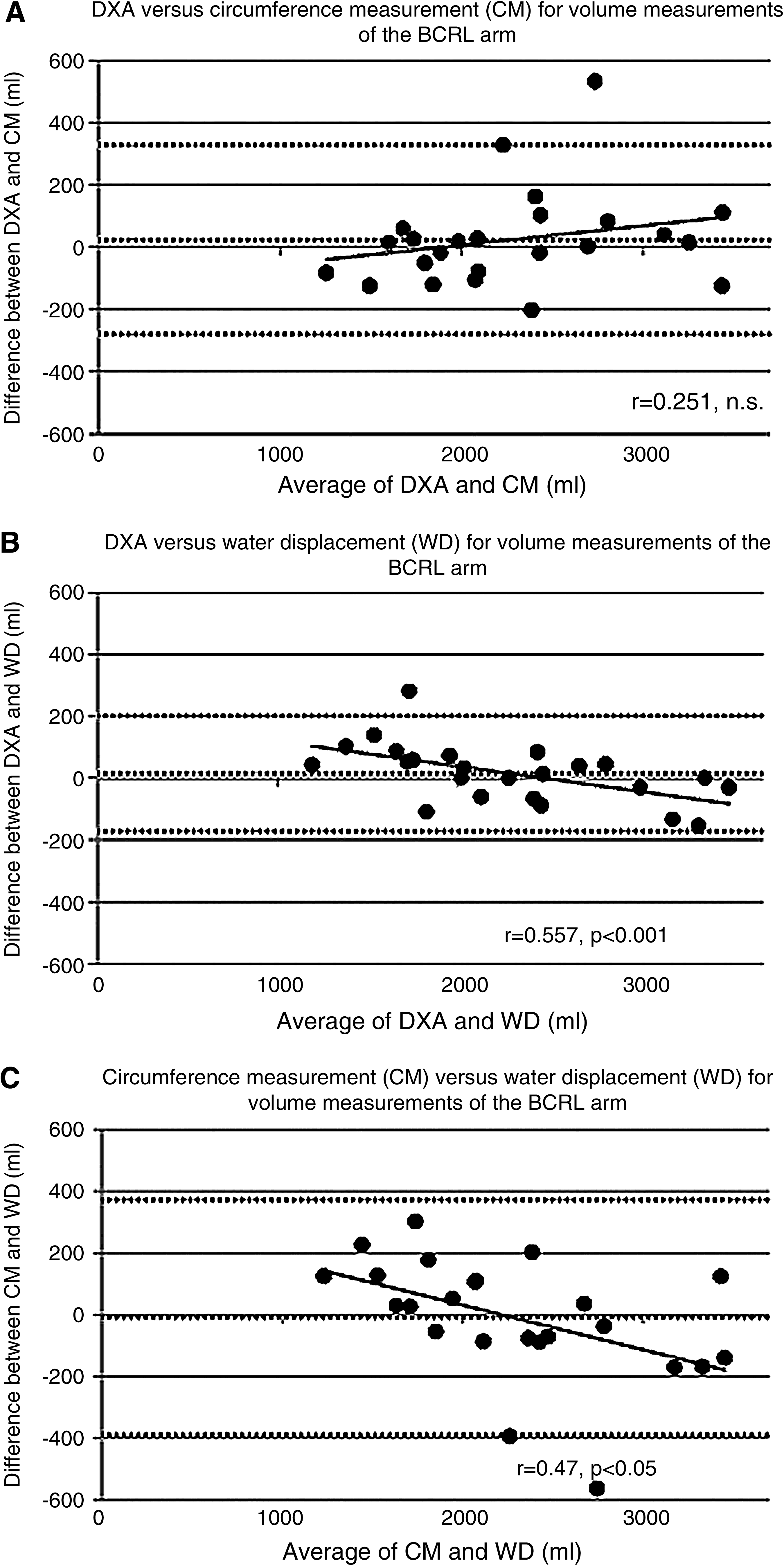
Limits of agreement for the BCRL and contralateral arm comparing the three methods are shown in Table 4 and illustrated in Figures 3A–3C. The narrowest LOA (best agreement) was found between DXA and WD. There was no systematic bias between DXA and CM.
(
However, WD significantly underestimated the volume of small BCRL arms and overestimated the volume of large arms compared to both DXA and CM using linear regression, as illustrated in Figures 3B and 3C.
The volume of the BCRL arm was greater than the volume of the contralateral arm in only 13 subjects (54%) with CM1 and 12 subjects (50%) with CM2, but in 23 subjects (96%) with WD, DXA1, and DXA2. A CM of two or more centimeters higher on the BCRL arm than the contralateral arm in at least two points were only found in five (21%) subjects by the one physiotherapist (CM1), six (25%) subjects by the second physiotherapist (CM2), with only four (17%) subjects being the same.
Discussion
We have found DXA to be superior to WD and CM for volumetric assessment of BCRL: Superior to WD because of better repeatability, superior to CM because of better inter-rater reproducibility. Moreover, there was a significant inter-rater bias for CM. DXA and WD are superior to CM in identifying subjective BCRL. This is somewhat surprising since diagnosis of BCRL was based on CM. We believe that this can be explained by the fact that the initial diagnosis was based on CM before treatment had taken place.
Circumference method
There was a poor agreement between the two physiotherapists' measurements (Fig. 2A). This could be caused by differences in how tight the tape measure was placed around the arm, failure to take the CM around the arm at right angles to its axis, as well as the exact location of the tape measure, even though the physiotherapists had agreed on a uniform way of measuring the CM prior to the study. Positioning of the arm when CM was taken could also affect the CM. However, prior to the study, the physiotherapists had agreed on having the subjects seated with their arms by their side when taking the CM. The six marks used for CM would clinically have to be marked out each time. This gives rise to further errors. The use of anatomical landmarks for sites of CM was shown in a previous study to be more accurate than the distances from fingertips because the segment would not span the elbow and therefore correspond better to truncated cones. 26 However, it requires more expertise and training of the examiners to use anatomical landmarks. We estimated arm volumes based on an assumed geometrical model of the arm (right circular truncated cone model) which is widely used, but for obvious reasons is not quite true. Arm volume could, alternatively have been estimated based on an assumed elliptical truncated cone model. 30 Another disadvantage of CM for volume measurements is the poor ability to measure BCRL of the hand, which often is clinically important.5,31 The repeatability was better for the contralateral arm than the BCRL arm. This could be due to the BCRL arm responding differently to physical force due to pitting and fibrosis. 21
On the basis of the poor level of agreement between the two physiotherapists, we do not find it clinically acceptable to use CM for volume measurements unless obtained by the same physiotherapist each time.
Water displacement
The level of agreement of half a liter for the duplicate volume measurements of the BCRL arm by WD is not clinically acceptable. This poor agreement is partly due to some outliers. We choose to retain the outliers for the statistical analysis. The level of agreement for the BCRL arm is poorer than for the contralateral arm. This could be caused by more difficulties holding the BCRL arm still due to altered sensitivity, aching, feeling of heaviness or stiffness, which are common symptoms of lymphedema.
The poor agreement of WD for volume measurements regarding repeatability and the significant underestimation of small volumes and the overestimation of large volumes compared to both DXA and CM could be caused by the participants' possible lack of ability to hold their hand and arm completely still while immersed as water was coming out of the overflow spout, because the subjects with large arms will have an increased tendency to cause sloshing and thereby overflow. Also, differences in the angle of which the arm and hand were immersed into the water each time could reduce the level of agreement. However, attention was taken to positioning during the consecutive WD. The volume of the hand was used to subtract from the volume of the arm and hand to assess the volume of the arm excluding the hand. Therefore, possible errors of both the WD of the arm and hand as well as of the hand can reduce the level of agreement.
We believe that our difficulties with WD would be similar in a clinical setting. However, the marks used for WD would be drawn on occasion by different examiners. Also, the way of monitoring the extent to which the arm and hand were immersed each time might be different, as well as differ between the different examiners. This could produce even larger errors.
Dual energy X-ray absorptiometry
The differences between the duplicate volume measurements by each examiner as well as between the two examiners were small as compared to the other two methods. Therefore, we found DXA to be superior for measuring the volume of the BCRL arm and the contralateral arm.
DXA is simple to perform on hands and arms and is even suitable for elderly and very sick patients. The patients are not enclosed and only have to lie still for a few minutes. The scan time is not different from the time spent for CM and WD. Disadvantages of using DXA include exposure to radiation. However, the effective dose of only 5 μSv is negligible compared to the yearly natural background radiation to the whole body in Denmark of 3–4 mSv and even allows for repeated measurements. One disadvantage includes having to use the same software and the same DXA scanner or at least a machine from the same manufacturer to allow sufficient repeatability for follow-up comparisons. 32 Calibration of DXA scanners is important and cross calibration is difficult and time consuming. DXA cannot be performed in patients who cannot lie still during scans. However, this potential problem did not occur in our study. Reproducing positioning of the arm from scan to scan could present a problem. To assess this possible problem, the subjects could have been scanned twice with repositioning in between the two scans. Tothill et al. DXA scanned one volunteer four times supine and four times prone. 33 Results of the arms showed significant differences in the bone measurements as well as differences of the soft tissue measurements between the two orientations. However, scanning patients consistently supine would avoid such problem. We used software originally designed for measurement of small animals, due to a better resolution that allowed both more precise definition of ROIs and the possibility to perform manual definition of bone and soft tissue. The latter was performed by two examiners with differences in mean volume calculations of the BCRL arm of only 3 ml. Brorson et al. have also used DXA scans on 16 patients with BCRL but used a different software and other densities for bone than in the present study. 20 They found a high correlation between WD and DXA and suggested that DXA can be used to estimate the excess volume but they do not provide data on the limits of agreement in their method. Perometry is a method with reported high precision for volume measurements. In principle it works as a CT-scanner with infrared light instead of X-rays. Cross-sectional segments are measured every few mm along the arm while the arm is positioned in a frame with a mobile infrared source. Volumes are computed from summation of the segments. 34 Bioimpedance which is a method based on the assumption that the magnitude of the opposition to the flow of an electric current through the limb is inversely proportional to the volume of the fluid in the tissue has been shown to correlate closely with perometry. 25 Perometry and bioimpedance are potentially portable methods which is an advantage for clinical use. Since DXA has proven to be superior to the classical methods (WD and CM) in the present study, a head-to-head comparison of DXA to perometry and bioimpedance is highly relevant.
Conclusion
DXA is a strong candidate to become a new gold standard for diagnosing and monitoring BCRL compared to WD and CM, due to its better reproducibility. The individual physiotherapist's CM is clinically acceptable for volume measurement, but its poor inter-rater variation makes it less reliable and dependent on the same physiotherapist. WD is difficult to perform and has a poor repeatability, although identifying the same patients as DXA with volume differences between BCRL and contralateral arm.
Footnotes
Acknowledgments
We thank Theis C Hansen, Merete C Wittenkamp, Malene D Nielsen, Jann B Lohse, Teresa S Madsen and Michele W Sandholdt and, most importantly, all the patients who participated.
Author Disclosure Statement
Drs. Gjorup, Zerahn, and Hendel all report no competing financial interest.