
Abstract
Abstract
Background:
Arm lymphedema is routinely assessed by clinicians and researchers, using arm circumference measurements. A protocol was developed for measuring arm circumference independent of medically trained professionals. The aim of this project was to assess the protocol's inter-rater reliability and its coherence with perometry measures.
Methods and Results:
Community-dwelling adults (n = 57), aged 60.2 ± 12.8 years, in good general health, were included in this study. Circumference of both arms were measured at the ulnar styloid of the wrist and at four 10 cm intervals up the arm by a friend of the participant, as well as the trained assessor using a tape measure. The same measures were also obtained with a perometer. The assessment tools had moderate to high concordance (rc = 0.84–0.94 for assessor vs. perometer and rc = 0.68–0.93 for assessor vs. participant). Limits of agreement analysis revealed that the mean difference between methods varied based on the measurement location; the bias ranged from −5.5% to 1.5% for assessor-measured vs. perometer methods and from −2.4% to 4.0% for assessor-measured vs. participant-measured methods.
Conclusions:
The written instructions and cartoons are reliable tools that could be used by women at risk of lymphedema as well as those with lymphedema following treatment for breast cancer to measure their arm circumference reliably independent of medically trained personnel.
Introduction
Clinically, arm circumference measures are the most commonly used approach to identify and monitor lymphedema. 5 Typically, measurements taken of the ‘at risk’ limb are compared to the same measurements of the ‘not at risk’ limb. These measures are taken with a tape measure and are typically carried out at standardized points along the arm. These measurements commence at the ulnar styloid of the wrist and are followed by more proximal locations at set intervals. 6 Perometry is less frequently used but provides the same information. The optoelectronic perometer records the limb dimensions every 5 mm, 7 whereas arm circumference measures may only be made every few centimeters. Both tools are highly reliable, but the perometer has been proposed to be more accurate for measuring arm volume than those based on arm circumference measures.8,9
As part of a larger project, a protocol was developed to instruct community dwelling older adults, without a medical background or a history of breast cancer, to perform arm circumference measurements with the help of a friend or family member. The protocol included instructions and descriptive cartoons (Appendix 1) to enable participants to measure their arms reliably. The aim of this study was to determine the reliability with which women could undertake this process. Specifically, we compared the accuracy of the measures obtained from the participants' friend or family to those obtained by trained researchers, and by the perometer. Confirmation of the reliability of this tool will enable it to be used to follow up patients and participants over time without the requirement of a trained individual performing the measures.
Materials and Methods
Study design and recruitment
This cross-sectional study was approved by the Human Research Ethics Committee of the University of Sydney (Reference Number 12923) and all the participants provided a written consent before commencing the study. Participants were recruited from June to October 2010 by inviting past research participants who had indicated willingness to take part in future studies, and by word-of-mouth.
Community-dwelling older adults (n = 57) over the age of 40 years in good general health were recruited. The participants were included if they were able to comprehend English, able to give consent, and could attend one 45-minute assessment session. The exclusion criteria included disorders of the nervous system disrupting voluntary movement, severe functional limitation, breast cancer, arm lymphedema, or cognitive impairment. Characteristics of the participants enrolled in this study are presented in Table 1.
N = 57, except for mass and BMI where n = 56.
Mean (±Standard deviation).
Adapted from World Health Organization (WHO) 1995, WHO 2000, and WHO 2004.
BMI, body mass index.
Protocol
A letter of invitation, participant information statement, and consent form were mailed or given to each volunteer. They also were provided with a measurement package that contained an instruction sheet on how to measure arm circumference and a form on which to enter the data. Participants were requested to have the circumference of their arms measured by a nonmedically trained friend or a family member. They were encouraged to submit an electronic version of the data sheet to the study assessor if they had access to the internet and had a valid email address.
Following the completion of the home measurements, the participants attended one session in which assessment of their arm was undertaken by a trained study assessor using a tape measure and the perometer. This appointment was made within a 2-week period of the home assessment.
Arm circumference using a tape measure
Instructions for measuring the circumference of both arms using a retractable Jobst nonstretch tape measure were provided to all participants. The instructions required participants to measure the circumference at the wrist, and 10, 20, 30, and 40 cm proximal to the wrist. Written instructions were supplemented with cartoons illustrating each step (Appendix). Briefly, participants were seated with their arm extended in forward flexion. This is the same protocol used by research assistants in our laboratory to routinely measure arm circumferences. 10
Arm circumference using an optoelectronic perometer
An optoelectronic perometer (Perometer 350S, Pero-system GmbH, Wupertal, Germany) was used to obtain limb circumference measures. 11 The perometer consists of a movable frame positioned at 90° above a horizontal base plate. This frame contains rows of infrared light emitters on two sides at right angles to each other which project light toward rows of light sensors on opposite sides. 11 When a limb is placed in the measuring frame, it blocks the transmission of light creating a shadow. As the measuring frame is moved along the longitudinal axis of the limb, vertical and horizontal limb diameters are recorded every 5 mm. 11
Participants were asked to wear sleeveless tops. They were seated, and were asked to hold their arm horizontally at shoulder height (at 90 degree abduction, palm down) with their elbow extended inside the movable frame and their middle finger touching the end of the hand rest. An assessor slid the metal frame towards the participant's shoulder, and then back towards the hand. Measurements were performed on both arms. The frame did not touch the participant's arm at any stage of the measurement.
All participants were assessed once, as the perometer has been reported to have an excellent reliability and reproducibility with repeated measure.10–12 The perometer data were exported into a spreadsheet and were determined manually from the Peroplus software™. According to a previously published method, 5 circumferences were determined for the ulnar styloid and at the 10, 20, 30, and 40 cm proximal to the ulnar styloid.
Other characteristics
Demographic characteristics, medical history, current medication, and arm dominance were recorded. All the physical measurements were undertaken in a single session by a trained assessor. Body mass index was calculated from height and weight measures.
Statistical analysis
A sample size of 50 people has been reported to be sufficient to assess reliability at the level of 0.8 over two measurement occasions.13,14 The data were expressed as mean and standard deviation (SD) or median and range after being tested for normality (skewness −1 ≥ 1). Lin's concordance correlation 15 and limits of agreement analysis were used to determine the concordance of arm measures derived from those obtained by the participants with the two sets of measures obtained within the laboratory environment. The dominant arm was used for analysis. For ambidextrous participants, the right arm was considered as the dominant arm. Statistical calculations were carried out using IBM SPSS (Release 19.0 for Windows, 2010, Chicago: SPSS Inc) and statistical significance was assumed at α level of P < 0.05.
Results
A medium to high degree of concordance was observed between the arm circumferences measured by participants' untrained friend or family members and those measured by the assessor (Table 2; Fig 1). The concordance for the arm circumference measures ranged from rc = 0.68 for arm circumference at 10 cm to rc = 0.94 for measures at 20 cm. The concordance between the arm circumferences measured by the assessor and those measured by the perometer ranged from rc = 0.83 for the 10 cm measure to rc = 0.94 for 40 cm measure. In contrast, the concordance between the measures organized by the participant and those of the perometer ranged from rc = 0.76 for the 20 cm measure to rc = 0.93 for 10 cm measure.
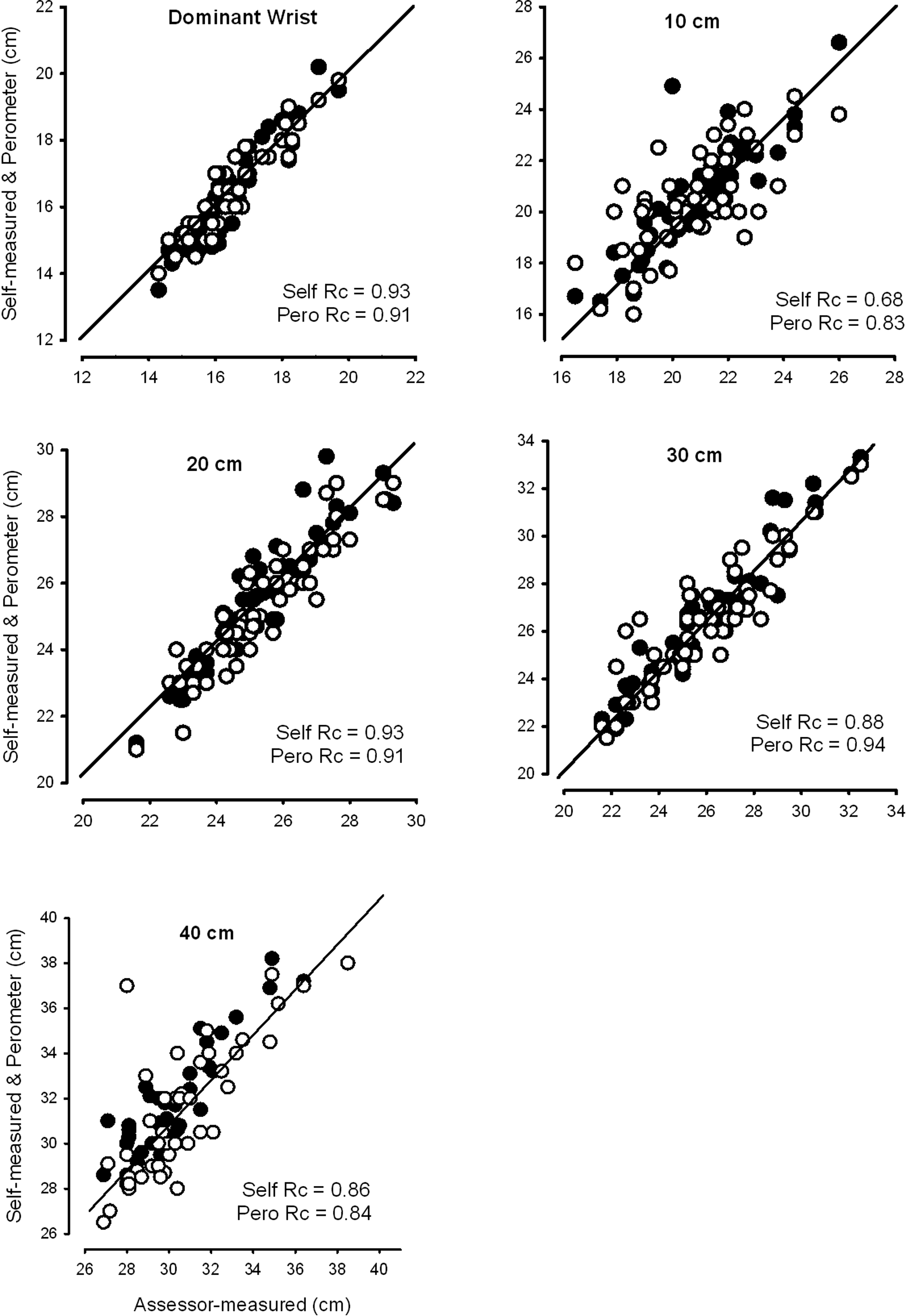
Concordance of arm circumference at 10 cm intervals between assessor-measured and participant-measured (closed circles) and between assessor-measured and perometer (open circles). The line of identity between the two measures is represented by the solid diagonal line.
N = 57, except for perometer where n = 55.
Right arm assumed as dominant limb for ambidextrous participants.
The bias between methods was minimal and varied based on the measured arm point. The bias ranged from −5.5% at 40 cm to 1.5% at 10 cm for measures taken by an assessor compared to those from the perometer and from −2.4% at 40 cm to 4.0% at the ulnar styloid for measures taken by assessor compared to those organized by the participant. The mean values measured at each point are presented in Table 3.
N = 57, except for perometer where n = 55.
Values of the right arm reported for ambidextrous participants.
Mean (±Standard deviation).
Discussion and Conclusion
There was a moderate to high agreement in measuring arm circumference between the measures taken by participants' friends and relatives, research assistants, and perometer at all arm points. Interestingly, the point which had the least reliability and concordance with the perometer was 10 cm proximal to the wrist. This is the part of the forearm which progressively increases in width. Slight variation in starting point at the wrist could have a significant effect on circumference, thereby contributing to only moderate reliability.
Detailed instructions and cartoons resulted in moderate to high reliability of measures of arm circumference. However, measurements obtained from the participants were as reliable as arm circumference measures undertaken by experts. Reliability and concordance between two expert measures has been shown to be consistently very high for arm circumference measures.8,16,17 Interestingly, even though there is excellent reliability with arm circumference measures from experts, Devoogdt et al. 18 employed a measurement device to assist in standardized locations along the arm. They used a stainless steel bar on which a tapeline was fixed at every 4 cm distance. The arm circumference was measured at the olecranon and 4 cm proximal and distal of the olecranon. High intra-rater and inter-rater reliability (ICC range: 0.942–0.998) was found, leading those authors to conclude that these arm circumference measurements could be obtained accurately and quickly using their cost efficient device. 18 Use of arm circumference measures to derive volume also demonstrates much higher reliability. Czerniec et al. 10 , using the protocols described in the current study, reported high intra-rater reliability for derived arm volume (ICC2,1: 0.98 (0.97–0.99)). Thus, more structured approaches with experts or tools does result in better reliability.
Overall, if resources are available, using an expert to measure arm circumference is the preferred option. However, in many instances, this is not feasible as ‘at risk’ women do not have access to experts to measure their arm. In this instance, self monitoring using the instructions in Appendix 1 would be an option. In the current study, women were provided with the written instructions only. The reliability, and particularly for the point 10 cm proximal to the ulnar styloid, might be further improved by reviewing the instructions, particularly the starting point, with ‘at risk’ women prior to usage. At this time, it could also be emphasized for women to recheck their measurements to see if any discrepancies between the two sides are logical.
The option was given to participants to submit their data sheet electronically; however, none chose to use this approach as they were physically coming to the research laboratory for the second part of the study. Measurement and electronic submission of data could be an area of further exploration.
In conclusion, self monitoring using the instructions and cartoons provides a cost-efficient, user-friendly tool for ‘at risk’ patients to measure their arm circumference and to identify possible lymphedema post cancer treatment. These instructions may also be beneficial in the conduct of the longitudinal cohort studies where measurement of arm circumference becomes costly and time consuming.
Footnotes
Acknowledgments
The authors acknowledge the valuable time of volunteers devoted to this project.
Author Disclosure Statement
No part of this work has been published anywhere else and there is no commercial, financial, or personal relationship with other people or organizations that could inappropriately influence this work. The typescript has been read and agreed by all authors. This study was conducted under no conflict of interest. No competing financial interests exist.