
Abstract
Abstract
The use of compression garments in treating lymphedema following treatment of genital (penis, testes, uterus, cervical) and breast cancer treatment is a well-established practice. Although compression garments are classified in compression classes, little is known about the actual subgarment pressure exerted along the extremity. The aims of this study were to establish an in vitro method for measuring subgarment pressure along the extremity and to analyze initial and over time subgarment pressure of compression garments from three manufacturers. The measurements were performed with I-scan® (Tekscan Inc.) pressure measuring equipment once a week during a period of 4 weeks. Wear and tear was simulated by washing and putting on the garments on plastic legs every day. There was a statistically significant difference between the garments of some of manufacturers. There was no difference between garments from the same manufacturer. No significant decrease of subgarment pressure was observed during the trial period. The study demonstrated that Tekscan pressure-measuring equipment could measure subgarment pressure in vitro. The results may indicate that there was a difference in subgarment pressure exerted by garments from different manufacturers and that there was no clear decrease in subgarment pressure during the first four weeks of usage.
Introduction
A variety of pressure transducers have been used in studies to measure surface pressures at the interface between compression garments and the skin; for example, the Kikuhime device 3 (TT Medi Trade, Sorø, Denmark) and the I-scan® system4–7 (Tekscan Inc., Boston, MA). The Kikuhime device consists of a 3-mm thick air-filled rubber bladder pressure transducer, which can measure pressure at one point, whereas the I-scan® system uses one or multiple sensors and is ultra thin (0.15 mm). In most of the studies, subgarment or sub-bandage pressure has been measured merely at one or a few levels along the extremity.
In 1997, Mann et al. measured in vivo mean subgarment pressure under burn garments using the I-scan® system with sensor 9801 and found a high validity and reliability (r=1).4,5 Liu et al. (2005) 6 measured in vivo subgarment pressure, on garments used for venous disorders, using Tekscan FlexiForce interface pressure sensors along the leg at 4 different levels. Macintyre (2007) 7 measured in vivo subgarment pressure under burn garments along the extremity in order to optimize compression using the I-scan® system with sensor 9801.
No studies have been performed to measure the actual subgarment pressure of garments used for lymphedema treatment, along the entire extremity. To achieve a more well-adapted treatment for each patient, it would be of interest to be able to easily assess the longevity of the garment (i.e., the decrease of subgarment pressure by time in order to determine when garments should be renewed). Furthermore, the possibility to optimize the subgarment pressure might reduce the patient's discomfort and consequently augment the compliance. Compliance is essential to maintain the compression therapy and hence a stable arm volume postoperatively. 3
The aims of the present study were to establish a method of measuring subgarment pressure using the I-scan® (Tekscan Inc.) pressure measuring equipment and to analyze initial and post-wear and tear subgarment pressure along the extremity of 5 similar compression garments from three different manufacturers.
Material and Methods
Plastic legs and garments
Fifteen identical plastic lower legs were obtained from a company manufacturing mannequins for clothing shops (KA Olsson & Gems AB, Mölndal, Sweden). The legs are made of recyclable high-density polyethylene and have a hard surface. Measurements were taken according to standard procedures on one of the legs and used when the garments were ordered from the manufactures. Five custom-fitted and flat-knitted below the knee compression garments, compression class 3, compression range: 34.0–46.0 mmHg, were ordered from each of the 3 different manufacturers. The manufacturers were not informed that the garments were intended for a study.
Pressure measuring device and calibration
All pressure measurements were made with I-scan® system (Tekscan Inc.) with an ultra-thin flexible sensor (0.15 mm), sensor model 9801 (see Appendix) The sensor consists of a total of 96 sensing points, organized in 6 columns and 16 rows. To avoid artifacts and peak values due to the normal curvature of the leg, the sensor was split in half and trimmed down to a total of 2 columns of 16 sensors each (Fig. 1). The distal group of 8 sensing points was used to fix the distal part of the sensor, thus leaving 24 points to use for the analyses. The sensor was composed of two layers of very thin polyester sheets, each coated with opposing electric conductors enclosing a pressure-sensitive material patented by Tekscan Inc. The property of the interlayer material allows it to alter its electrical conductivity in a linear way when different amounts of force are applied. The flexibility and thinness of the sensor allows it to be placed easily between the plastic leg and the compression garment.
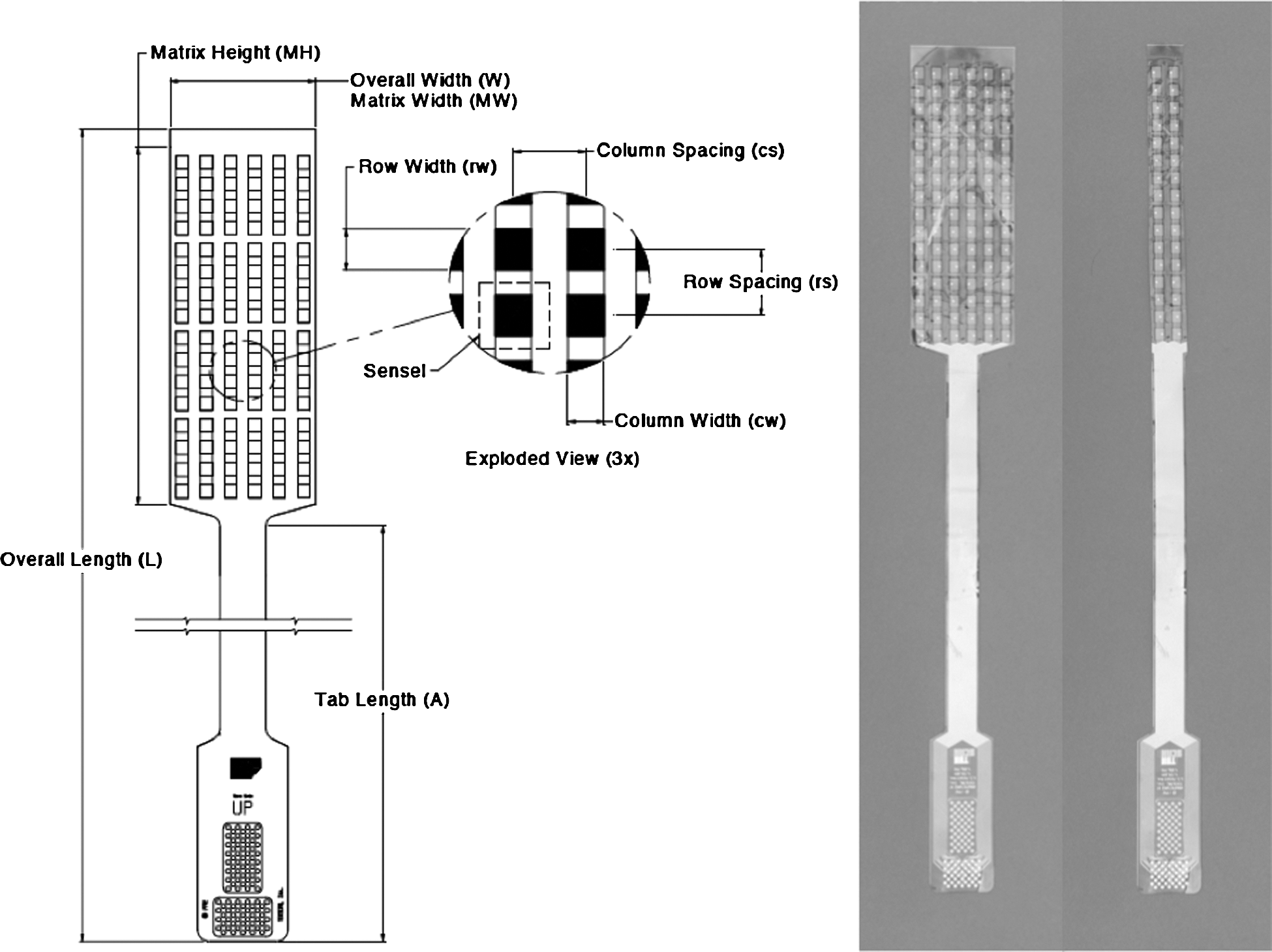
The drawing shows the sensor in detail. The photo depicts original sensor (left) and the trimmed modified sensor (right).
Measurements were directly recorded on a PC via a transducer (Tekscan, Model EH-2). The Tekscan software presents the measurements both in a numerical and a graphical way. All the readings were exported to Microsoft© Excel.
The electrical properties of the sensor incorporate a slight drift, that is, if the sensor is loaded with the same amount of force repeatedly, it will deliver a slightly higher reading over time. The drift is most apparent the first 30 seconds of loaded time. To achieve accurate readings, it is therefore important to calibrate the system. The sensor and the software were calibrated with a linear calibration tool (Tekscan, Model PB5A). The calibration tool is composed of two metal plates, in between which the sensor is inserted. The air piston of the tool is then loaded with an appropriate amount of weight, in this case a 500 g weight providing a uniform pressure of 6 kPa (=45 mmHg), which fills a polyurethane bladder that in turn compresses the sensor (Fig. 2). The bladder membrane delivers a uniform output to all of the sensing elements. First an equilibration is made after pressure application to allow the sensor output to stabilize. The device normalizes the output of all the sensing elements with the help of the Tekscan software. Once equilibration is finished, the sensor is calibrated using the same pressure. The amount of pressure applied is recorded by the pressure gauge and transferred to the Tekscan software in the computer. The equilibration and calibration and the actual reading are performed after the same amount of time (2 min).

Equilibration and calibration is made with the linear calibration tool (Tekscan, Model PB5A).
Measurements
To achieve a texture that resembles the softness of human tissue, measurements were performed on three different configurations (Fig. 3): (1) bare legs, (2) legs lined with standard Velcro made of 100% Polyamide (Velcro brand fastening systems, Velcro USA Inc., Manchester, NH), and (3) legs lined with foam material (Poron® urethane foam, Rogers Corp., Rogers, CT). The sensor was fixed to the leg using thin adhesive tape (3M Micropore, St. Paul, MN). An electronic tonometer (Tonometer Model 1329, Biomedical Engineering, Flinders Medical Centre, Bedford Park, South Australia) was used to evaluate the three different alternatives. 8 The principal mechanism of a tissue tonometer is to evaluate the resistance of the tissue when compression is applied. The tonometer device is composed of two plungers, one outer (diameter 55 mm) that is compressed fully (about 3 mm) when applied on the area to be measured and one inner plunger (diameter 11 mm), located in the center of the outer, that moves freely. The Lymphometer is gently pressed on the tissue. When the outer plunger is fully compressed, a beep is heard after 2 seconds, during which time inner plunger is forced into the tissue. When the Lymphometer beeps, the measurement of the inner plunger is locked and read. The tonometer is always calibrated before use. To avoid any disturbance of the set up, an Easy slide (Arion, AG Geleen, Nederlands) was used when the garment was put on. Measurements were recorded from the malleolus and proximally 30 cm along the lower plastic leg (Fig. 3). Thus, a total of 24 measuring points were used, with a distance of 1.27 cm between each point. All graphs show the distance (cm) along the lower leg on the x-axis, were distance 0 cm equals the malleolus. The y-axis represents the force (mmHg) applied by the compression garment in each given point along the lower leg.
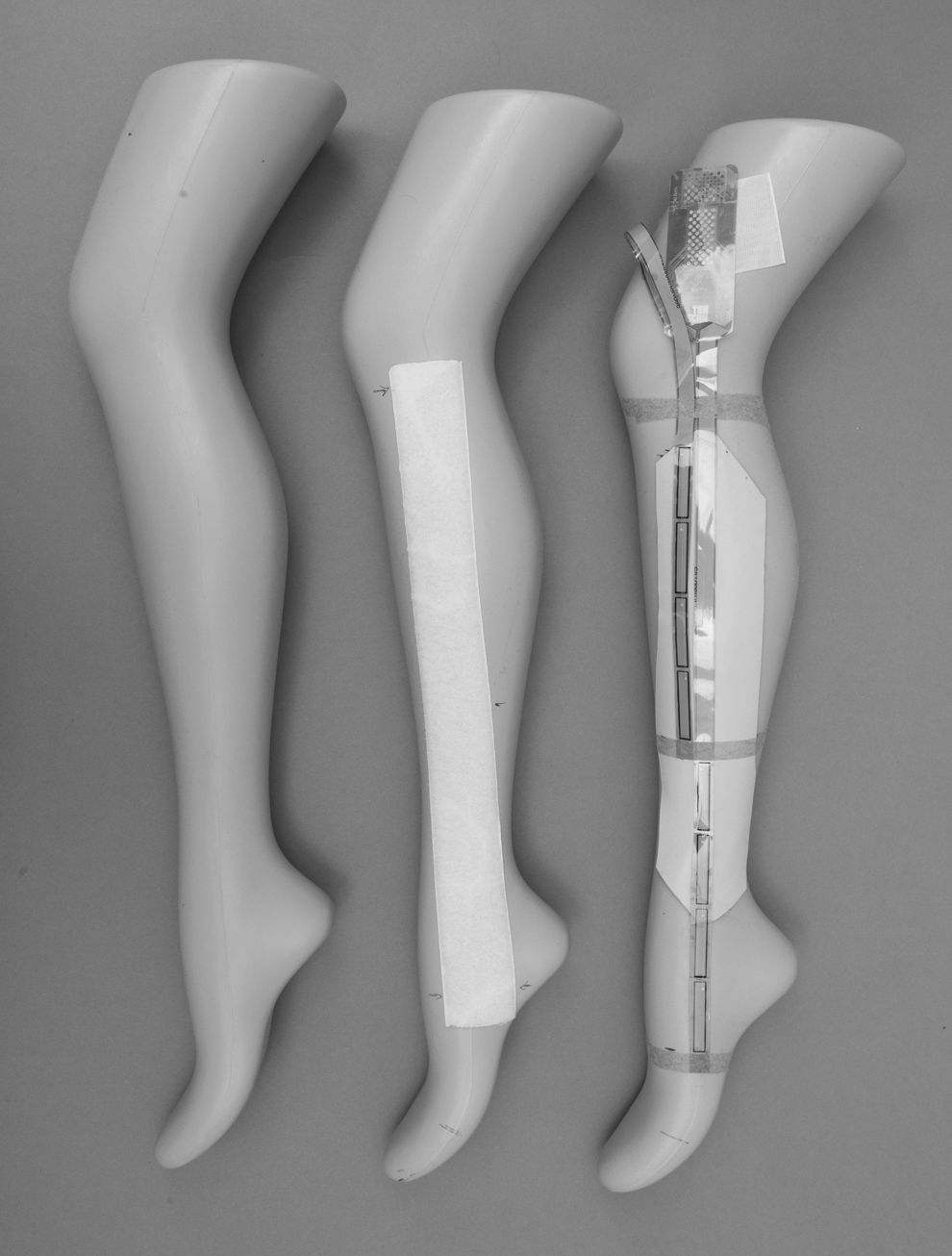
The photos depict, in order from left to right, the bare plastic leg, the leg covered with Velcro, the leg covered with foam and the sensor placement on top of the foam.
Initial measurements and simulation of wear and tear
The initial measurements were made on the garments fresh from the manufacturers. They had not been subjected to washing or exposed to any handling that might alter the garments' elastic properties. To be able to assess the decline in subgarment pressure over time, wear and tear of the garments was simulated by washing in the evening, drying overnight, and then put on to the plastic legs during the next day. This procedure was repeated for 7 days between each measurement, which was made in the evening of the seventh day. The procedure was repeated for 4 weeks. The garments were washed in a washing machine according to a standard careful washing program at 40°C. A mild synthetic detergent was used, in accordance with the manufacturers' recommendations.
Statistical methods
The measured factors were not statistically normally distributed and hence values are presented as medians and range or 1q–3q, and nonparametric methods were consistently used. The initial pressure in each of the 24 pressure points was calculated from the mean exerted pressure of 5 garments from each manufacturer. The mean of all 24 pressure points along the garment was used to calculate the pressure gradient of each garment. Differences over time within the groups were analyzed using the Wilcoxon signed rank test, and differences between groups were analyzed with the Mann-Whitney test. The outcome of the significance tests was considered as exploratory results; therefore nominal p values are presented without any adjustment for multiple comparisons. A p value of 0.05 or less was considered to indicate a statistically significant difference.
Ethics
The procedures followed were in accordance with the Helsinki Declaration of 1964, as revised, and the Good Clinical Practice (GCP) guidelines.
Results
The evaluation of the three materials to measure on (Fig. 3) revealed that the foam material had a tonometry value of 30 N/mm2, which is close to that of a normal human leg. 8 Furthermore, foam did not produce any extreme values that could be seen when measurements were performed on the bare leg, a hard and inelastic surface. Thus, foam was used for all the measurements in this study.
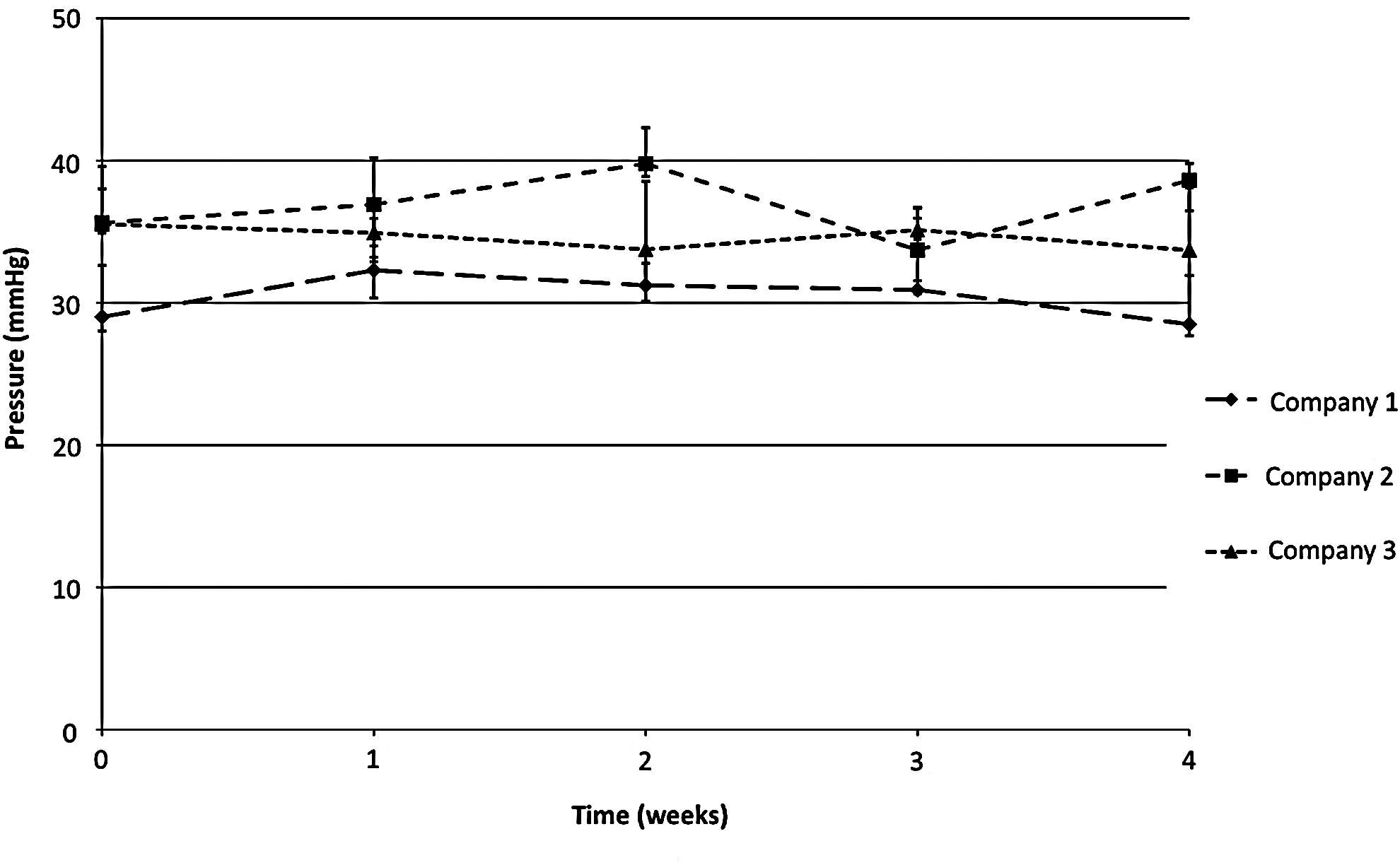
Table 1 and Figure 4 show the initial median pressure outcome of all measurements along the leg of each set of compression garment. There was a statistically significant difference in exerted subgarment pressure between the garment of Company 1 and 2 (p=0.009**) and between Company 1 and 3 (p=0.028*), but not between Company 2 and 3 (p=0.531) (Table 3). There was no significant decrease in subgarment pressure from any manufacturer during the observation period (Table 2, Fig. 5). There were statistically significant differences between the manufacturers during the wear and tear period (Table 3).
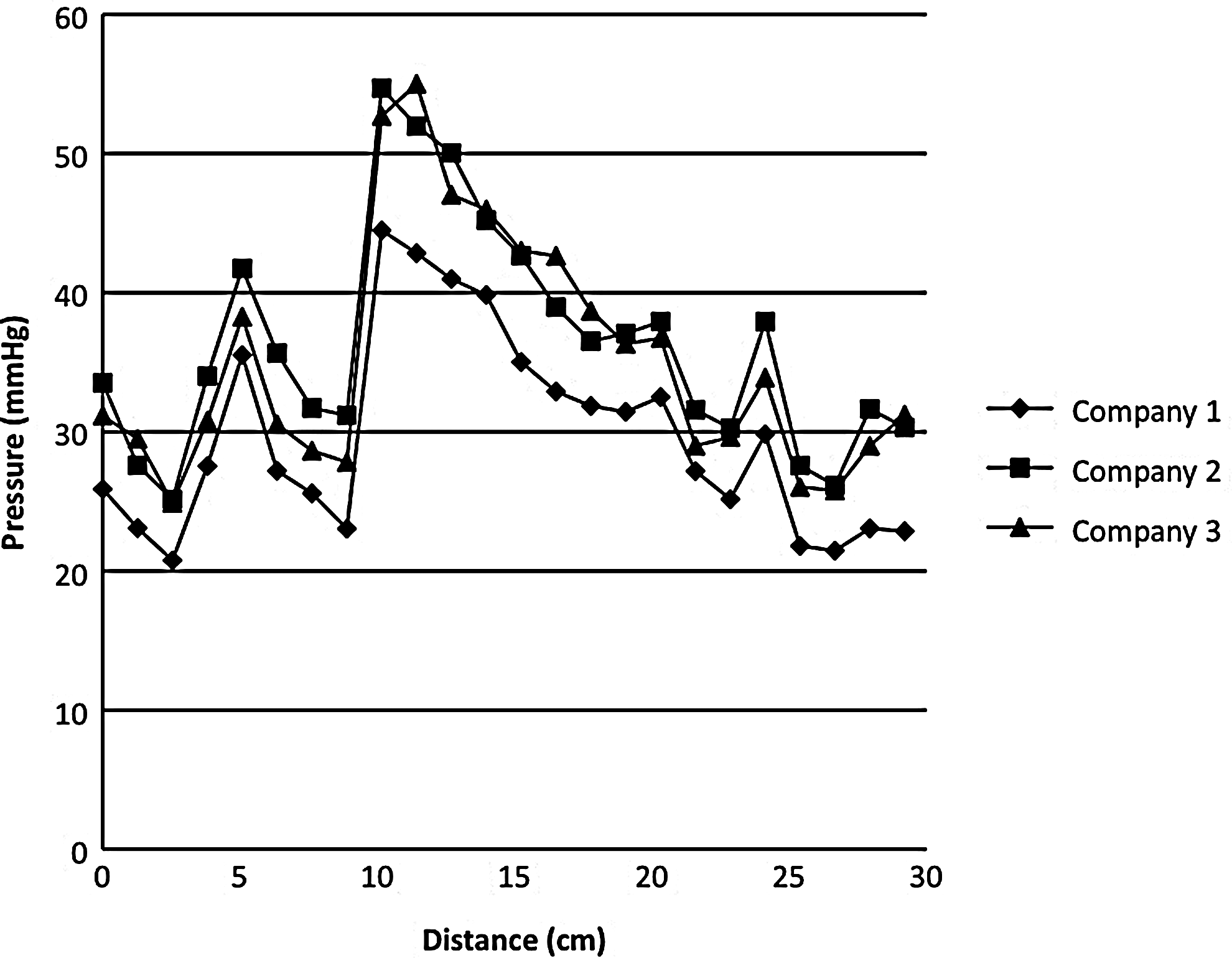
Initial mean pressure gradient along the leg of all 5 garments from the 3 manufacturers. For statistical outcome, see Table 3.
Initial pressure outcome (mmHg) of all measurements from 24 measuring points along the leg of each set of the 5 compression garments.
No significant differences were found within groups during 4 weeks' of wear and tear.
Comparison between groups before (fresh) and during 4 weeks' of wear and tear.
=p<0.05
Conclusion
One of the cornerstones in modern conservative treatment of lymphedema is the use of compression garments. The treatment is essential to preserve extremity function and to avoid morbidity and discomfort for the patient. To achieve results with compression therapy, it is important that the subgarment pressure exerted by the compression garment is high enough to enable a decrease in lymph fluid deposition and to maintain this state over time. On the other hand, it must not be so high that it causes discomfort that lowers the patient compliance. Previous research has showed that the subgarment pressure used often is higher than needed for sufficient treatment. 3 A method for measuring subgarment pressure in vivo, and for determining at which pressure the treatment effect is optimal, is essential to ameliorate the treatment of lymphedema.
According to international standard, compression garments are produced in different compression classes. The different classes are defined by a measure system that gives an estimate of the garment's stiffness in a two-dimensioned way rather than the actual subgarment pressure. However, previous studies indicate that the two-dimensional stiffness of the garment corresponds well to the actual subgarment pressure. 9 Thus, the manufacturers measure flat-knitted garments using a method where the garment fabric is stretched along its length. Based on the measurements of the amount of force used, and the increase in length that occurs, an estimated classification of the garments pressure profile can theoretically be calculated.
Even though the use of compression garments in the treatment of lymphedema is a well-established method, little is known about the longevity of garments and the optimal pressure required for adequate treatment. 10 This study set out to establish a method for measuring the actual subgarment pressure provided, during wear and tear, by using the Tekscan pressure-measuring equipment. The I-scan® (Tekscan Inc.) system has previously been used to measure local point pressure under arm burn garments, 5 and along the extremity on specified levels,6,7 but not to measure the pressure profile along the extremity. The lack of significant difference within each manufacturer's garments as compared to initial values, during the 4 weeks of wear and tear, may indicate high quality and maintenance of pressure in the compression garments during the first weeks of usage. However, to truly evaluate the effect of wear and tear, and decrease in subgarment pressure, a longer study period of at least 3–6 months, corresponding to garments' normal life span according to the manufacturers, would be needed
Furthermore, our study method only simulates the washing and taking on and off of the garment, but not the actual wearing on the extremity that changes its shape constantly during movement. Movement would further add to the wear and tear. Moreover, the dynamic behavior of pressure garments is considerably different than static behavior and the pressure exerted changes according to activities of daily living. 11 In a clinical application, it would be interested to know how much the pressure of the garments changes in the ambulant patient to be able to optimize the treatment of lymphedema further.
In addition, to achieve a good result in the lymphedema treatment with compression garments, it is important that the garments' pressure profile is correct, that is the subgarment pressure should be highest at the distal part of the extremity, and decrease along the extremity. This is not always achieved with standard garments. 12 In this study, it was demonstrated that all garments did not show a continuous drop in pressure from distal to proximal leg. We have no clear explanation of the sudden increase at the 10 cm level (Fig. 4). The same outcome was found when Velcro and no padding were used, and when different parts of the sensor were tested. There is a trend in the pressure data, which indicate that the readings are accurate. It could be due to increase in leg diameter at this point, but this should be compensated for by the manufacturer according to measurements of the patient's leg.
In this study, no suitable ready-made sensor was found and hence a modified sensor (Model 9801) had to be used to be able to measure along a distance of 30 cm of the lower leg. Our modified sensor is not feasible to use for in vivo measurements. A longer sensor, in one piece, would be more apt for clinical use. Since a normal leg is around 84 cm long, a sensor of that length would be ideal. For arms, a length of 44 cm is sufficient. A clinically usable in vivo measuring device would be important for future research regarding compression therapy and would give a better understanding of how subgarment pressure alters with time in a clinical setting. Such research would make an individualization of compression therapy possible and give valuable information about the number of garments needed for the lymphedema not to recur. 13 This would probably, in the long run, lead to decreased costs for the health care system as it would be possible to avoid maintenance therapy, such as massage and bandaging.
In conclusion, there was an initial difference between some of the manufacturers' garments. However, the homogeneity within garments from the same manufacturer was satisfying. No significant decrease of subgarment pressure was observed during the trial period. The study demonstrated that Tekscan pressure-measuring equipment could be used to measure subgarment pressure in vitro. Nonetheless, it would be of interest to develop a modified simpler sensor for a more straight forward subgarment pressure measurements to be able to perform in vivo measurements in a time efficient way and to promote further research in the field.
Footnotes
Acknowledgments
We thank occupational therapist Karin Ohlin, physiotherapist Barbro Svensson, and Magnus Dustler MSc for skillful counseling.
The project was supported by the Tegger Foundation, the Swedish Society of Medicine, the Lundgren Foundation, the Swedish Cancer Society, the Foundation Against Cancer at Malmö University Hospital, the Thureus Foundation at Uppsala University, the Royal Physiographic Society in Lund, and Skane County Council's Research and Development Foundation.
Author Disclosure Statement
The authors state that no competing financial interests exist.