
Abstract
Abstract
Secondary lymphedema is a common complication after lymph node excision and radiotherapy in cancer therapy. Therapies are limited to symptomatic treatment. Adequate animal models to test potential surgical therapies are needed. The aim of this study was to induce a tissue environment in the hind leg of the rat similar to the one found in operated and irradiated patients. Quantification of edematous swelling was performed by an automatic 3D-contour segmentation (ITK- Snap ©) on MR- images. Swelling was induced by excision of superficial inguinal and popliteal lymph nodes and adjacent lymphatic vessels, followed by radiotherapy of the right groin with a single dose of 15 Gy. Four weeks after irradiation, the animals were examined with MRI of both hind legs. Fluid volumes around the joint line of the knee were calculated on T2-weighted images. We documented a significant higher volume of fluid in the legs following excision of lymph nodes and lymphatic vessels, combined with radiotherapy than in control legs.
Introduction
Impairment of lymphatic drainage leads to fluid congestion and accumulation of macromolecules and cells in the interstitium, a condition known as lymphedema. Primary lymphedema is uncommon. These cases can be idiopathic or hereditary (such as Milroy's disease, where a mutation in the VEGF-R3 gene has been demonstrated in some affected individuals 3 ).
Secondary lymphedema has numerous potential causes. It can result from bacterial or parasitic infections (e.g., filariasis 4 ) or can be posttraumatic. In industrial countries, secondary lymphedema most commonly represents a consequence of lymph node resection and/or radiation in cancer therapy.
The incidence of secondary lymphedema after breast cancer treatment is estimated to be 30%, and an estimated 20% of patients develop lymphedema after lymphadenectomy in the therapy of cervical cancer or melanoma of the extremities. 5
Lymphedema is most often a lifelong condition. Therapy is directed at palliation of symptoms and consists of regular manual lymph drainage, use of compression garments and, in many cases, intermittent pump therapy. Surgical techniques intended to be curative have been proposed but long-term efficacy is poorly documented.
To facilitate the development of newer surgical techniques, such as avascular lymph node transplantation, there is a need for adequate animal models to permit quantification of lymphedema and its responsiveness to different treatment modalities. Hadamitzky et al. summarized present models. 6 There are models for secondary lymphedema established in the tail of the mouse 7 and the rabbit's ear. 8 These models are helpful for molecular studies but they are unsuitable for clinical settings. A combination of radiotherapy and excision of lymph nodes and lymphatic vessels is suitable to induce lymphedema in rodents9,10 and dogs. 11 In these publications single doses of 30 and 45 Gy in the rat and 12 Gy in dogs are described to induce lymphedema.
In previous studies we analyzed several single doses of radiotherapy and varying timing of experiments. Radiotherapy followed by excision of the lymph nodes and vessels leads to surgical hemorrhage and higher complication rates in wound healing. Randomized examination of single doses of 12, 15 and 18 Gy did not lead to significant differences; thus, a single dose of 15 Gy was chosen for this study.
Quantification of edema in in vivo small animal models like the rat is difficult. In human clinical studies, water displacement, perometer measurements, and circumference- based techniques have been proposed as suitable techniques.12, 13 In the mouse tail model, serial water displacement analysis lead to high measurement variability within the same tail. 14 perometers are not available for experiments with rodents and circumference- based measurements are also very highly variable. Digital photography has been used as a reproducible method to analyse edema volumes in the mouse tail. 14
Tammela et al. recently published an edema model in the forelimb of the mouse. After excision of axillary lymph nodes, they demonstrated swelling in the subcutaneous space of the operated mice in T2- weighted MRI pictures. 15 Slices showing the paw were examined, hand calculated on each slice, and summated for quantification. Imaging of lymphedema by T2- weighted MRI has previously been documented as a suitable method in human studies. 16
Area quantification of various regions in the brain by a user- guided 3D segmentation on MRI pictures with an open source medical imaging segmentation tool for ITK-SNAP (http://www.itksnap.org/) has been described and successfully implemented.17–19
In previous studies we have investigated the regeneration of avascular transplanted lymph nodes as a surgical approach to the prevention or treatment of lymphedema. In healthy rats, avascular transplanted lymph node fragments are able to reorganize into lymph nodes. Regeneration can be improved by platelet-rich plasma 20 and VEGF-C (unpublished observations). However, in order to examine the effects of a successful transplantation on the extent of edema, a suitable lymphedema model is necessary.
The aim of the present study was to create a technique to quantify edema in the rat hindlimb, to facilitate future study of such interventions as avascular transplanted lymph node fragments on the volume of lymphedema, and to improve quantification of edema volumes on MRI-pictures by using an automatic segmentation tool.
Material and Methods
The experimental procedure was reviewed and authorized by the local authorities. The study population comprised 12 female Lewis rats (approximately 200 g). Full anaesthesia was performed by using Isoflurane (Baxter Deutschland GmbH, Unterschleißheim, Germany). Postoperative analgesia was obtained by application of Carprofen (2,5mg/kg s.c. Rimadyl, Pfizer GmbH, Karlsruhe, Germany) for three days after intervention.
All animals were first subjected to an extirpation of the superficial inguinal lymph nodes, the popliteal lymph nodes, and adjacent lymphatic vessels of the right hindleg under visual control.
One week after surgery the animals were irradiated in the right groin with 6 MV photons by a Primus Linear Accelerator (Siemens Healthcare, Erlangen, Germany) with a single dose of 15 Gray. For this intervention, the animals were fixed in supine position on a purpose-built board having an elevation dorsal to the hip to obtain a plane surface in the groin for radiation (Fig. 1). Full anesthesia was induced by intraperitoneal injection of ketamine (90 mg/kg; Albrecht GmbH, Aulendorf, Germany) and medetotomin hydrochloride (0,25mg/kg; Pfizer GmbH, Karlsruhe, Germany).
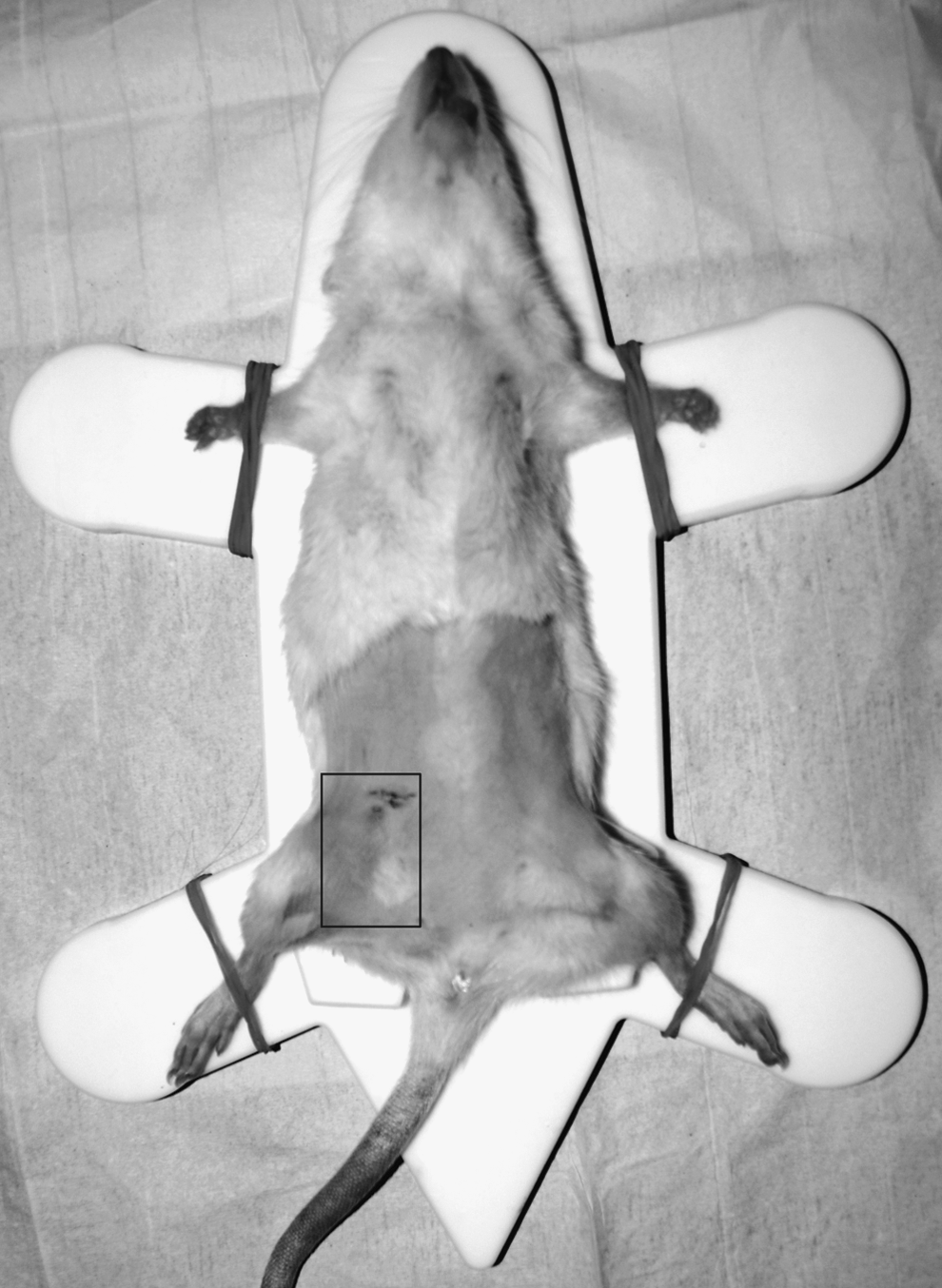
Position of the rat for radiotherapy and irradiated area in the groin (box).
Four weeks after radiotherapy the animals were examined by MRI. Magnetic resonance imaging was performed on a 7T Bruker Pharmascan 70/16 (Bruker Biospin, Ettlingen, Germany). With a 16 cm horizontal bore magnet and a 9 cm (inner diameter) shielded gradient, 1H-resonance-frequency of 300 MHz and a maximum gradient strength of 300 mT/m. Data acquisition and immediate image processing was completed with Bruker software Paravision 5.0. A rat whole body resonator (72 mm linear Volumeresonator/Transmissioncoil) was used as a transmitter and receiver coil (FOV 6×7 cm). Axial multislice T2 weighted RARE images (repetition time TR=5500 ms, echo time TE=40 ms, FA=180) and diffusion weighted (TR=4000 ms, TE=27 ms, FA=90) were acquired.
A dedicated two-animal bed (Fig. 2) with masks for gas anesthesia (Isofluran, Baxter Deutschland GmbH), temperature controlled warming blankets and Small Animal Monitoring System (Model 1025; SA Instruments, Inc.) equipped for control of respiration rate, ECG, temperature as well as ECG and respiration triggering was used. After the examinations the animals were sacrificed by cervical dislocation.
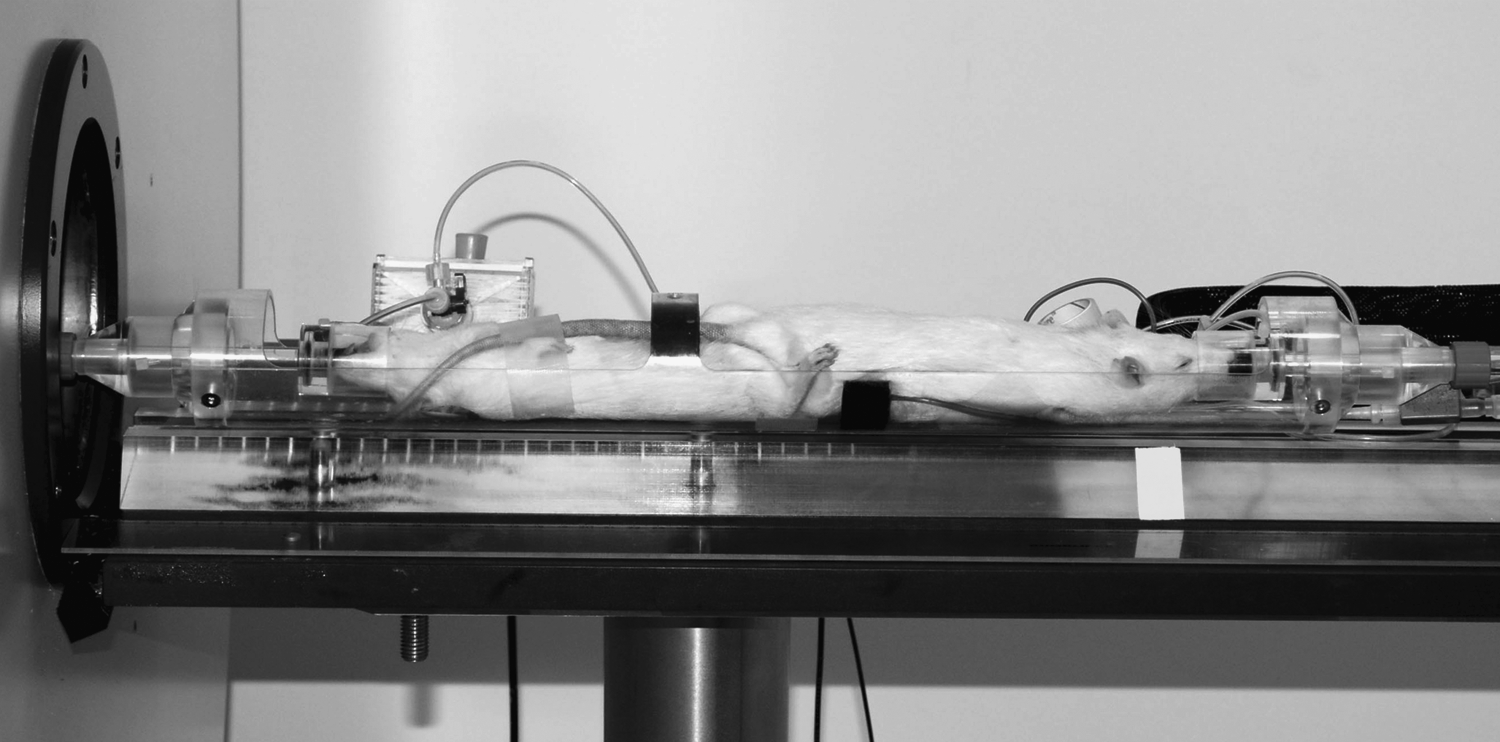
Position of the rats for MRI. Two animals were fixed in a purpose-built device to hold two animals with masks for gas anesthesia, temperature-controlled warming blankets, and Small Animal Monitoring System for monitoring respiration rate, ECG, and temperature.
T2-weighted scans are of basic type. Like the T1-weighted scan, fat is differentiated from water—but in this case fat shows darker, and water lighter. These scans are therefore particularly well-suited to imaging edema.
The pictures were converted to DICOM. The DICOMs were analyzed by comparing T2 weighted and Diffusion- weighted pictures to identify the region of free fluid under the skin.
Beginning points for the quantification were set on the slice that contained the joint line of the knee as an anatomical landmark. Subcutaneous fluid accumulation in three dimensions around the knee was calculated by using ITK-Snap 2.0 for Windows XP. Levels of the right (operated and irradiated) and left (healthy) hind leg were compared (Fig. 3). Statistical analysis utilized the standard t-test.

T2-weighted MR-images of a rat lying in abdominal position
Results
Macroscopic inspection of the legs did not show differences between postsurgical legs and control limbs.
MR images were analysed in eight of 12 animals after excision of lymphatic vessels and lymph nodes of the right hind leg, and the volume of subcutaneous fluid was calculated. Four animals could not be analyzed. In two of them, chemical shift artifacts interfered with the region of interest and in two animals the region of the knee was not completely shown due to poor animal positioning. Volumes of eight evaluated animals are shown in Fig. 4. Seven of them show a higher volume of fluid under the skin of the right (treated) leg. The elevation of fluid volume in the postsurgical limbs was statistically significant (p=0.028).

Graph of volumes calculated by ITK-Snap in mm3; seven animals document a higher level of volume in the operated and irradiated leg.
Discussion
Animal models to study surgical techniques for prevention and therapy of secondary lymphedema are rare and quantification of edema volumes in rodents is difficult and rarely documented adequately. This leads to highly variable and nonreproducible data.
In the present study we successfully measured subcutaneous swelling of rat hind legs after removal of the lymphatic vessels and lymph nodes of the leg and radiotherapy by MR imaging. Inspection of the legs did not show differences between healthy and treated legs. On MR images a higher subcutaneous fluid accumulation in T2- weighted images was documented in the treated rats.
ITK- snap© was used to quantify fluid accumulation in this study. In analogy to the work in neurological interrogations, the area of edema was determined and the program calculated the region with the same intensity next to the determined point.
In seven of eight calculated animals, the volume of subcutaneous edema was higher in the treated leg as measured by segmentation of MR images. A statistically significant increase of volume was demonstrated. Lymph node excision and radiotherapy are suitable to induce lymphedema in rats.
Avraham et al. irradiated mouse tails with a single doses of 15 or 30 Gy. 21 Four weeks after radiotherapy they documented an increase of tail volume in both groups. At 12 weeks after radiation, the volume showed no difference to control animals. In the present study, rats were sacrificed four weeks after radiotherapy for volume calculation. Whether it will be possible to use our model to induce a stable lymphedema for longer than four weeks, with the chronic findings of tissue swelling and fibrosis will require investigation in future experiments.
Histological and functional examination of the skin of the extremities can help to define the diagnosis of lymphedema in future trials. Lymphedema results from reduced transport of lymphatic load. This can be shown by scintigraphy of lymph vessels or injection of fluorescent agents or in MR contrast studies after injection of gadolinium. 16
Radiotherapy results in a loss of dermal lymphatic vessels and promotes the development of scar tissue in the mouse tail. 21 The effects of radiation on the rat's skin and dermal lymphatic vessels in the groin could complementarily be examined in future trials.
We show a statistically significant increase of total volume in the treated leg. Nevertheless, the model can be improved, as the detected volume was subclinical. Additionally, two of the animals were omitted from the analysis because of their position in the scanner. The rat's limbs have to be fixed in an exactly reproducible manner in future trials so that all animals can be analyzed. In the present study only edema at the level of the knee was considered. Swelling in the paw was not taken into account. Tammela and colleagues 15 calculated swelling in the paw in a murine forelimb model. Total leg volumes have not been calculated on MR images in the literature. However, different starting points for calculation with ITK- Snap could make this quantification possible.
In our experiments, we used young Lewis rats with a weight of approximately 200 g. In patients secondary lymphedema often occurs in older age groups, 22 and older animals might develop more obvious limb swelling.
Avraham and colleagues recently demonstrated, four weeks after radiotherapy, an increase of tail volume of 15% in animals radiated with a single dose of 15 Gy. Animals irradiated with 30 Gy demonstrated an increase of 25%. Other studies on edema models in rodents demonstrate the development of reliable edema in the extremity after radiotherapy with a single dose of 45 Gy. 22 Thus a higher radiotherapeutic dose might improve the outcome of experiments in future trials.
In conclusion, diffusion- and T2- weighted MRI is suitable for quantitative imaging of subclinical fluid accumulation in rats. ITK- Snap is useful to calculate the volume of subcutaneous swelling. Lymph node dissection followed by radiotherapy with a single dose of 15 Gy leads to a statistically significant increase of subcutaneous swelling.
Footnotes
Acknowledgments
The authors thank Katrin Häussler, Institute of Biometry for Statistical Analysis, Sheila Fryk for polishing the English, Sabine Buhmann for secretarial help, Marita Peter for her help with the figures, and Cornelia Hoepfel for excellent technical assistance.
Author disclosure statement
No competing financial interests exist.