
Abstract
Abstract
Background:
Progressive osteolysis caused by lympathic malformations is a rare condition that should be known by specialists involved in the study of lymphatic disorders because they are necessarily involved in the treatment. The purpose of the present study is to report on a large series of patients to illustrate the multiple clinical pictures and the wide range of therapeutic measures necessary for arresting bone destruction and lymphatic leak.
Methods and Results:
Inclusion criteria were osteolysis associated with lymphatic malformation that required treatment. Diagnosis was based on history, plain X-rays, MRI, and demonstration of the lymphatic nature of the lesions with D2-40 immunohistochemistry. Treatment was based on resection of the bone lytic lesion or soft tissue lymphatic masses, control of chylothorax or chyloperitoneum, interferon, zoledronic acid, and radiotherapy. The study included 54 patients (25 females and 29 males) with a median age of 9 years (range 2 to 65). Eight patients had focal osteolysis without soft tissue lymphatic anomaly, 15 multifocal osteolysis without soft tissue lymphatic anomaly, 7 focal osteolysis associated with soft tissue lymphatic anomaly, and 24 multifocal osteolysis with soft tissue lymphatic anomaly. Among the wide variety of pharmacological therapies provided, only one protocol showed a consistent positive effect (end of ostelytic progression) in 17 patients who received a course of 6 to 15 months of interferon alpha-2B at 1.5 million units/m2 body surface area/day in association with zoledronic acid at 0.05 mg/kg/month. Thirty-two patients underwent multiple surgical procedures in order to remove the soft tissue involved, correct orthopedic problems, or improve chylothorax, and three were treated with radiotherapy which was successful in one case.
Conclusions:
Osteolysis from lymphatic origin is a devastating surgical condition. Therapeutic options have to be considered separately if the disease is active or inactive and according to the targeted organ (skin, bone, or viscera). Total removal of the lymphatic anomaly is rarely possible, but its subtotal excision together with pharmacological antiangiogenic therapy in selected patients under surveillance of a multidisciplinary group familiarized with the disease, minimize the progression of both, lymphatic invasion, osteolysis, and their serious complications.
Introduction
Progressive idiopathic osteolysis was first reported by Jackson in 1838 in a 12-year-old boy with complete osteolysis of the humerus. 1 In 1955, Gorham and Stout further characterized the main pathologic features of this rare disease as nonmalignant intraosseous proliferation of vascular tissue that caused massive osteolysis. 2 The disease has been described in patients as young as 1 month to as old as 75 years. Imaging features at conventional radiography, CT, MR, and scintigraphy have been reported elsewhere in the literature, and most of the cases failed to show the vasculature entity of the lesion, an important pathologic feature of the disease. Moreover, because of a lack of specific findings on conventional images, including those of conventional radiography and CT, the diagnosis of Gorham disease or generalized bone lymphatic anomaly can be difficult. It often takes many years for the condition to be recognized. Because of this rarity, it is most unusual for a case of the disease to be known from the beginning of an incident and for ancillary treatment to be commenced at once.
Modern classification of vascular anomalies of the bone into tumors and vascular malformations follows the ISSVA nomenclature of vascular anomalies used for those of the skin, soft tissue, or viscera. 3 Immunohistochemical identification of the nature of the endothelium involved in bone destruction allows separation of this entity from “angiomatosis of the bone” in which blood vessels, and not lymphatic structures, are involved.4,5 Appropriate classification facilitates the choice of likely effective therapeutic protocols.6,7
In addition, the prolonged chyle depletion observed in patients with associated soft tissue lymphatic anomaly, chylothorax, or chyloperitoneum may result in nutritional, metabolic, and immunologic deficiencies due to loss of essential proteins, immunoglobulins, fat, vitamins, electrolytes, and water, needing specific nutritional support with low-fat diet and medium-chain triglyceride restriction.
Surgeons are necessarily involved in the diagnosis and treatment of these patients but, unfortunately, not many of them are familiar with the proteiform clinical features of this condition and the multiple therapeutic measures that are required for its relief. These unfortunate individuals often travel to various cities and countries and become, as John B. Mulliken described several years ago, “nomad patients,” in a search for relief in the clinics of hematologists, oncologists, rheumatologists, orthopedic, plastic, pediatric, or thoracic surgeons, depending on the location of the lytic lesions. 37
The purpose of the present report is to summarize the findings and the results of multidisciplinary management of a large number of patients with lymphatic osteolysis referred to our institution.
Materials and Methods
We reviewed the charts of patients treated for lymphatic osteolysis at our department in the last 15 years (Table 1). Inclusion criteria were:
• Osteolysis associated with soft tissue lymphatic malformation or lymphangiomatosis (Fig. 1).
• Aggressive idiopathic osteolysis without soft tissue lymphatic malformation (Fig. 2).
• Multiple osteolytic lesions without soft tissue lymphatic malformation with a positive immunohistochemical staining against D2-40 markers on biopsies (Fig. 3).
• Osteolytic lesions without soft tissue lymphatic malformation associated with chylothorax or spleen involvement (Fig. 4).

Spine osteolysis associated with axillary, pelvic, and splenic lymphatic malformation.

Aggressive cubital osteolysis without soft tissue lymphatic malformation.

Aggressive multifocal osteolytic lesions without soft tissue lymphatic malformation.
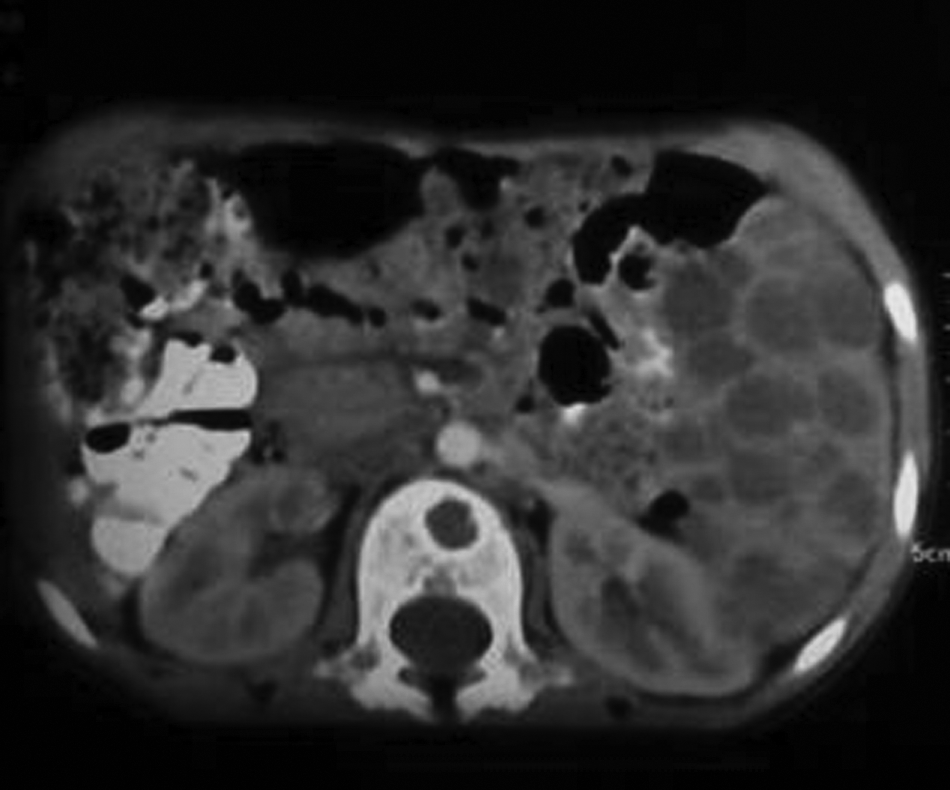
Osteolytic lesions without soft tissue lymphatic malformation associated with chylothorax and spleen involvement on MRI.
Diagnosis was made on the basis of clinical symptoms, imaging (MRI, CT, and X-rays), or open biopsy of the bone lesions. Regular HE stains were complemented with immunohistochemistry for D2-40. In these cases, paraffin-embedded tissue blocks were selected, and sections from the blocks were cut and placed on glass slides coated with 3-aminopropyltriethoxysilane. They were then incubated with an antihuman D2-40 monoclonal antibody (Signet Laboratory, Dedham, MA) at 1:200 dilution for 60 min at room temperature, then with biotinylated antimouse immunoglobulin for 15 min, and then with avidin–biotin complex reagent (LSAB kit, Dako, Carpinteria, CA) for another 15 min. Next they were reacted with a 3, 3'-diaminobenzidine tetrahydrochloride (Mutoukagaku, Tokyo, Japan) solution and 0.01% (weight/volume) hydrogen peroxide for 2–5 min at room temperature and counterstained with hematoxylin, directed to identify the lymphatic nature of the lesions.
Patients were first classified as suffering from active or inactive disease. The disease was considered active if new osteolytic lesions were noticed in the preceding 3 months. If not, it was considered as inactive. Patients with active disease were proposed for pharmacological treatment, while those with inactive disease were not.
Treatment was based on surgical excision of the lymphatic mass when present, followed by interferon alpha 2B (1.5 million units/m2 body surface area/day) and zoledronic acid at 0.05 mg/kg/month for a period between 6 and 15 months. Additionally, 7 patients underwent intramedullary nailing, 6 had spine stabilization, and 2 had plate osteosynthesis to correct spontaneous fractures. Symptomatic lymphatic effusions without response to pharmacological therapy or surgery were treated by pelvic and thoracic radiotherapy sessions in 3 patients 10 Gy of 10 MV photons in 14 fractions over a 15-day period.
The criteria for considering the treatment successful or failed were arrest of osteolysis progression and pain, with significant improvement in physical activity. Follow up was based on clinical visits every 3 or 6 months and repeated imaging.
Results
Fifty-four patients (25 females and 29 males) with a median age of 9 years (range 2 to 65) (44 from age 2 to 10, 6 from age 10 to 40, 4 more than 40) presenting with bone destruction suspected to be due to lymphatic involvement were referred to our institution from 9 different countries, in many instances through the Gorham's Patients Association (www.gorhams.org).
The most common initial symptom was pain. In 11 patients, osteolytic lesions were noticed on X-ray without previous symptoms.
Nine patients had aggressive complete or near complete bone destruction (iliac bones in 5, cubitus in 2, and more than 8 ribs in two patients). Two patients suffered from complicated meningitis after partial mastoid and ethmoid bone involvement. Three patients had bilateral and symmetric foot involvement, requiring amputation in two cases. Only 8 patients suffered from spontaneous fractures, which were not correlated with the aggressiveness of the disease. Severe trauma was not recorded in any of them. Twenty-three patients had thoracic involvement and 18 of them presented with chylothorax or chylopericardium.
The spleen was involved in 9 patients, 4 of whom had disseminated lymphangiomatosis, with focal lesions in 5 patients. Ten patients received interferon alpha 2B(IF 2B) at 3 million units/m2 body surface area/day; 6 patients received unsuccessful courses of pamidronate at different institutions, and 17 received a course of 6 to 15 months of IF 2B at 1.5 million units/m2 body surface area/day plus zoledronic acid at 0.05 mg/kg/month. Only those 17 were followed up by the first author (after considering as active the osteolytic process) and they showed no progression of the bone destruction in any case. One patient had a skin rash and one had transient neutropenia as side effects, without the need for interrupting the treatment.
Interestingly, 4 patients underwent aggressive bone resection during the active course of the osteolytic process, resulting in termination of disease progression and cure. Additionally, 6 patients with severe spine involvement underwent uneventful spine arthrodesis.
Thirty-two patients underwent multiple surgical procedures after ineffective sclerosis of the lymphatic malformation in order to remove the soft tissue involved, correct orthopedic problems, and ligate the thoracic duct.
Three patients died at our institution in the context of respiratory failure and septic complications (Table 2).
Discussion
Classification and nomenclature
While waiting for international consensus regarding the criteria for definition of Gorham disease and generalized lymphangiomatosis with bone involvement, we decided to retain as inclusion criteria the demonstrated lymphatic origin of the osteolytic process, regardless of any other consideration as severity of the process or cortical destruction.
Our experience demonstrates that patients can suffer from different patterns of bone destruction unrelated to age, previous disease, or other features. Unifocal, multifocal, or diffuse lesions affecting 1 to 30 bones with different levels of aggressiveness were observed. Patients had aggressive bone reabsorption at different levels (30–60% or 90% of a single bone volume with different clinical outcomes).
Diagnosis
The etiology and pathogenesis of this disease remain undefined.7–11
Patients consistently had a different previous radiological diagnosis, with idiopathic osteolysis being the most common. Normally, histiocytosis and bone cysts in children or metastatic disease in adults have been suspected first. Biopsy of the lesions has commonly been the second diagnostic step. Biopsies are usually useful for ruling out previous clinical diagnoses and have a poor accuracy rate in clarifying their lymphatic origins unless performed by experts. 12,13
Osteomyelitis, angiomatosis of the bone, and idiopathic osteolysis are commonly found as diagnoses not only in our series of patients, but also in the medical literature. It is of paramount importance that a trained pathologist familiar with the disease establish the diagnosis. 3 We consider that every patient with osteolytic lesions and for whom biopsy is unable to confirm diagnosis is a serious candidate for bone lymphatic infiltrative disease. Many patients with consistent clinical and radiological findings undergo up to five unsuccessful biopsies to clarify a final diagnosis, and remain undiagnosed or misdiagnosed for years.
It is also to be noticed that no uniform imaging protocol was possible in view of the proteiform nature of the clinical pictures caused by the lymphatic bone destruction. Plain X-rays, CT scans, or MRI were used when necessary in the course of the osteolytic process. The best and most practical imaging exams are yet to be recommended but the goal is to determine whether the disease is active or inactive.
Clinical course
Our series show that the osteolytic process was self-limited and never progressed for longer than 15 months, regardless of the nature of of the treatment selected or even the abstention of it.
An important concern is the aggressiveness of disease progression. Osteolysis can progress over a period of weeks or months, can vary in speed, and is without relation to other factors. Fast osteolysis development is believed to be more dangerous, but we have no data to support this statement. Clearly, presence of chylothorax, as well as location and the extent of bone destruction, have much more importance as a prognostic factors.14–23
When managing patients with GD, a serious problem is the lack of a marker in blood or urine to determine stage or aggressiveness. VEGF and others such as metalloproteases have been postulated as useful by some authors, but none of them show specificity for lymphatic activity and they are have little clinical use. 24 Progression of osteolysis in several consecutive X-rays is the most accurate diagnostic tool to demonstrate lytic activity and is therefore an indication for pharmacological therapy to arrest the process.
Similarly, no markers for decreases in osteoclast activity are available and two consecutive radiologic exams without osteolytic progression should be considered as the end of the activity (not the disease, as orthopedic sequelae can be devastating).
It is curious that two patients with progressive osteolysis of the cubitus underwent surgical resection of the resorption-active end of the bone with a 2 cm margin, resulting in termination of the process and allowing reconstruction of the forearm with a vascularized fibula transfer. Unfortunately, this unifocal activity is not the most common presentation pattern, making a curative surgical approach rarely feasible.
Treatment
Arresting the lytic process must be the critical goal of the treatment and it should be acknowledged that bone regeneration is not to be expected regardless of the selected therapeutic option. From the clinical point of view, it is critical to identify at least six different problems in this group of patients: 1. bone destruction; 2. lymphatic malformation (macro- or microcystic) of the skin and subcutaneous tissue; 3. pleural and pericardial effusions; 4.visceral involvement;5. hematological disorders; and 6. pain, malnutrition, and psychological impairment.
All of these can appear together at different stages of the disease, and all need a separate and specific approach. No data are available to establish the relationship between aggressiveness and intensity of each process in different patients.
Bone osteolysis
We do not know if bone destruction happens in a random or nonrandom fashion. 25 Certain bones are more frequently affected, but the disease has been reported from skull to feet. Pharmacological treatment of osteolysis has been suggested, despite poor information regarding its origin and its relationship with lymphatic malformations.26–31
Clinical use of interferon alpha 2B in the treatment of vascular anomalies was introduced by Judah Folkman, 38 and is considered an option in patient with lymphatic disorders under two conditions: its use is safer and more effective at lower doses (1.5 million units/m2 bsa), and it has synergic antiangiogenic effects when used in combination with other antiangiogenic drugs such as zoledronic acid, a powerful bisphosphonate widely used in the treatment of osteoporosis.
Several reports as well as our experience confirm this therapy as useful in some patients. Bone regeneration does not occur, but the progression of the disease is ended. Nevertheless, it remains unclear whether this phenomenon is exclusively due to the treatment or is the result of factors such as the self-limited course of the disease.
Radiotherapy has also a role in the management of the disease.32–35 Stopping the progression of osteolysis and chylothorax has been reported, and one of our patients achieved a successful outcome of an untreatable lymphatic fistula after 15 sessions of radiotherapy.
Orthopedic management has to be tailored after considering the affected group of bones:
A. Vertebra: osteolysis of the spine is a serious concern as paraplegia or tetraplegia are frequent complications in untreated patients. Scoliosis and spondylolisthesis are also common findings after collapse of vertebral bodies. Orthopedic treatment is possible despite bone osteoporosis, and spine stabilization is a preventive procedure indicated if pain is untreatable or complications are expected.
Despite the lack of well-designed prospective studies to establish the efficacy of preventive instrumentation in these cases, the high incidence of reported paraplegia supports the use of instrumentation in unstable spines to prevent neurologic injury and maintain spinal alignment.
B. The skull is also commonly affected. Multifocal lytic lesions are the most frequent pattern, but some patients can develop single bone resorption with cerebrospinal fluid fistulae or meningitis as possible complications.
C. There is an intriguing relationship between rib involvement and chylothorax development. In fact, there is lack of information about the role of the lymphatic duct in the course of the disease.
D. Pelvis and lower limb involvement lead to significant morbidity and different types of disability can affect patients. Symmetrical patterns of osteolysis have been observed in 3 patients with foot and leg disease, but most appear in the trunk, head, and upper limb (Fig. 4).
According to our experience, the rate of bone fractures is low in patients with aggressive patterns without preventive intramedullary nailing. Therefore, the indication for this procedure has to be carefully considered. Significant morbidity associated with this procedure has been observed in 2 patients.
Lymphatic malformations and osteolytic lesions
The relationship between lymphatic malformations of the skin or subcutaneous tissue and osteolytic lesions has been well established. There is no consensus regarding criteria for lymphangiomatosis diagnosis. The size, extent, and type of location of a lymphatic malformation to be considered as disseminated lymphangiomatosis remain unclear. In any case, bone osteolysis is not uncommon in children with large or disseminated lymphatic malformation of the skin. It is significantly more frequent to find children with osteolytic lesions with cutaneous lymphatic malformation than children with a giant lymphatic malformation of the skin with osteolysis. Obviously the presence of both problems is a concern, but the prognosis is not necessarily poor. In those cases, staged removal, in as aggressive manner as possible, of the cutaneous macro or microcystic anomalies has resulted in significant clinical improvement. Cutaneous involvement in the vicinity of affected bones is common, so that the reduction of lymphatic aberrant tissue probably decreases the amount of lymph circulation and infiltration of the bone. Despite poor quality scarring and the difficulty of management during the postoperative period due to persistent lymphorrea, we recommend surgical excision of subcutaneous lymphatic malformation by expert surgeons whenever possible. A final point of interest is the presence of pigmented-like lesions of the skin in several patients with cutaneous lymphatic malformation and bone destruction. Histopathology shows no melanin in the affected skin despite this nevi-like coloration. In fact, the skin closely resembles plexiform neurofibromas. Amazingly, many children with neurofibromatosis type I develop congenital pseudoarthrosis and bone destruction with similar osteolytic patterns as those found in some children with Gorham disease (Fig. 5).
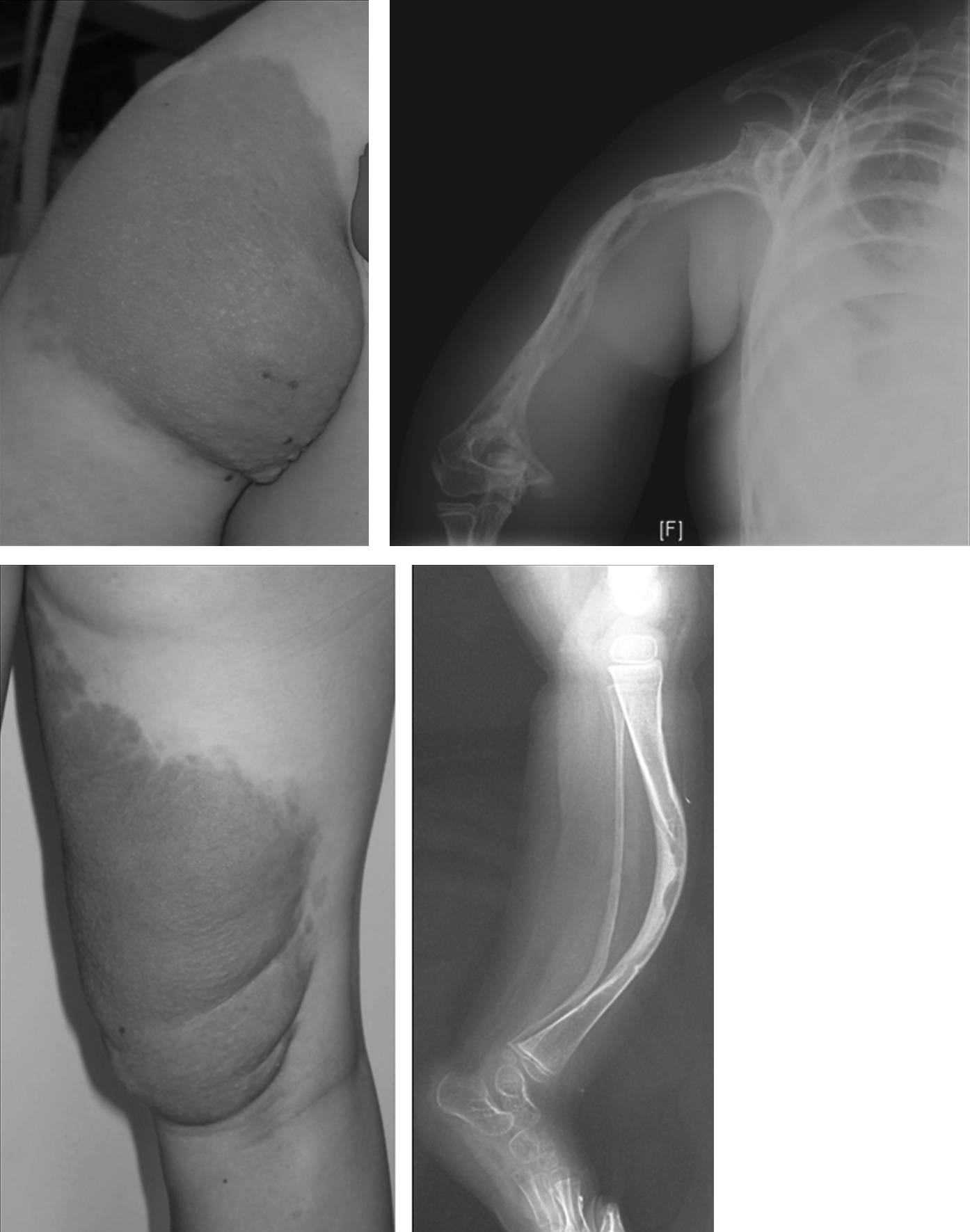
Similar cutaneous and X-ray findings in two patients with lymphangiomatosis and type I neurofibromatosis, respectively.
These findings, together with consistent signs of hypervascularization commonly found in those two different disorders, suggest a possible connection at the molecular level between Gorham disease and neurofibromatosis.
Thoracic involvement
Development of chylothorax in patients with chest osteolysis is a common finding. It is difficult to treat and may lead to severe complications if mismanaged. From the clinical point of view, mild symptomatology is common and most children do not need ventilatory support. Infection (empyema) is uncommon if properly managed. The issue, therefore, is when to treat and how to proceed. We support leaving asymptomatic patients untreated. Based on the self-limited progression of the disease, minimal to moderate pleural effusions will allow patients to have a normal quality of life and many patients in this group are overtreated with long-term parenteral nutrition, chest-tube replacements, pleurodesis, and thoracic duct ligation. In addition, there is no certainty of a successful outcome after aggressive management, so careful selection of candidates is mandatory. It is our protocol to treat only symptomatic patents using weekly percutaneous drainage. A chest tube placement is only indicated after failure of respiratory distress treatment using this therapy. Enteral nutrition with a low fat diet is then started, avoiding the use of TPN since morbidity is directly related to its use (central venous line infections, malnutrition, and immunodeficiency). After one month of unsuccessful conservative therapy and the need for ventilatory support, surgical options such as pleurodesis or thoracoscopic thoracic duct ligation must be considered. We have been asked to treat children with alarming pleural effusions on X-ray exams, without the need for ventilatory support, with up to 6 months of ICU stay, on total parenteral nutrition and in critical condition after several episodes of systemic fungal infection related to central venous catheters. Reintegration of enteral nutrition and progressive clamping of the chest tube has been the treatment of choice with progressive clinical improvement, despite persistent radiological chylothorax. Some of our patients remain asymptomatic after up to 6 years of chylothorax development. Factors such as lung parenchyma infiltration with bilateral pleural lymphatic malformation have a poorer prognosis, making thoracic duct ligation ineffective. A similar approach should be considered for patients with chylopericardium. Cardiac tamponade is infrequent and partial pericardiectomy is commonly successful if percutaneous drainage is insufficient (Fig. 6).
Chylopericardium in a patient with lymphangiomatosis and cardiac tamponade.
Among the 51 cases from the reviewed mortality in the literature between 1.954 and 2.010, 36 19 had bilateral chylothorax, 15 had right chylothorax, and only 2 had exclusive left chylothorax. Eleven patients had complications as respiratory distress and pneumonia, 10 suffered pathological fractures, and 10 underwent chylopericardium or chylous ascites. The most common cause of exitus was respiratory failure in 25 patients, followed by pneumonia and sepsis.
Visceral lymphatic malformations can be observed in patients with osteolysis
The spleen is the most frequently involved organ, and if severe thrombocytopenia is not present, splenectomy is usually unnecessary, as it does not change the natural course of the osteolytic disease.
Hematological disorders
A few patients develop hematological disorders, mostly anemia or coagulopathy in the context of extended vascular anomalies with a relevant lymphatic component and osteolysis.
Pain control
Finally, every patient with aggressive clinical course needs specific pain control therapy, nutritional support by a clinical nutritionist as well as psychological help, and a strict rehabilitation program. Patient associations such as the Gorham Disease Patients Association (ALEG) or the Lymphatic Alliance are key for the development of group strategies, research promotion, funding, accurate patient information collection, and data recruitment.
Conclusions
A correct understanding of the histological origin of the problem and appropriate pharmacological treatment according to the biopsy results are necessary. Strategies for understanding the disease must emphasize its apparent identity as a disease of disordered lymphangiogenesis, emphasizing the following points:
1. Osteolysis of lymphatic origin remains an underdiagnosed disorder. Any patient with osteolytic lesions must undergo a biopsy, including inmunohistochemical lymphatic studies, in order to confirm their etiology 2. The nomenclature is unclear and needs to be addressed to clarify a proper diagnosis. Most patients follow two patterns: focal, aggressive, with cortical destruction or multifocal without cortical destruction in the context of disseminated lymphangiomatosis, but a significant number of them shows a not well-defined pattern with mixed features from the two groups. 3. Despite its different form of presentation, osteolysis is uniformly a self- limited process and “phenomenon” would be more appropriate than “syndrome.” 4. Patients with confirmed diagnosis should be referred to a tertiary center familiarized with lymphatic disorders management. Osteolysis status (activity or sequellae) as well as the presence of chylothorax and or cutaneous/visceral lymphatic malformation have to be carefully addressed. 5. Therapeutic options have to be considered separately after considering if the disease is active or inactive and according to the targeted organ (skin, bone, or viscera) (Table 3). 6. A multidisciplinary team approach to the problem is necessary since progress in its understanding comes from different fields of medicine (genetics, biology, radiology, pathology, and surgery). 7. Global interchange of knowledge will improve research and future disease management.

Footnotes
Author Disclosure Statement
No competing financial interests exist.