
Abstract
Abstract
Lymphangioleiomyomatosis (LAM) is a rare, slowly progressive neoplasm that causes gradual but often life-threatening cystic destruction of the lung. Advances in our understanding of the molecular and cellular pathogenesis have LAM have identified a number of promising targets for testing in therapeutic trials. However, the design, prioritization, organization, and implementation of clinical trials in rare lung diseases poses unique challenges, including geographically disperse populations, sluggish enrollment, off- label drug use, burdensome regulations, and paucity of validated surrogate endpoints.
Overview of Interventional Trials in LAM

Signaling pathways and targets for LAM. Binding of ligands to cell surface receptors such as the insulin receptor and platelet-derived growth factor receptor (PDGF) result in phosphorylation of downstream proteins (e.g., IRS 1, PI3K, PDK1 downstream of IRS 1) and ultimately Akt. The estrogen receptor (ER) can also signal through Akt. Akt activates the TSC1/TSC2 complex, which in turn downregulates the activity of mTOR, the mammalian target of rapamycin, through an intermediate protein called Rheb. In the absence of TSC1 or TSC2, the mTORC1 complex (composed of mTOR and raptor and msLT8 (not shown)) is constitutively activated, resulting in inappropriate ribosome biogenesis, protein translation, and cell growth (through downstream effectors S6K and S6, as well as 4EBP1 and eIF4E), and downregulation of autophagy. mTORC2 (composed of mTOR, msLT8, and rictor), which controls cytoskeletal arrangement and cell movement through downstream effectors ROCK and Rho, is also activated in the absence of TSC1 or TSC2. Various steps in this signaling pathway can be blocked by currently available agents, including selective estrogen antagonists, tyrosine kinase inhibitors, angiogenesis inhibitors, lymphangiogenesis inhibitors, farnesyl transferase inhibitors, statins, mTOR inhibitors, metalloproteinase inhibitors, and Rho inhibitors.
Rationale for choosing molecular and cellular targets in LAM
A growing body of evidence indicates that LAM is caused by mutations in either of the known tuberous sclerosis genes, TSC1 or TSC2, which have been shown to cause TSC (Fig. 1). 5 TSC1 and TSC2 encode hamartin and tuberin, respectively, which control cell growth, survival, and motility by forming a complex that regulates the activity of the mTOR (mammalian target of rapamycin) signaling pathway.6–8 The mTOR serine/threonine kinase is the catalytically active subunit of two functionally distinct protein complexes, mTORC1 and mTORC2. mTOR is a 'master switch' that integrates input from cellular systems that report on the status and environment of the cell, including signals arriving from cell surface growth factor receptors, oxygen sensors, nutrient sensors, hormones, and energy sensors. In the absence of hamartin or tuberin, mTORC1 is constitutively activated, and through downstream effectors pS6 and 4EBP1 drives inappropriate protein translation, cellular proliferation, migration, and invasion. Progression to frank malignancy is prevented by a pS6 feedback loop which inhibits the activity of IRS-1 and other upstream elements.9,10 Everolimus and sirolimus are two FDA-approved macrolides currently being tested in TSC and LAM trials (see below) which form a complex with a protein called FKBP12 and allosterically inhibit mTOR.
Some mTOR driven functions are rapamycin-insensitive, suggesting that combination therapies may be required for maximal effect. Direct kinase inhibitors such as Torin are more potent than the currently available mTOR inhibitors and are promising candidates for future trials.11,12 Inhibitors of many of the other signaling elements in the Akt pathway including PI3K, Akt, Rheb, and S6 kinase, are being developed for cancer and other indications. Estrogen is suspected to play a role in LAM disease initiation and/or progression, based on the profound gender restriction in LAM (although men also have significant amounts of circulating estrogen). Recent evidence suggests that estrogen can signal through Akt to release the hamartin- or tuberin-deficient cell from pS6-mediated feedback inhibition, and through MEK-dependent pathways to promote pulmonary metastasis by enhancing the survival of detached, tuberin-null cells. 13 Aromatase is an enzyme that can synthesize estrogen by converting testosterone to estradiol and androsteindione to estrone, and is the primary source of estrogen in postmenopausal women and in those with pharmacologically suppressed ovarian function. Multiple therapeutic strategies for the treatment of LAM are currently being considered based on the inhibition of estrogen production or estrogen action, with GnRh agonists, selective estrogen antagonists and aromatase inhibitors. Matrix metalloproteinase (MMP) imbalance involving MMP-2, MMP-9, and TIMP-3 has been described in LAM lesions and may contribute to cyst formation.14–16 A direct causal link for MMPs in the pathogenesis of lung destruction has not been established, however. In addition, trials of metalloproteinase inhibitors in cancer have shown no clinical efficacy, most likely because the MMPs are most important in the earliest stages of cancer pathogenesis such as early invasion and micrometastasis. 17 Two trials of doxycycline, a tetracycline family antibiotic with putative anti-MMP and anti-angiogenic activity, are currently underway in the United Kingdom and Australia. Genetic analysis of recurrent LAM lesions in the donor allografts of LAM patients who have undergone lung transplantation have revealed that LAM can metastasize; suggesting a novel mechanism for the disease.18,19 Potential strategies for intervention based on early resection of the primary tumor have been proposed, but the source of metastasis in LAM is controversial. 20 Two leading candidates have emerged, angiomyolipomas that are present in about 30% of sporadic LAM patients and 80% of TSC-LAM patients, and the uterus, which has been reported to harbor LAM lesions in multiple case reports. 21 Consistent with the metastatic theory, cells containing LOH for TSC genes have been isolated from the blood of LAM patients. 22 There is also compelling evidence for lymphatic dissemination in LAM, based on clinical and autopsy observations.23–25 Kumasaka et al. found that LAM cell clusters enveloped by lymphatic endothelial cells are abundant in the lymphatic lumen and populate chylous fluids and axial and supraclavicular lymph nodes in patients with LAM. 25 Abundant expression of lymphatic endothelial markers such as podoplanin, VEGFR-3, and VEGF-C within LAM lesions implicates inappropriate lymphangiogenesis in the pathogenesis of LAM. 26 VEGF-D, the ligand for VEGFR-3, is abundantly produced by LAM cells, and is elevated over three-fold in the serum of patients with LAM.27,28 In essence, LAM cells have adopted a strategy for spread which involves generating their own system of 'escape tunnels' through induction of lymphatic development. It is also quite likely that the cystic lung destruction that occurs in LAM is the result of relentless lymphatic remodeling by infiltrating LAM cells. Anti-lymphangiogenic approaches to LAM therapy, with VEGF-D antibodies or VEGFR-2/VEGFR-3 inhibitors, are under consideration. The unregulated growth, lymphatic or vascular spread, and tissue destruction 20 that are described above are entirely consistent with classification of LAM as a cancer. The benign histological appearance of LAM cells and very slow progression of the disease certainly place LAM at the far left in the neoplastic spectrum of severity, but the gradual recognition that LAM is a precious model of metastatic cancer due to a single gene mutation has begun to attract interest from the National Cancer Institute and other federal agencies.
Combined use of the cancer and signaling models in designing trials
The explosion in our understanding of the pathogenesis of LAM has provided a robust framework for identifying molecular targets for trials (Fig. 2). Opportunities for intervention suggested by adoption of the cancer paradigm include each of the putative stages of LAM pathogenesis of 1) somatic mutation, 2) proliferation, 3) lymphangiogenesis, 4) dissemination, 5) implantation, 6) infiltration, and 7) angiogenesis and remodeling. Knowledge of the signaling pathways that are deranged in LAM and their role in each of the cellular processes of growth, motility, angiogenesis/lymphangiogenesis, apoptosis, anoikis, and differentiation provides the tools to target each of the seven pathogenic stages above. The cancer model and the signaling models are complementary and should both be considered in choosing endpoints and designing trials.
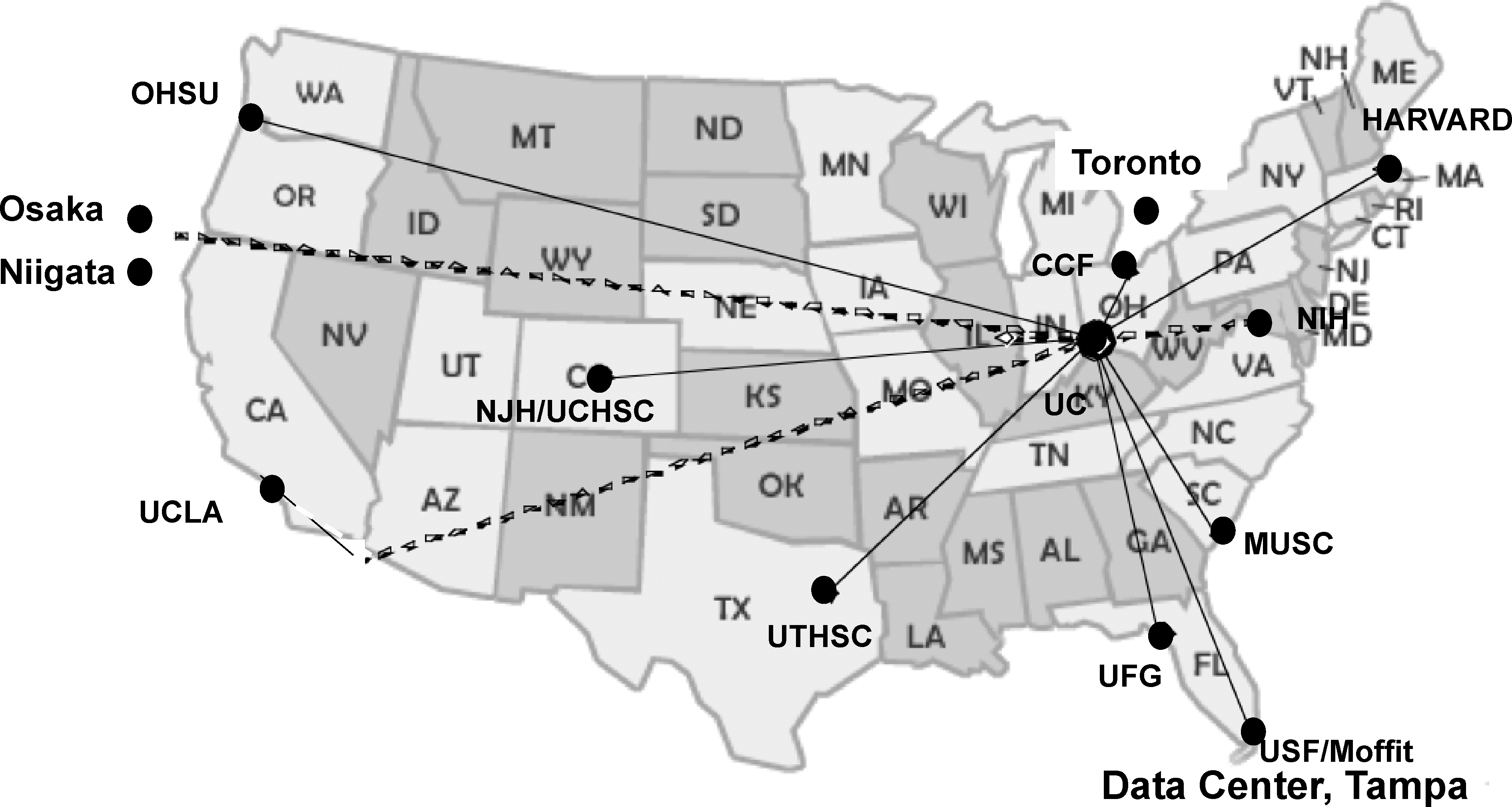
The MILES Trial is being conducted by the NCRR/NIH supported Rare Lung Disease Consortium. The Rare Lung Disease Consortium (RLDC) is composed of the primary site at the University of Cincinnati (co-Directors Bruce Trapnell, M.D. and Frank McCormack, M.D.), 9 other domestic sites, 3 international sites, and a Data and Technology Coordinating Center at the University of South Florida School of Medicine (Director, Jeff Kirscher, M.D.)
For instance, mTOR inhibitors target multiple pathogenic steps including proliferation, motility/dissemination, 29 angio/lymphangiogenesis,31,32 and anoikis/apoptosis, 32 and might be reasonable candidates for trials in which improvement in lung function (through tumor apoptosis and reduction of pulmonary interstitial infiltration) is the primary endpoint. On the other hand, a trial based on inhibition of metastasis by blocking MEK pathways may fail if the primary endpoint is lung function measurement, since a lung that is already extensively infiltrated with LAM cells may continue to deteriorate even if further metastases are interrupted. Finally, metalloproteinase inhibitors that block further cyst formation but perhaps not pulmonary parenchymal infiltration might slow the decline in lung function, but would not be predicted to result in a measurable improvement in lung function, gas exchange or exercise tolerance.
Choice of endpoints in LAM trials
Functional endpoints such as exercise tolerance, survival, dyspnea, and quality of life, are the most informative and important in lung disease trials since they have indisputable meaning for patients. Unfortunately, for LAM, these are also less practical endpoints for efficient trials. Six-minute walk testing is often not very sensitive to changes in functional status, since many LAM patients are young, otherwise healthy, and able to walk 1500–2000 feet despite severe structural pulmonary disease. On that background, detection of improvement is difficult or impossible. More formal exercise testing is expensive, labor intensive, not easily standardized, and often limited to specialized centers. Survival as an endpoint in LAM is also suboptimal, since the length of trials that would be required to answer questions of drug efficacy in a disease in which the average survival is in the range of 90% at 10 years is prohibitive. Quality of life, sense of dyspnea, and other questionnaire-based endpoints are valuable adjuncts, but are more subjective in nature and prone to bias, especially when making recommendations about potentially toxic therapies.
To circumvent the difficulties with these functional endpoints, surrogate endpoints of lung function measurements, biomarkers or structural and functional imaging may be considered. Unfortunately, none of these surrogate measures have been validated as a reliable predictor of survival or quality of life in LAM. Lung function measurements suffer from the inherent limitation of significant inter-test and intra-subject variability, as well as relative insensitivity to small changes in lung function. Serum biomarkers such as serum VEGF-D are just now being developed.27,28,33 Computed tomography-based measurement of cyst volume percent as a potential surrogate endpoint was recently reported. 34 There is an urgent need to develop serum or imaging based measures of lung and/or whole body LAM cell burden and validation of these and other biomarkers as surrogate endpoints for disease burden and survival.
Networks for LAM trials: The Rare Lung Disease Consortium and LAM Foundation Clinics
The MILES study was conducted under the auspices of the NIH/National Center for Research Resources (NCRR) Rare Lung Disease Consortium (RLDC), comprised of 13 sites distributed around the United States, in Canada and Japan, and a Data and Technology Coordinating Center (DTCC) in Florida 35 (Fig. 3). The concept behind the RLDC was that networks built for the purpose of trials in one rare disease could be used for multiple rare diseases and serial trials. The RLDC executed trials in LAM, alpha one antitrypsin deficiency, and pulmonary alveolar proteinosis, and has remained intact even as the RLDC funding from the NCRR has ended. Another novel, durable mechanism for conducting trials in rare diseases is to integrate clinical care and research at distributed centers. The LAM Foundation has recently opened LAM Clinics across the United States (Fig. 4). The objectives are to improve clinical outcomes in LAM and to organize the 800 North American LAM patients registered with the Foundation in a manner that facilitates the conduct of trials. LAM clinics are designed to provide state of the art, multidisciplinary care to LAM patients close to their homes. They also serve as incubators for expertise, in which pulmonary physicians, thoracic surgeons, nephrologists, interventional radiologists, and gynecologists become increasing familiar with LAM over time as patients accrue to their Clinic. LAM Clinics that are already open include University of Cincinnati, Columbia University, University of Pennsylvania, University of California Los Angeles, University of California San Francisco, Stanford, University of Michigan, Mayo Clinic, Cleveland Clinic, Tufts, and Medical University of South Carolina. A subset of LAM Clinics that have the interest, resources, and expertise to conduct clinical research, in conjunction with Dr. Joel Moss's program at the NHLBI, form the “LAM Clinic Research Network” (LCRN). The LCRN is focused to maintaining a population of LAM patients ‘at the ready’ for clinical trials, by gathering quality-controlled clinical and research data in a uniform fashion. In this model, patients see LAM experts in the clinics at defined intervals, perhaps every 6 months, for clinical care. During those visits, studies that are part of both clinical care and research trials, including pulmonary function tests and 6-minute walk distance, are obtained in a quality-controlled manner. When a trial becomes available, each patient enrolls with running baseline that can serve as her own control as the intervention is executed. This design lends itself to several efficient and rapid trial designs, including 'N of 1' trials discussed below. Over time, research funding from federal and nonfederal sources will be used for ongoing support of research coordinators, trial visits, and data management. A distributed network for conducting LAM trials has many advantages over the centralized ‘center of excellence’ model, in which patients must be well enough to travel, costs are high, and extent of disruption to work and family life limit enrollment.
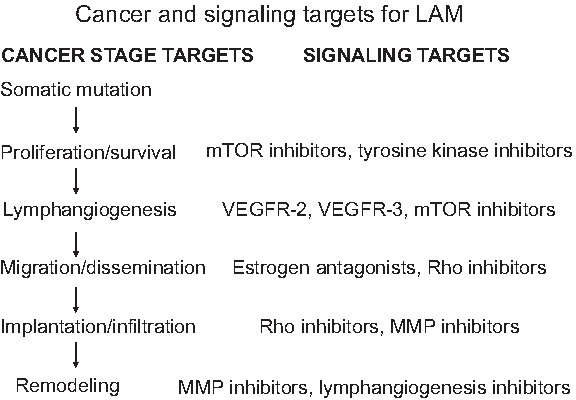
Choosing candidate trial therapies based on cancer staging targets and signaling targets in LAM. The model of LAM pathogenesis can be divided into six stages, which can be targeted by blocking signaling pathways and cellular processes involved in each step.

LAM Foundation Clinics.
International cooperation
In LAM, as with all rare diseases, international cooperation for clinical trials is critical. Patient populations ranging in size from 50 to 250 subjects are organized and ready for trials in the United Kingdom, Australia/New Zealand, Japan, France, Germany, Italy, Spain, Scandinavia, Brazil, and China. These concentrated populations are ideal for conducting phase I/II trials with the multiple candidate therapies that have been proposed for LAM. For phase III multicenter international trials, sponsorship by pharmaceutical companies is important. The burden of international regulations, the nuances of drug import/export, and language barriers make incorporation of international sites into investigator-initiated trials quite difficult.
Rationale for conducting early, staged LAM trials in humans
Given that there are no existing animal models of LAM that mimic the lung disease, in many cases the preferred approach to testing a promising therapy may be to bypass animal experimentation and proceed directly to human trials. This strategy is especially attractive for drug candidates with well-understood safety profiles that are already FDA-approved for other indications. Examples of drugs in this category would include mTOR inhibitors, statins, doxycycline, selective estrogen inhibitors, GnRH agonists, and aromatase inhibitors. Development of biomarkers that are faithful reporters of the burden of LAM cells or the stage of disease will greatly facilitate the conduct of rapid efficient trials that can identify the most promising candidates for larger multicenter trials. This staged approach of rapid, exploratory trials with biomarker endpoints in regionally concentrated populations, followed by multicenter, international, pivotal RCTs with functional endpoints is an attractive strategy for answering meaningful questions and for avoiding overlapping and conflicting trials in this small patient population.
Current LAM Trials
There are currently three categories of interventional trials for LAM underway; a) mTOR inhibitor trials targeting renal angiomyolipomas that include LAM patients, b) mTOR inhibitor treatment trials for LAM, and c) doxycycline trials for LAM.
Angiomyolipoma endpoint trials that include LAM patients
Lung function as primary endpoint trials
Doxycycline trials for LAM
Small trials in Australia and the United Kingdom (EUDRA CT registration 2007-003745-32) are underway to test the safety and efficacy of doxycycline in patients with LAM. Both studies are randomized, placebo controlled and 2 years in length. The primary endpoint in the UK trial is rate of decline in FEV1, the Australia trial cites multiple endpoints with none identified as primary.
General Principles on Study Design of Clinical Trials in Rare Diseases
Generally, clinical trial designs for rare diseases must meet the same rigorous standards as do designs for trials for diseases that occur with much higher frequency. 35 They should ask important scientific questions, reduce bias, and have a high likelihood of obtaining a scientifically acceptable answer. Study questions should be answered with the fewest number of enrolled subjects possible, irrespective of the number of subjects available, 35 and enrollment criteria should facilitate broad access and conclusions that can be generalized. However, there are several unique features and alternative study designs that may be considered particularly relevant for consideration in the study of rare diseases.
A randomized controlled trial is generally considered the gold standard in clinical research because intrinsic in its design is the minimization of the impact of confounding variables (both measured and unmeasured). Indeed, one of the main benefits of RCTs over observational studies is the equal allocation of important covariates between the intervention and control arms of a study, provided that there are sufficient numbers of study subjects. Thus, the results of RCTs are often considered as the strongest evidence in testing a hypothesis. However, RCTs are not easily performed and are costly (both time and resources). Recruitment of a sufficient number of patients can be particularly difficult in rare diseases, 38 leading to lengthy accrual periods. In addition, randomization requires that the investigator and the subject consider themselves in a state of equipoise (i.e., they believe that the treatment received from either arm of a randomized trial is equivalent unless proven otherwise). This is difficult for participants who want to believe that their treatment will be based upon what is best for them and not the ‘flip of a coin’, and difficult for physicians who also think that they are ethically bound to provide the ‘best’ treatment. Equipoise is also difficult since trials are often developed because an investigator feels that an experimental therapy is better and they wish to test that hypothesis in a rigorous fashion. 35 Many subjects are hesitant to enroll in trials if they have a likelihood of being assigned a potentially inferior arm (i.e., have a likelihood of not receiving the experimental therapy) or randomized to a placebo. Several study design techniques have been developed to attempt to address some of these difficulties in performance of classical RCTs.
A study design technique that increases efficiency and deals with the concerns of potential placebo treatment assignment is the use of concurrent controls in which participants can serve as their own control. Such designs are beneficial if there is less within patient variability in a treatment response than there is between-patient variability. 35 In such cases, outcome estimates will have less variance and the study design will require less accrual, leading to study efficiency. Some examples of designs that use concurrent controls include cross-over designs and “N-of-1” designs. These study designs do have certain caveats, however. Concurrent controls can only be used in situations where the following conditions are met: there is a relatively rapid response to the intervention; the response abates after the intervention is withdrawn, and the natural history of the severity of the disease does not change appreciably over the study time period. 35 These designs may work well for certain chronic diseases, but there are many situations in which the assumptions can not be justified.
In cross-over trials, participants are randomized to a treatment arm for a time period at the end of which the outcome is assessed and then the subjects are ‘crossed over’ to the other treatment. Cross-over designs use the same patients twice and effectively halve the number of patients that must be enrolled. ‘N-of-1’ designs use the same patients a number of times (generally up to 5) and are even more efficient. 35 Both the cross-over design and ‘N -of-1’ trials make the same assumption that a washout period is assumed to eliminate the effect of the treatment after the intervention is withdrawn.
Factorial designs are somewhat akin to cross-over designs with respect to increased study efficiency, but differ notably in that they involve a double randomization in which two questions are asked concurrently in the same participant study population. This is as if the investigators are conducting two simultaneous studies in the same patient population with an overall sample size savings of approximately 50% for both. This type of design assumes that there is no interaction between the two treatments (i.e., the biologic effect of the first intervention is not mediated or modified by the second intervention). Once again, this is assumption is often difficult to validate.
Summary: Future Trials in LAM
LAM is uniquely positioned for discovery through clinical trials. The molecular basis of the disease is well-studied and at least partially understood, a number of promising candidate therapies are already FDA approved for other indications and ready for testing, patients are generally young, well-informed, and motivated, and mechanisms to conduct geographically distributed trials are in place. For early phase trials where there is little available clinical evidence of efficacy, a study design that requires fewer subjects and can explore multiple interventions in a high throughput format such as open label phase II studies or the ‘N-of-1’ design is likely preferable. Interventions that show promise in these types of pilot studies should be followed with larger randomized controlled trials. For the later phase studies, consideration may also be given to study designs with increased efficiency (e.g., Factorial designs) so that the limited number of available study subjects can yield the most useful information. In addition, as individual therapies are shown to have an impact on disease course/outcome, there will likely be a need for well- designed studies of combination therapies akin to the chemotherapy model of cancer management.
In a population based survey of LAM patients regarding attitude toward participation in trials, the primary reasons cited for enrollment in clinical trials were access to information, access to the drug, closer monitoring and altruism toward other LAM patients. 39 The most frequent reasons given for not enrolling in trials were failure to meet the enrollment criteria, stable disease, and risks of side effects from the drug. Less often cited but still important reasons for not enrolling were inclusion of a placebo arm, access to the drug off label or through concurrent open label trials, fear of toxicity, and inconvenience or cost. These motivations for and against trial participation differ considerably from those of trials for more common diseases, and must be taken into account when designing trials. In so far as is possible, studies in rare disease should be designed to be as inclusive as possible, to take full advantage of the limited numbers of patients available, and to produce results that can be generalized to the population has a whole.
Footnotes
Author Disclosure Statement
Drs. Kinder and McCormack have no conflicts of interests or financial ties to disclose.