
Abstract
Abstract
Background:
The aim was to investigate the effect of patient position on the size of the cisterna chyli using positional MRI. The cisterna chyli is usually the only large lymphatic vessel that can be found on cross-sectional imaging. Not much is known about its postural behavior. However, animal studies suggest that the cisterna chyli varies in size according to physical activity.
Methods and Results:
Retrospectively, 998 MRI scans of patients referred for positional MRI were reviewed. Ten patients had acquired axial scans in at least two positions at the level T12/L1 or/and L1/2 and were included in the study. The area representing the cisterna chyli was assessed on axial images and its size was compared in different positions. The size of the cisterna chyli determined as the cross-sectional area was 14.7 mm2 ± 17.3 mm2 in the supine position, 43.8 mm2 ± 3.1 mm2 in the sitting position, and 62.9 mm2 ± 42.5 mm2 in the standing position. Using the t-test, a statistically significant difference was found in the size of the cistern chyli between supine and standing positions and between supine and sitting positions.
Conclusions:
The size of the cisterna chyli shows postural variations. This finding is discussed in regards to possible implications of interventional procedures in the thoracic duct. Physicians reading MR images acquired in positions other than supine should be aware of these physiological changes.
Introduction
Whereas several studies investigated the postural effect and flow in the peripheral lymphatic system, studies concerning lymph flow in the central lymphatic system are scarce, and missing in humans. 3 Studies in animals have demonstrated that physical activity leads to an increase of lymph flow in the thoracic duct. 4
Cross-sectional imaging is usually performed in the supine position. Positional MRI is a relatively new method of studying the spine in function under weight-bearing conditions, and dedicated scanners allow the examination of patients in supine and erect positions. 5
This study addresses the issue of whether the size of the human cisterna chyli varies between different body postures, especially between supine and erect positions.
Materials and Methods
A retrospective analysis of 998 MRI scans of the lumbar spine in patients presenting to our facility for weight-bearing MRI between October 2008 and November 2009 was performed. The weight-bearing MRI was indicated for various reasons, but most often for lumbago, spinal claudication, or sciatica.
Out of the 998 lumbar MRI scans acquired, the following patients were included in this study: all patients who underwent MRI scan either in the supine and sitting or supine and standing positions for whom axial images were available at level T12/L1 and/or L1/2 in both supine and weight-bearing positions.
Patients who presented with examinations in the supine position that had been performed less than 6 months previously with another scanner with axial slices available at level T12/L1 or L1/2 were also included in our study if axial slices were available at level T12/L1 or L1/2 in both supine and weight-bearing positions. Altogether 10 patients met the inclusion criteria.
Using the FONAR Upright MRI (Melville, NY), the following MRI sequences of the lumbar spine were acquired in the sitting position using a two-channel surface coil: sagittal T2-weighted scan (TE: 140, TR: 1445, matrix: 320 × 320 to 640 × 640, field of view: 36 × 36 cm), sagittal T1-weighted sequence (TE: 15, TR: 420, matrix: 320 × 320 to 640 × 640, field of view: 36 × 36 cm), axial T2-weighted sequence at level T12/L1 and/or L1/L2 (TE: 120, TR: 1245, matrix: 288 × 288 to 576 × 567, field of view: 20 × 20 cm), coronal STIR sequence (TE: 20, TR: 2528, TI: 95, matrix: 240 × 240 to 480 × 480, field of view: 36 × 36 cm).
In five patients, in the standing position a sagittal T2-weighted scan (TE: 140, TR: 1445, matrix: 256 × 256 to 512 × 512, field of view: 36 × 36 cm) and an axial T2-weighted sequence at level T12/L1 and/or L1/L2 (TE: 120, TR: 1245, matrix: 256 × 256 to 512 × 512, field of view: 20 × 20 cm) were acquired. In seven patients, the same parameters as in the standing position were used in the supine position; in three patients, a similar protocol had been performed prior to our examination in the supine position using other MRI systems. The time from the prior MRI to the scan in the weight-bearing condition was noted.
The images were digitally analyzed using picture archiving and viewing software (JiveX–Visus, Bochum, Germany). All images were analyzed by two senior radiologists.
On the axial images in the sitting and/or standing position, the image with the maximum size defined as cross-sectional area of the cisterna chyli was identified. The cisterna chyli was considered present if a fluid collection, isointense to cerebrospinal fluid, was found in the para-aortal retrocrural space, as defined previously. 1 In cases where the cisterna chyli could not be identified, the size was recorded as 0 mm2.
The area representing the cisterna chyli was measured in consensus by two experienced radiologists using tools in the picture archiving and viewing software. The size of the area was recorded in mm2. These measurements were performed in the supine position at the same level. All available adjacent images were visualized to rule out movement of the cisterna chyli.
The data were recorded onto a datasheet using Excel (Microsoft, Redmond, WA). Statistical analysis was performed on the data using an unpaired t-test. The hypothesis tested was that there would be no difference in the size of the cisterna chyli in different body positions. The hypothesis would be rejected with p < 0.05.
Results
Ten patients, four females and six males, mean age 59 years, were studied. None of these patients had a prior history of cancer and all were referred for problems related to degenerative disease of the lumbar spine. The patient characteristics are shown in Table 1.
Patient characteristics and findings for all patients (CC, cisterna chyli; n.a, not available). The size of the cisterna chyli is shown in supine, sitting, and standing positions. The last row shows the summary (see text).
The scans in the supine and erect positions were both performed on the same day in seven patients; in one patient each they were performed within 2 months, in another 4 months and 6 months, respectively.
The maximum size of the cisterna chyli was found at level T12 in two patients, at level L1 in three patients, and at level L2 in five patients. The location of the cisterna chyli in each individual patient was identical in all positions and the maximum size was found at the same location in all positions.
Axial images were available in all three positions for four patients, in the supine and standing positions for two patients, and in the supine and sitting positions for four patients.
The mean area of the cisterna chyli on the axial images in the supine position varied between 0 and 57 mm2 (mean: 14.7 mm2 ± 17.3 mm2); between 10 and 103 mm2 (mean: 43.8 ± 33.1 mm2) in the sitting position, and between 10 and 114 mm2 (mean: 62.9 mm2 ± 42.5 mm2) in the standing position. The size of the cisterna chyli displayed a great variability between the different patients. However, it was always smaller in the supine position as compared to the erect position.
Figures 1 and 2 clearly depict the postural change in size. In the coronal STIR sequence and adjacent axial images, the origin of the thoracic duct could be identified in all patients (Fig. 2). The thoracic duct could be followed in adjacent axial slices and in the STIR sequence (Fig. 3).

The postural effect on the cisterna chyli (arrows) is shown. On the left side, a sagittal and an axial T2-weighted image in the supine position are shown. On the right side, the same images are shown in the sitting position. Note the increase in size of the cisterna chyli in sitting position as compared to the supine position. The cisterna chyli is located identically in both positions. 50 × 44 mm (300 × 300 DPI).
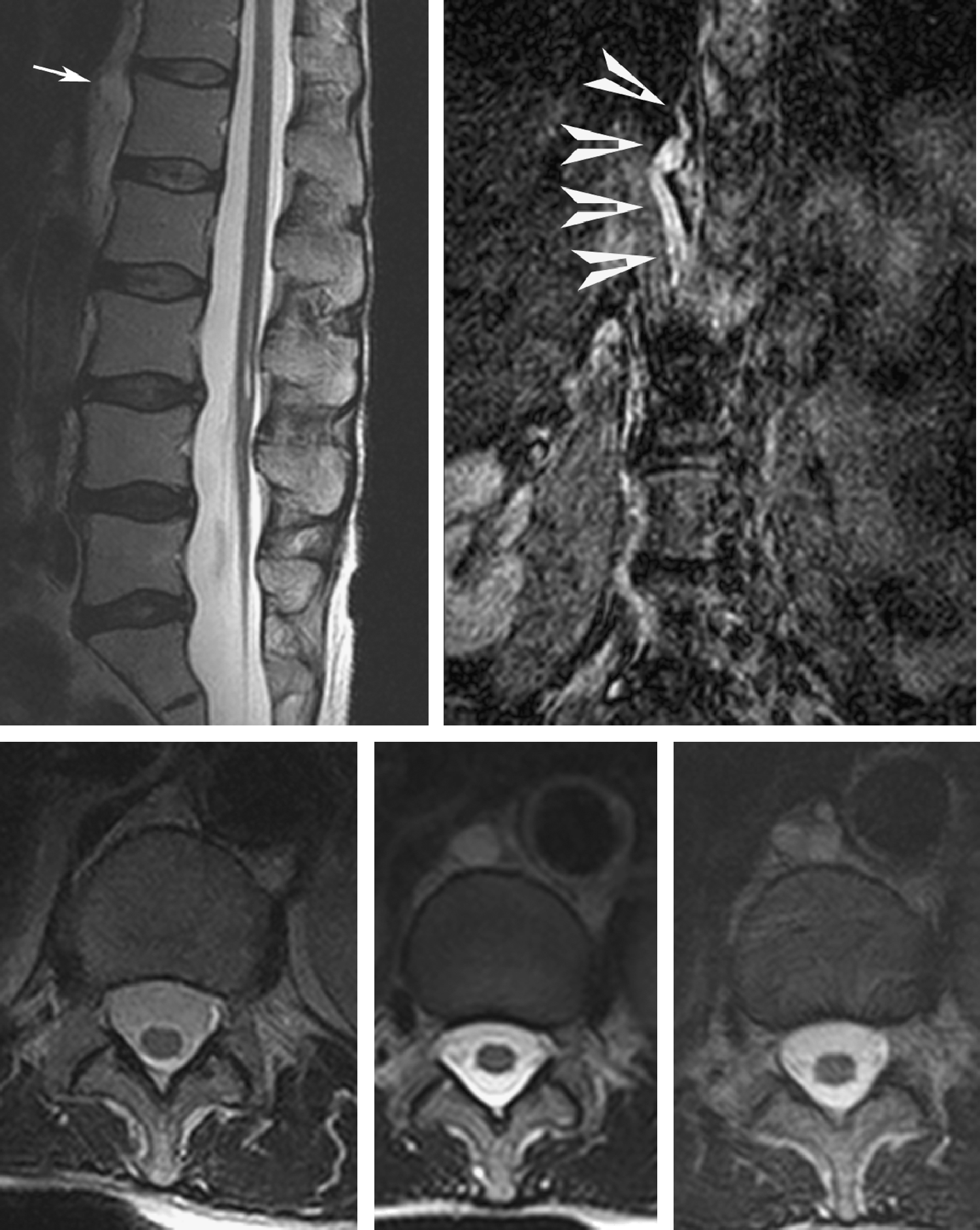
Postural effect on the cisterna chyli (arrows): Sagittal T2-weighted sequence (top left) and a coronal STIR sequence (top right), both in the sitting position. The cisterna chyli is prominent and the origin of the thoracic duct is visible on the STIR sequence (arrowheads). The bottom row shows, from left to right, axial images at the same level in supine, sitting, and standing positions. The cisterna chyli is not visible in the supine, but is well depicted in sitting and standing positions. Note the different configurations in the sitting and standing positions. This patient was investigated because of tethered cord syndrome, which is depicted on the sagittal image. 104 × 132 mm (300 × 300 DPI).
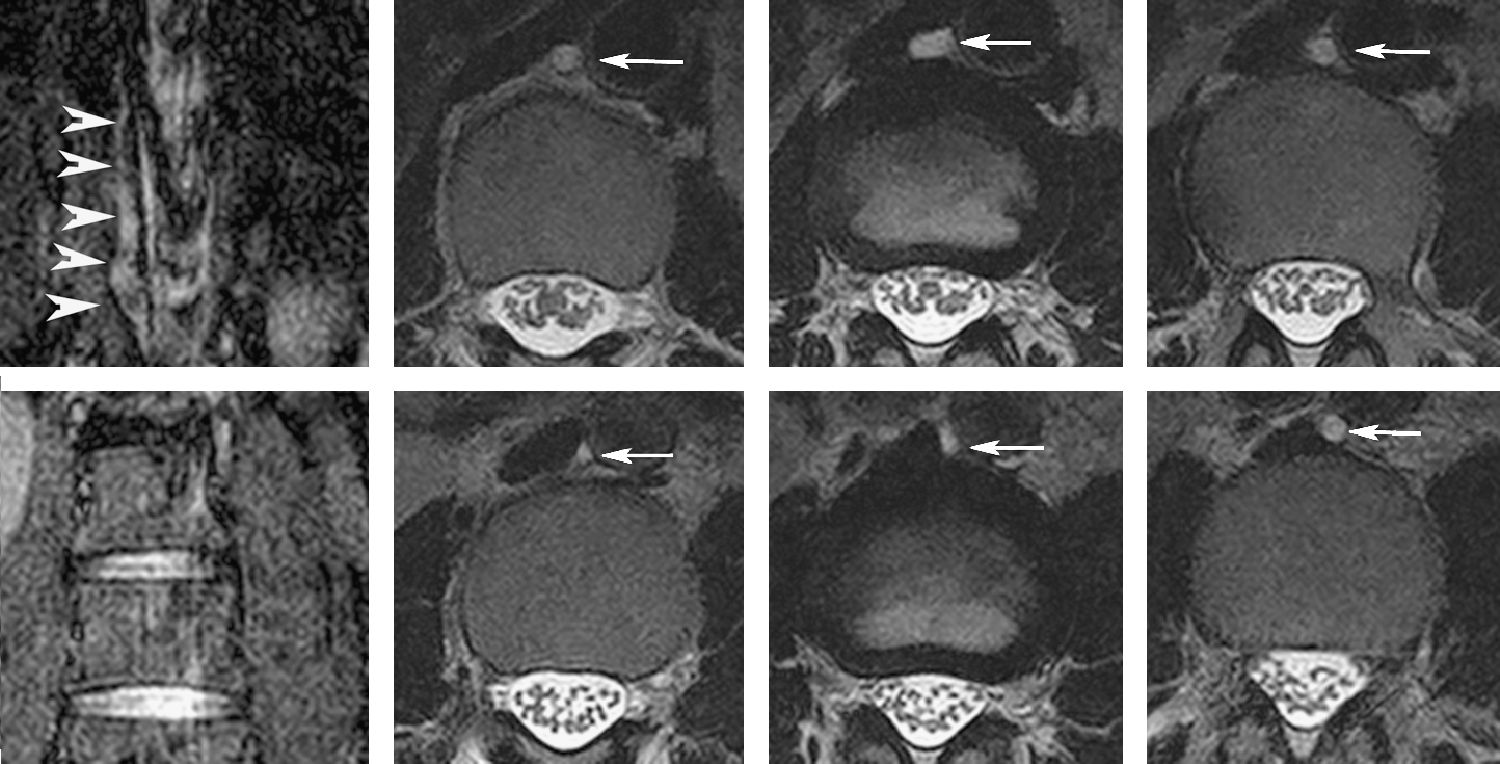
A coronal STIR sequence and axial T2-weighted images at different levels in the sitting position are shown. The distance covered by the T2-weighted images is 8.5 cm (T12 to L2). The thoracic duct and the cisterna chyli (arrows and arrowheads) are visible in all images at varying sizes. 184 × 94 mm (300 × 300 DPI).
The statistical analysis did not shown any significant difference between the size of cisterna chyli in the sitting and standing positions (p = 0.44), even though the configuration of the cisterna chyli varied between the different postures (Fig. 2).
A significant difference in size of the cisterna chyli was found between both the sitting and standing positions when compared to the supine position (p = 0.048 and p = 0.038, respectively).
Conclusions
The cisterna chyli, representing the origin of the thoracic duct, varies in location but is usually located ventrally of the eleventh thoracic vertebra to the second lumbar vertebra between the aorta and the cava vein. The lymph from the lower extremity and the digestive systems drains through the cisterna chyli into the thoracic duct. 8 It is the only part of the lymphatic system that can be seen on cross-sectional imaging and it displays a large variance. It is found in about 15%–20% of patients on CT examinations, and in up to 50% of patients on lymphangiography.1,2
The largest study, which included 3000 patients, showed a cisterna chyli diameter of 6.1 mm in 11.6 % of the patients without history of cancer. 2 Recalculating the diameter into an area of a hypothetical circle, the area of such a circle would correspond to 29 mm2. This finding is concordant with our own results (21 ± 17.2 mm2).
We could show that there is a postural variation in size between the supine and erect positions; however, there is no significant variation between the sitting and standing position. There was no postural variation in the location of the cisterna chyli.
Several clinical implications can be discussed from our findings: Percutaneous embolization of the thoracic duct using the cisterna chyli as access route has recently become an interventional radiological procedure employed in patients with recurrent chylothorax or chylous ascites.6,7,9 After direct puncture of the cisterna chyli or thoracic duct, embolization using coils, clues or particles is performed. The technical success rate was reported as 73.8% 10 in a large study which included partial treatment response to the procedure. The most often encountered problem was difficulty in catheterizing the thoracic duct.
In patients undergoing such a procedure, different body positioning to increase the size of the cisterna chyli and thus facilitate the puncture might be difficult due to co-morbidities in these patients. In case the puncture of the cisterna chyli fails in the recumbent position, tilting the treatment table might yield an increase in volume of the cisterna chyli and hence facilitate puncture after opacification of the cisterna chyli using lymphography. It is unclear, however, if the size of the cisterna chyli changes the same way in patients with lymphatic vascular disease, such as chylothorax, compared to healthy subjects. Due to lymph leakage, the change in size of the cisterna chyli might be less pronounced or absent.
Our findings showed that the cisterna chyli, and hence the distal part of the thoracic duct, are elastic vessels. Occlusion of the thoracic duct, especially with coils, might only be temporal due to the elasticity of the vessel, hence explaining why no lymphedemas of the lower extremities have been reported after such procedures. Temporal occlusion, however, may be sufficient to treat recurrent chylous ascites or chylothorax.
The depiction of the cisterna chyli on cross-sectional imaging has triggered several reports about normal anatomical findings and variances potentially due to malignant diseases.11,12 Since the cisterna chyli is more prominent on CT or MRI exams performed in either the sitting or standing positions, physicians interpreting images acquired in these positions must be aware of the physiological changes occurring in the cisterna chyli.
Besides making a contribution to the study of central lymphatic system physiology, the findings are of interest to radiologists and surgeons alike because of the increasing number of interventions in the thoracic duct and the cisterna chyli.6,7 An increased knowledge of the physiology of the central part of the lymphatic system might be beneficial in facilitating access and increasing patient safety, especially during percutaneous procedures.
Footnotes
Author Disclosure Statement
Pascal Niggemann, Andreas Förg, Dieter Grosskurth, and Hans–Konrad Beyer have no conflicts of interest or financial ties to disclose.