
Abstract
Abstract
Background:
Breast cancer-related lymphedema in the arm is commonly detected by bioelectrical impedance spectroscopy as an increased inter-arm impedance ratio due to the presence of excess lymph in the at-risk arm relative to that of the unaffected arm. The presence of lymphedema is determined by a value of this ratio greater than the mean ratio, plus three standard deviations observed in a comparable healthy population. This threshold value has not been established using the measurement protocols in current practice. The aim of the present study was to determine the reference range of the inter-arm impedance ratio to allow a cut-off value to be established as a criterion for the detection of breast cancer-related lymphedema.
Methods:
The mean and variation (3 SD) of the inter-arm impedance ratio for the arms of 172 healthy female control participants were determined from an accumulated database of impedance data obtained using present generation impedance instrumentation and methodology. This reference range and threshold value was compared to the original threshold ratio determined a decade ago but still in current use.
Results:
The presence of lymphedema is indicated when the impedance ratio exceeded 1.106 when the nondominant limb is at risk, and 1.134 when the dominant limb is at risk compared with the currently used values of 1.066 and 1.139, respectively. Although the difference in these values was statistically significant, this difference was determined to be of minor importance to clinical practice.
Conclusions:
The impedance ratio thresholds for early detection of lymphedema remain suitable for clinical use with present day bioimpedance spectroscopy analyzers and measurement protocols.
Introduction
Bioelectrical impedance analysis is the measurement of the opposition (impedance) to the flow of a harmless electric current through a body region. The magnitude of the impedance is inversely related to the volume of the conductive material (tissue water) in the measured region (Equation 1):
where V is volume, L is conductor length and ρ is the specific resistivity of the conductor. 6
The current is applied through EKG-style gel electrodes attached to the skin spanning the body (i.e., on the dorsal surface of the hand and foot) so that the current flows through the region of interest. Two additional electrodes are placed to span the region of interest and detect the impedance to the flow of current. The original protocol for measuring BCRL of the arm was to place one of these electrodes at the wrist and the second 40 cm proximally along the arm; this pair of electrodes thereby measuring a 40-cm segment of the arm. Thus, while a segment of identical length was measured in all subjects, in people of different body sizes, and hence arm lengths, this however encompasses different proportions of the whole arm. The currently recommended protocol obviates this difficulty by placing the proximal electrode on the opposite wrist, which according to the principle of equipotentials 5 is electrically equivalent to a point in the region of the axilla, that is, the whole arm. Mirroring these electrode positions on the contralateral arm measures the equivalent body region facilitating direct comparison of the two arms. The original reference data were collected using the original paired electrode approach.
The term bioelectrical impedance analysis or BIA strictly refers to the measurement of impedance at a single fixed frequency of applied current. Impedance is conventionally denoted by Z while electrical resistance is denoted by R, both with units of ohm. At zero and infinite frequencies, resistance and impedance are identical and hence R = Z. For the purposes of this report, the terms impedance and resistance at these frequencies are used interchangeably. The preferred impedance method for lymphedema assessment is bioimpedance spectroscopy (BIS). BIS measures the impedance over a range of applied frequencies and uses data modeling to predict the impedance at zero and infinite frequencies that cannot be measured directly. The path that an electric current takes through biological tissues is frequency dependent such that the impedance at zero frequency (R0) is that of the extracellular water (ECW) compartment only while the impedance at infinite frequency (R∞) is that of total tissue water. Thus, the impedance at zero frequency is a measure of the ECW volume, including lymph. Since impedance is inversely related to volume as lymph accumulates, R0 decreases proportionately (Equation 1).
The absolute measured impedance of a limb cannot discriminate, however, between an affected limb (i.e., one with excess lymph) and an unaffected normal limb, owing to the wide biological variation between individuals in impedance values. The impedance of a limb with, or at risk of developing, lymphedema is therefore normalized to that of the contralateral unaffected limb, and this ratio is then compared to normative values.
As with all measurement techniques, BIS is not error-free and the errors in estimation of R0 and R∞ are dependent upon the performance of the electronic measuring apparatus and the data modeling (curve fitting) procedures used to estimate these parameters from the actual measured data.7,8 Impedance devices currently commercially available are electronically superior to the older devices used to gather existing reference data and data analytically techniques are now more sophisticated, implying greater precision and accuracy in the determination of R0 and R∞.
The purpose of the present study was to determine the normal variation in R0 and R∞, and their ratio, in the limbs of a cross-section of a healthy population measured with a current model impedance device according to the method of equipotentials, and with data analyzed using commercially available data analytic software purpose designed for this BIS analysis.
Methods
Participants
Data for healthy control participants were retrospectively drawn from a database of impedance data maintained at The University of Queensland. The participants had all been recruited for a variety of research studies being undertaken by the authors over the period 2005–2010. Participants were all volunteers and were recruited from the greater Brisbane or Sydney regions. All contributing studies had received the appropriate approvals of the University Medical Research Ethics Committee and written informed consent to participate in the study was obtained.
All participants were weighed using digital scales, to the nearest 0.1 kg, and their height measured, to the nearest 0.1 cm, using a wall or stand-mounted stadiometer. All participants were asked to state their arm and leg dominance. Self-ascribed health status was verified by interview with the researchers. Inclusion and exclusion criteria for entry into the studies were broad: subjects were excluded if fitted with a pacemaker, were pregnant, taking diuretic medication, or recently undertaken activities that may have markedly altered their hydration status (e.g., extreme physical exercise). Participants were not required to fast overnight. A total of 172 women were identified in the database as having the required impedance data recorded. The women were aged 44.2 ± 18.1 (mean ± SD) years (range, 18.3 to 86.0 years); weighed 65.1 ± 13.4 kg (range, 40.4 kg to 119.0 kg); had a height of 164 ± 7.1 cm (range, 142.1 to 184.0 cm); and had a body mass index (BMI) of 24.2 ± 4.5 (range, 16.1 to 46.0 kg m2).
Measurement of limb impedance
The impedance of the arms of all participants was measured according to methods described in detail elsewhere.6–8 Briefly, whole limb impedance (wrist to axilla) was determined according to the principle of equipotentials 5 while the participant lay supine on a nonconductive examination couch, arms by their side and slightly abducted from the body. All jewelry, except rings on fingers, was removed, and the skin at the electrode sites cleaned with an alcohol wipe prior to the application of Ag-AgCl gel electrodes. The electrode locations were those recommended by the manufacturer (i.e., current drive electrodes on the dorsal surface of the third metacarpal of the hand and the dorsal surface of the third metatarsal of the foot and the voltage sensing electrodes on the dorsum of the wrists midway between the styloid processes and the dorsal surface of the ankle midway between the malleoli).
Impedance data were obtained with two different impedance instruments, either an SFB3 (frequency range 5–1024 kHz) or SFB7(3–1000 kHz) frequency scanning bioimpedance spectrometer (Impedimed Ltd., Brisbane, Australia). Small, <2.5%, but significant differences in estimated R0 and R∞ values between the SFB3 and SFB7 instruments have been determined when both are tested on participants or electronic test circuits. 9 Therefore, all SFB3 data were converted to equivalent SFB7 data using the conversion factors provided by Ward. 10
Data processing and analysis
Data from both instruments were analyzed according to Cole theory, 11 using the manufacturer's software (Bioimp version 4.8.0.0, Impedimed Ltd.), to provide values for R0 and R∞. Generally, the default program settings were used for analyses; however, for some data sets, the analysis was optimized by adjustment of the frequency “window” used for fitting the data to the Cole model guided by minimizing the standard error of the estimate (SEE) for the curve fitting procedure. 9 The SEE for all analyses was <1%.
The resistance of intracellular water (ICW), Ri, was calculated from the relationship (Equation 2):
Statistical analysis
Bioimpedance characteristics, including R0, R∞, and Ri group data, were expressed as means ± SD or %SD. Frequency distributions were determined using MedCalc version 11.3.3.0 (MedCalc Software bvba, Mariakerke) and normality plots using Sigmastat version 3.5 (Systat Software Inc, Chicago). Normal distributions for both the participant data set and the current reference data 2 were calculated from the mean and standard deviations using an Excel spreadsheet (Vertex42 Software, Vertex42.com Accessed June 29, 2010). Significance of difference between the distribution of R0 ratios in the current population and the current reference data 2 was determined using group t test for mean and SD.
The threshold inter-limb R0 ratio, indicative of the presence of lymphedema, was set at the conventional value of the mean ratio + 3 SD value observed in the control population. The practical clinical importance of a difference in this threshold value between the current and the new threshold was assessed by a reanalysis of the original data of Ward et al. 12 to determine whether the application of the threshold altered the classification of patients with lymphedema.
Results
The impedance values of the arms and their ratios are presented in Table 1. The raw impedances (R0, R∞, and Ri) of the dominant arms were all significantly decreased (P < 0.0001) compared to those of the nondominant arms, reflecting the asymmetry in arm size due to dominance. The variance in the values seen in the population varied with the impedance parameter being measured but varied from approximately 12 %SD for R0 to 27 %SD for Ri. The larger %SDs for R∞ and Ri reflect the larger error associated with determination of R∞ 9 and inflation of the combined errors associated with determination of R0 and R∞ when calculating Ri by Equation 2. The mean and standard deviation for the inter-arm ratio of R0 (dominant: nondominant) was 0.986 ± 0.040 which was significantly different (group t test; P < 0.0004) from the value published by Cornish et al. 2 of 0.964 ± 0.034. The %SD for this ratio observed in the present study (4.1%) was slightly greater than that observed by Cornish et al. (3.5%). 2
Significance of difference between arms determined by paired t test.
The inter-arm impedance ratios were normally distributed, as indicated by the close agreement of the cumulative frequency distribution to a straight line 13 (Fig. 1A), justifying the use of as SD as a variation descriptor, and fitted a normal distribution (Fig. 1B). The fitted normal distribution for the data of Cornish et al. 2 is also presented for comparison. The threshold criterion indicative of lymphedema, set at the mean + 3 SD, was 1.106 compared to 1.066 for Cornish et al. (Fig. 2).
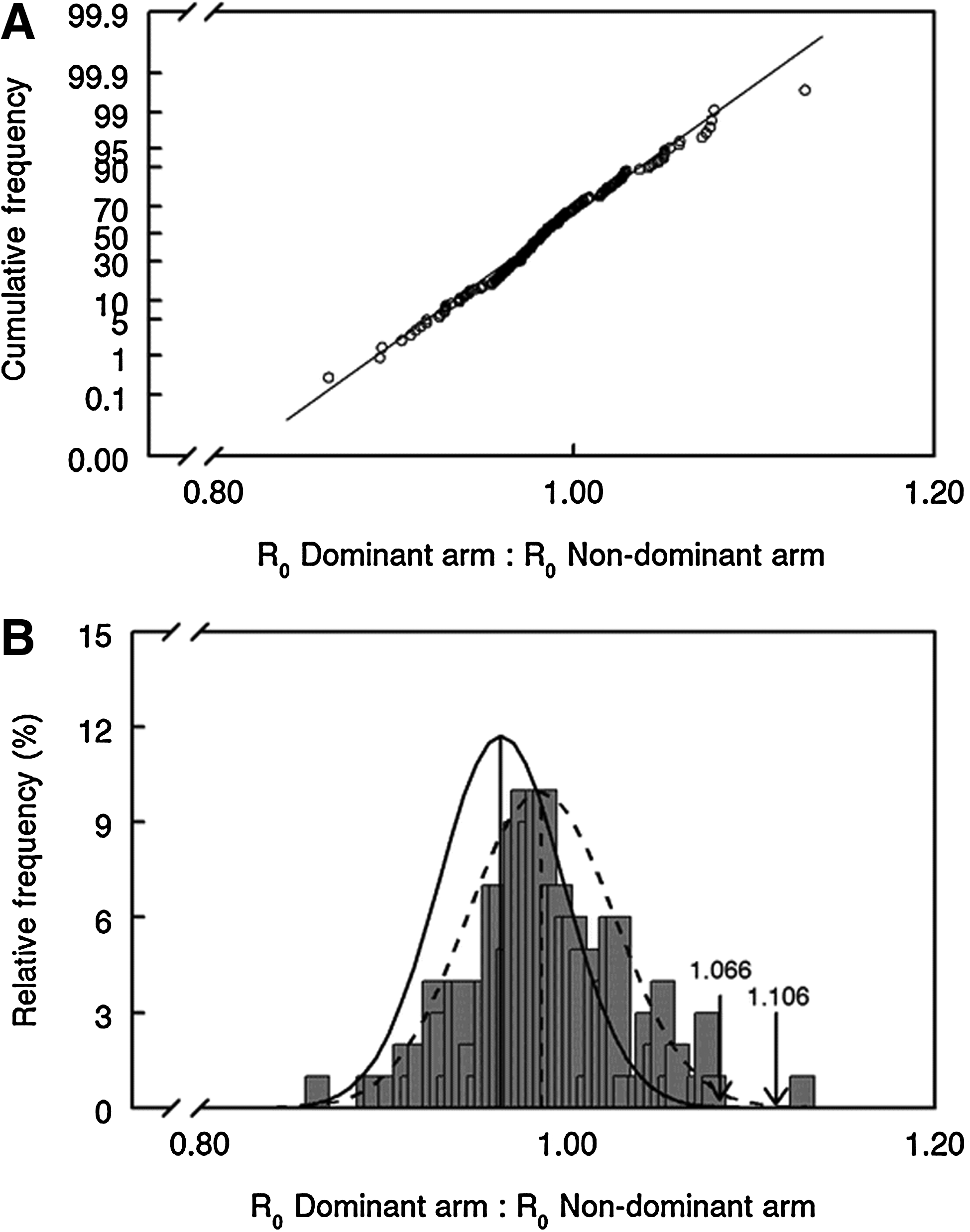
Frequency distribution of ratio of R0 between arms in of control female participants. Ratios calculated as dominant:nondominant arm.
Discussion
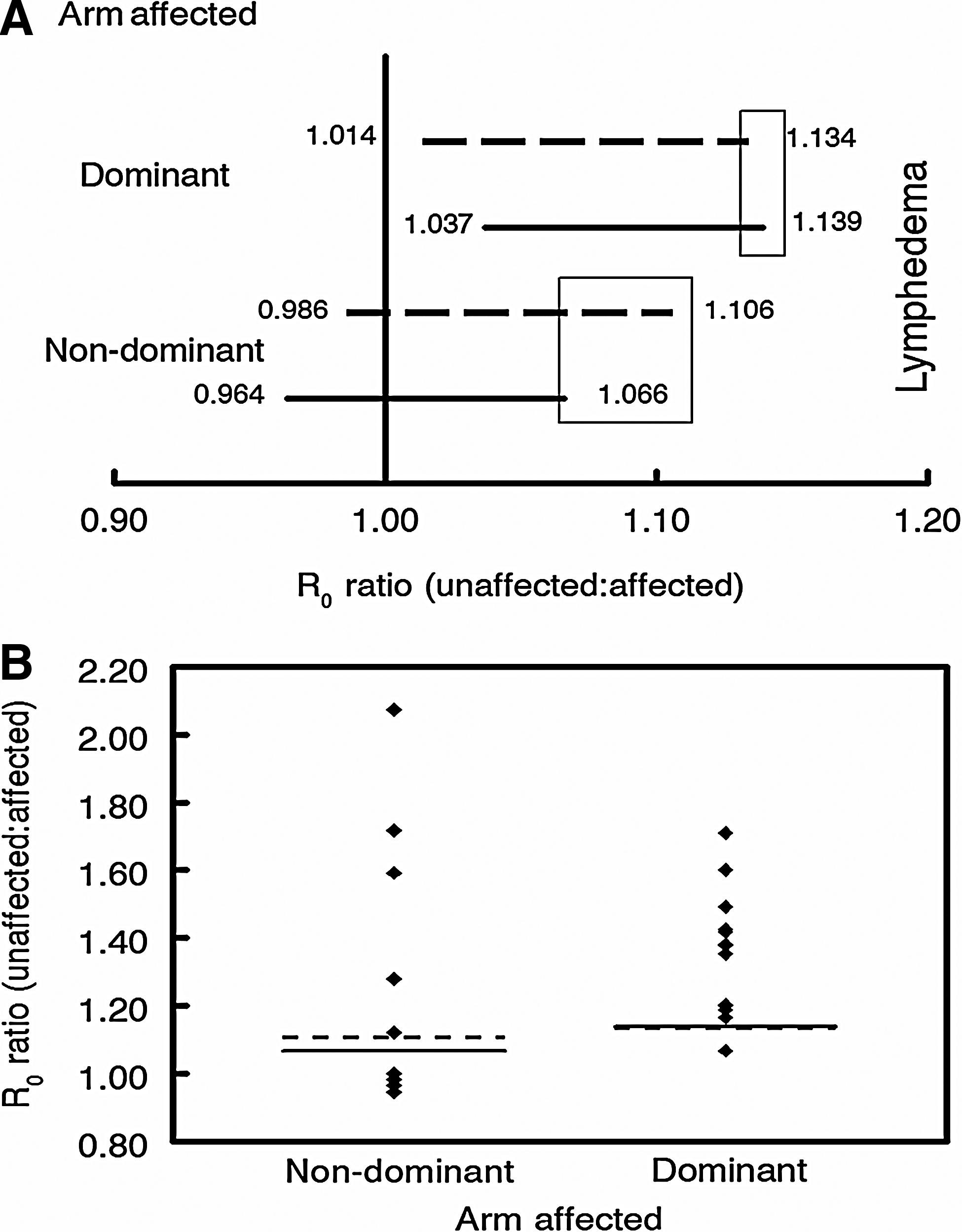
The present study has determined BIS ratios for the assessment of BCRL using present day impedance devices, measurement protocols, and data analytical techniques. The criteria ratios are similar to but, nonetheless, significantly different to those originally determined. This raises the question as to the practical clinical significance of this difference. A comparison of the new and current reference criteria is presented in Figure 2A. Three points are worthy of note. First, the mean values for the new ratios are closer to unity than the current reference values (i.e., less asymmetry between arms). With the much larger sample size (n = 172) and wider range in ages (18.3–86.0 years) in the present study versus those of Cornish et al. 2 (n = 60 and 27–84 years), it is possible that this represents a better reflection of true difference in normal healthy population. It is noteworthy that in a small group of subjects (n = 28), coincidentally, an identical ratio value to that determined here (0.986) was found by Ridner et al. 14 Second, the variation observed in the ratios within the present population is larger (4.1 %SD for the present study versus 3.5 %SD for that of Cornish et al. 2 and 2.7 %SD for the study of Ridner et al. 14 ). Third, and correspondingly, the threshold criteria presumptive of the presence of lymphedema differ, indicated by the boxes (Fig. 2A). This provides a region of diagnostic uncertainty depending upon which reference criteria are used.
In an attempt to assess the practical importance of this difference in threshold values, a set of existing data 12 were classified according to both sets of criteria (Fig. 2B). The adoption of the new criteria did not alter the classification of these subjects as to the presence of lymphedema. As described previously, 12 five subjects were consistently classified by both sets of criteria as not having lymphedema despite this being clinically confirmed. This may be due to the lymphedema being highly localized in a discrete segment of the arm for which a whole arm impedance measurement is less sensitive 15 or the presence of fibrosis which may not be detectable by BIS which measures the electrically conductive water space of the extracellular compartment.
The choice of the mean + 3 SD as the criterion value may be questioned as being too conservative compared to a criterion of the mean + 2 SD more common in diagnostic testing. This threshold value was originally proposed by Cornish et al. 2 but without supporting explanation for its choice. Its use in the present study was based upon this historical precedent. Furthermore, this criterion has been widely adopted by others, for example, Ridner et al. 14 It should be noted that, while this cut-off may be deemed conservative, Cornish et al. observed a sensitivity of 100% with 98% specificity in their study of BCRL when using this criterion, observations supported by others (e.g., Hayes et al. 16 and discussed in detail elsewhere 17 ). These studies attest to the clinical utility of a criterion of the mean + 3 SD.
The new criterion was determined from a retrospective analysis of data not specifically collected for this purpose. Nonetheless, identical protocols, and identical to those used in lymphedema assessment, were used in all studies, thereby providing comparable impedance data. However, it is acknowledged that the opportunistic use of an existing dataset provided no opportunity to ensure that the sample was matched for subject characteristics such as age, height, weight, or ethnicity to that of a typical population of women with BCRL. Nevertheless, since all of the subjects in the studies included in the dataset were randomly recruited from the population with few exclusion criteria (other than being healthy), they may be considered to be representative of the general healthy population.
No attempt has been made to derive criteria for subgroups of the population, for example, the elderly or the obese. The control data set was not considered sufficiently large to provide adequate numbers of subjects in the population subgroups of interest. This should be a focus for further research since the size of the extracellular water compartment measured by R0 is known to be affected by factors such as age 18 and obesity. 19
In summary, new criterion thresholds for the assessment of BCRL by BIS have been determined. Although statistically different to the established reference values, the magnitude of the difference is sufficiently small to be of no practical clinical consequence. It is concluded that, in accord with the observations of Ridner et al., 14 the present reference thresholds may be used with confidence as markers for lymphedema.
Footnotes
Acknowledgment
Dr. Ward conceived the study, undertook data collection and analysis and primary responsibility for manuscript preparation; Dr. Isenring undertook subject recruitment and data collection at Queensland University of Technology and contributed to manuscript preparation; Drs. Czerniec and Dylke undertook subject recruitment and data collection at University of Sydney, data analysis and contributed to manuscript preparation; Dr. Kilbreath undertook data analysis and contributed to manuscript preparation.
The willing participation of the participants is gratefully acknowledged. The assistance of Kendall Sharpe, Simon Van Rosendal, Jennifer Bengston and Julia Dyer in collecting control data is gratefully acknowledged.
Author Disclosure Statement
Dr. Ward has consulted to ImpediMed Ltd. ImpediMed Ltd. had no involvement in the conception and execution of this study or in the preparation of the manuscript.
These studies were funded, in part, by a research grants from the National Health and Medical Research Council of Australia, National Breast Cancer Foundation and ImpediMed Ltd.