
Abstract
Abstract
Background:
The aim of this article is to illustrate the possible applications of 18F-fluorodeoxyglucose positron emission tomography/computer tomography (18F-FDG PET/CT) in chronic extremity lymphedema and its complications.
Methods and Results:
18F-FDG PET/CT findings in a rare case of Stewart–Treves Syndrome (STS), angiosarcoma secondary to chronic extremity lymphedema, are presented. Lymphedema of the extremities is a debilitating disease characterized by chronic swelling due to interstitial edema caused by insufficient lymphatic drainage capacity. Progression with skin thickening, subcutaneous fibrosis, and increased adipose tissue volume is common. Chronic inflammation has been suggested as a key pathophysiologic component. STS is a rare complication with a very poor prognosis; however, early diagnosis and radical treatment is associated with increased survival. Thus, accurate pretreatment staging is paramount. 18F-FDG PET/CT is highly sensitive in detecting increased glucose metabolism as seen in many types of cancer and inflammation. The role of 18F-FDG PET/CT in the management of lymphedema and its complications has to our knowledge yet to be described. This case documents high 18F-FDG uptake in STS, but is at the same time an example of the low specificity of this imaging modality.
Conclusions:
We suggest that 18F-FDG PET/CT has the potential to become an important tool in the staging and treatment planning of Stewart–Treves syndrome. Furthermore, 18F-FDG-accumulation may be a sensitive tool in detecting low grade inflammation in the skin and subcutis, which has been suggested to cause tissue remodeling in lymphedema progression. However, further studies are needed to elucidate this theory.
Introduction
A rare but often fatal complication of lymphedema is Stewart–Treves syndrome (STS), which is defined as the development of a highly malignant angiosarcoma secondary to chronic lymphedema. 14
The uptake of 18F-FDG is a measure of tissue carbohydrate metabolism and is visualized by PET/CT scanning. 18F-FDG PET/CT has been demonstrated to be a very sensitive tool in detecting inflammation and many neoplasms.15,16 The role of 18F-FDG PET/CT in the management of lymphedema and its complications has to our knowledge yet to be elucidated. Future possible applications are illustrated by the following case report.
Case Report
A 44-year-old woman with known lymphoscintigraphy-verified lymphedema (Fig. 1) presented with newly developed macular skin changes in the affected lower left extremity (Fig. 2). The patient had acquired secondary lymphedema 6 years earlier following repeated surgery for an intrapelvic carcinoma of unknown origin involving resection of the sigmoid colon and multiple retroperitoneal lymph nodes. An initial histological skin biopsy showed no signs of malignancy. The symptoms were interpreted as cellulitis, but repeated treatments with antibiotics had no effect. In the months prior to admission, the lymphedema progressed rapidly, resulting in a total weight gain of approximately 35 kilograms. The skin changes progressed and ulceration and clinical signs of cellulitis developed. The patient was admitted for optimized compression treatment and intravenous antibiotics.
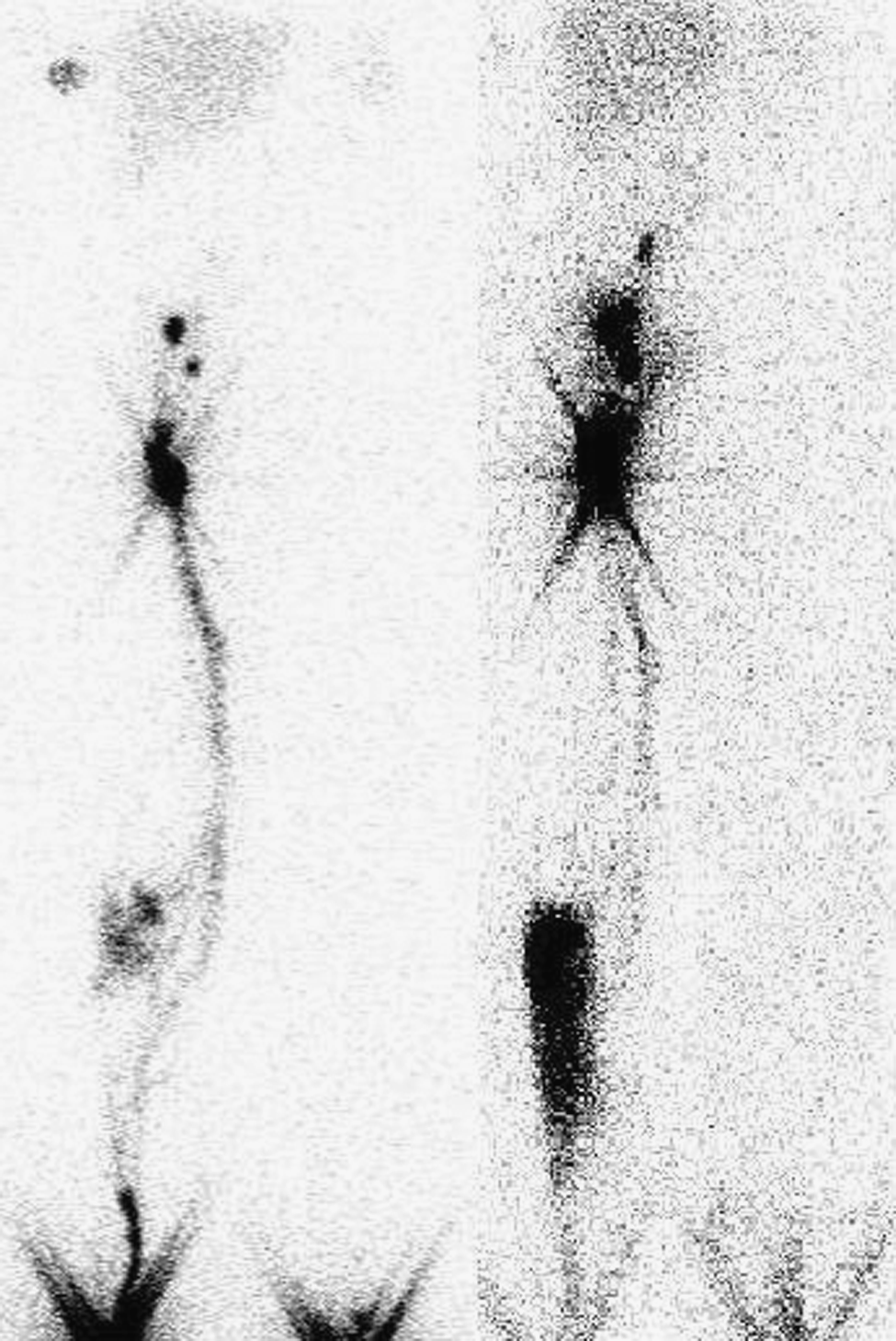
99mTc-nanocolloid lymphoscintigraphy showing no visualization of subcutaneous lymphatic collectors or lymph nodes in the affected lower left extremity on either the early (15 min post injection, left) or the late scan (120 min post injection, right). In the lower right extremity, there are signs of tracer leakage from subcutaneous lymphatic collectors at knee level.

Clinical photograph at admission showing macular skin lesions in the affected lower left extremity.
Among a host of different diagnostic examinations to determine the cause of the sudden edema progression, a 18F-FDG PET/CT scan was performed to rule out recurrence of the intrapelvic neoplasm (Fig. 3). The scan showed massive edema of the subcutaneous tissue of the lower left extremity and surprisingly a pronounced 18F-FDG accumulation primarily in the skin and subcutaneous tissue, with sharp demarcation at the ankle and groin level. There was no evidence of intrapelvic tumor recurrence. In spite of large treatment efforts to treat the cellulitis and reduce the edema (compression, elevation, loop-diuretics, broad spectrum antibiotics), the patient's condition continued to deteriorate over the following weeks with treatment refractory edema and progressive ulceration (Fig. 4). A second 18F-FDG PET/CT scan was performed 6 weeks later to make sure a neoplasm was not overlooked due to the massive FDG accumulation in the affected leg on the first scan (Fig. 5). It showed a marked decrease in overall 18F-FDG-uptake, however, multiple focal lesions in the skin and subcutaneous tissue remained. A histologic skin biopsy was repeated due to the lack of treatment effect and the diagnosis of angiosarcoma was made. The general condition of the patient was too poor to offer surgery or chemotherapy and she died shortly thereafter due to the massive tumor burden, infection, and kidney failure.
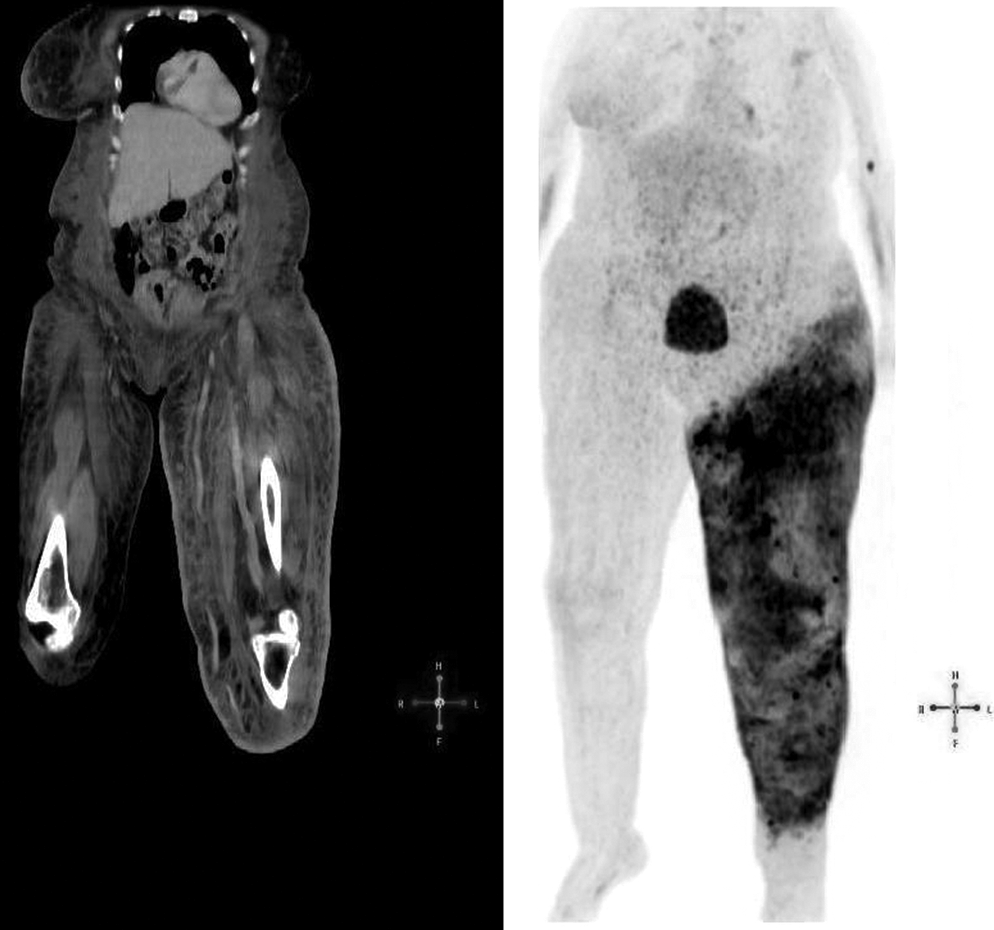
18F-FDG PET/CT showing massive subcutaneous edema (left) and increased 18F-FDG uptake in the skin and subcutaneous tissue with unusual sharp demarcations (right) in the affected lower left extremity.

Clinical photograph approximately 8 weeks after admission showing extensive progression of skin lesions.

The second 18F-FDG PET/CT 6 weeks later showing a decrease in edema volume and soft tissue 18F-FDG accumulation compared to the first scan, but multifocal lesions with increased 18F-FDG uptake in the skin and subcutaneous tissue in the lower left extremity remain.
Discussion
The case report described above represents an example of the possible applications of 18F-FDG PET/CT in chronic extremity lymphedema and its complications. Lymphedema is a chronic progressive disease but the speed of progression is very individual. It is, however, generally accepted that conservative treatment with manual lymphatic drainage massage, compression therapy, and meticulous skin care results in a better outcome. 17 The pathophysiologic mechanisms governing skin and subcutaneous tissue remodeling in extremity lymphedema have yet to be fully elucidated. If chronic inflammation plays a central role, then the degree of inflammation may be associated with the progression speed. 18F-FDG PET/CT scanning has been shown to be a very sensitive modality in the diagnosis of focal inflammatory processes. 15 We suggest that 18F-FDG PET/CT can become an important tool in identifying the patients at risk of tissue remodelling progression.
STS is a rare and often fatal complication to chronic lymphedema with an estimated incidence in breast cancer-related lymphedema (BCRL) of 0.07% –0.45%. 18 The average debut of STS in BCRL is 10 years after mastectomy and the prognosis is poor with a median survival of 19 months. In lower extremity lymphedema, STS is even rarer but seems to have a later debut (average 19 years) and perhaps a slightly better prognosis (median survival 34 months). 19
Local extensive spread via satellite lesions and metastasis to the lungs are common. 18 Early diagnosis and radical surgical treatment is associated with a better prognosis. 19 Thus pretreatment staging is paramount in choosing the correct treatment modality. 18F-FDG PET/CT has the potential to become a first line choice in initial staging and treatment follow-up because STS has been demonstrated to have a high 18F-FDG uptake.20–22
This case furthermore represents one of the possible pitfalls in applying 18F-FDG PET/CT on lymphedema patients. In the first scan, the STS changes were masked by the inflammation caused by the present cellulitis. The STS changes first became evident after the cellulitis had been sufficiently treated. Since 18F-FDG accumulate in all cells with a high glucose metabolism such as some forms of cancer cells and activated immune cells, the modality has a low specificity under circumstances where infection and malignancies are present concomitantly. 15
Footnotes
Author Disclosure Statement
No competing financial interests exist.