
Abstract
Abstract
Background:
Assessment of lymphedema is frequently based upon measuring the increase in volume of the affected region compared to that of a comparable unaffected region. This requires methods that can measure the volume of body regions that are not only accurate and sensitive but also suitable for use in clinical practice. To date, bioimpedance spectroscopy has been used to measure volume increase due to lymphedema in whole arms but excluding the hand. We report here an impedance-based method for the measurement of hand volume.
Methods:
Impedance measurement electrodes were located on the dorsum of the hand, with the sense electrodes at the level of ulnar styloid and metacarpal–phalangeal joint of the third finger and current drive electrodes on the forearm and at the nail bed of the third finger. The impedances of the hands of 50 participants were measured and hand volumes computed. These were compared with the hand volumes measured by perometry. The region of the hand defined by the impedance measurements was determined, both in vivo and using a hand phantom.
Results:
The region of the hand measured by the impedance technique was limited to the palmar volume (i.e., excluding the thumb). Palmar volumes computed from impedance measurements were significantly correlated (r=0.88) with those measured by perometry but were, on average, 8% larger. The impedance technique was sufficiently sensitive to detect the change in hand volume elicited by decrease in vascular volume due to blood draining from the hand on elevation.
Conclusions:
An impedance technique was developed that has the potential to measure the change in hand volume when affected by lymphedema. Bioimpedance spectroscopy has the advantage over currently used perometric or water displacement techniques in that it can measure specifically the change in extracellular fluid, including lymph, rather than simply total hand volume.
Introduction
Unfortunately, techniques such as these may not be capable of detecting the very earliest or latent stage of lymphedema, before discernible change in overall volume has occurred. Bioimpedance spectroscopy (BIS) has been shown to have the required sensitivity to detect latent lymphedema since it measures only the accumulation of extracellular fluid (ECF), of which lymph is a principal component, rather than overall volume. 7 Strictly, BIS measures the impedance of the volume of the water space only. However, since this represents greater than 95% of the total fluid space, the more commonly used terms of fluid spaces are used throughout the article. To date, BIS has only been used to detect and assess lymphedema in the whole limb, both arms and legs,8,9 or short segments of the limb. 10 The aim of the present study was demonstrate the feasibility of using BIS to assess hand volume and, in particular, ECF.
Methods
Participants
An opportunistic sample of 20 males and 30 females was recruited from staff and students at the University of Sydney. Participants' characteristics are presented in Table 1. All participants reported being right dominant.
Results presented as mean±standard deviation.
The Human Research Ethics Committee of the University of Sydney approved the study and all participants provided written informed consent before testing commenced.
Bioimpedance spectroscopy of the hand
Bioimpedance spectroscopy was performed using an SFB7 impedance spectrometer (Impedimed Ltd., Brisbane). This is a tetra-polar electrode instrument using pairs of current drive and voltage sense electrodes. The positions of the current drive electrodes determine route of current flow along the length of the hand. The skin at the electrode sites was cleaned with an alcohol wipe and Ag–AgCl gel electrodes (Impedimed Ltd.), cut in half lengthways, were used. The drive electrodes were placed immediately proximal to the nail bed on the third finger and midway up the forearm. The sense electrodes were on the third metacarpal–phalangeal joint and in-line with the ulnar styloid process (Fig. 1). The inter-electrode difference was calculated as the linear distance, measured with a tape measure, between the sense electrodes. BIS measurements were performed on both the right and left hands.
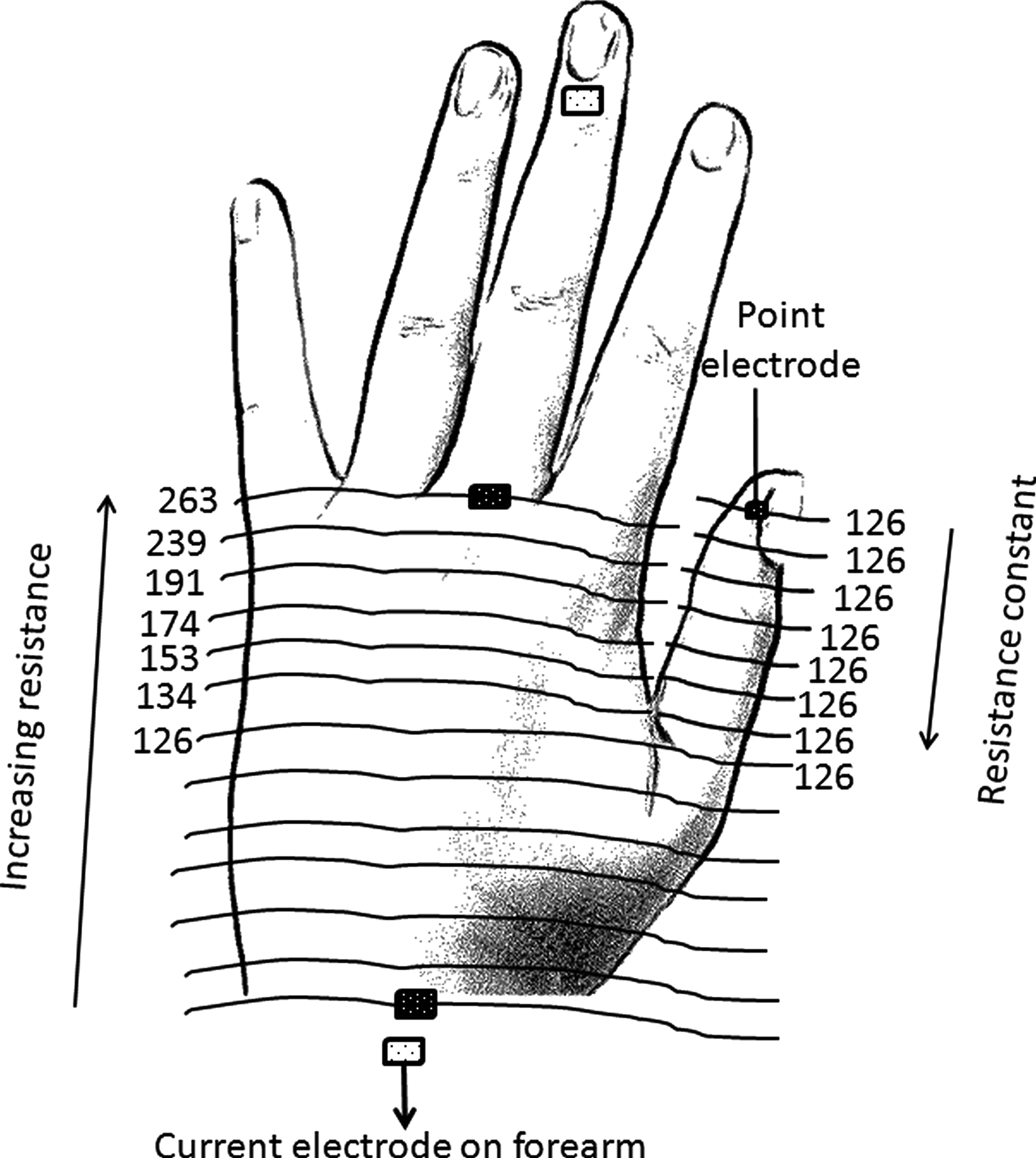
Locations of electrodes for bioimpedance spectroscopy of the hand illustrating the principle of equipotentials. Electrodes were located at the positions indicated. The voltage between the sense electrodes decreases as the distance between the sense electrodes decreases with all equidistant points having the same voltage (i.e., lying on the same line of equipotential). The voltage at any point along the thumb is equivalent to that at the base of the thumb. Key: Distal electrodes are the current drive electrodes; proximal electrodes are the voltage sense electrodes; lines indicate the lines of equipotential and the starting position of the probe electrode for mapping the lines of equipotential is indicated by arrow. Numbers are resistance measured at 5 kHz for a hand phantom.
Impedance of the hands was measured while participants were seated, arms extended horizontally and supported at heart height on a nonconductive table. All measurements were performed, at least in duplicate, after the participant had remained still in this position for three minutes.
Bioimpedance data were analyzed using software provided by the manufacturer (Bioimp V4.12.0.0) as described previously.7,9–11 Values for resistance at zero frequency (R0) and at infinite frequency (R∞) were determined.
Determination of hand region measured by bioimpedance spectroscopy
The thumb, being orthogonal to current track, was hypothesized to lie outside the measurement region. In order to determine the region of the hand being detected by BIS, a model phantom in the shape and dimensions of an adult hand was produced out of conductive material. BIS measurements were performed with the metacarpal–phalangeal sense electrode relocated to the tip of the “thumb”. Measurements were repeated with the metacarpal–phalangeal electrode progressively relocated at approximately 5 mm intervals proximally along the “thumb”. Needle electrodes were used for these studies. Finally, the electrode was relocated to the original metacarpal–phalangeal location and BIS measurements repeated as sections of the “thumb” were progressively removed to determine the effect on the impedance.
The results of the phantom studies were confirmed in vivo by measuring the impedance of a human hand. BIS measurements were performed with the metacarpal–phalangeal gel electrode being replaced with a fine metal electrode held in close contact with the skin. This electrode was placed on the tip of the thumb and impedance measurements obtained at 5 mm intervals as the probe was progressively moved along the participant's thumb.
Since the material used to manufacture the hand phantom was purely resistive, resistance only was recorded and data at 5 kHz is reported. The same response was seen for resistance at all frequencies monitored (3–1000 kHz).
Calculation of hand volume from BIS data
Calculation of hand volume excluding the thumb (palmar volume) from BIS data was based on the method for calculation of whole arm volume in lymphedema described previously by Ward et al.
11
R0 represents the impedance of the ECF and is directly inversely proportional to the volume of the ECF. R∞ represents the impedance of the total tissue fluid and is inversely proportional to the volume of that fluid. Ri, the intracellular fluid (ICF) resistance, can be computed from R0 and R∞ by Equation 1
ECF and ICF were calculated from R0, and Ri according to Equation 2:
where R represents R0 or Ri, and V is the volume of the ECF or ICF, respectively; ρ is the resistivity of the total fluid, ECF or ICF, respectively, and L is the inter-electrode distance. Total tissue fluid was calculated as the sum of ECF and ICF.
The resistivity values used were those reported by Ward et al. 11 The fat-free mass (FFM) was calculated from total fluid volume (ICF+ECF), assuming a hydration factor of 0.732. 12 Total palmar volume was calculated according to a simple two component model of tissue composition as FFM plus fat. 13 In an independent study of body composition using dual energy X-ray absorptiometry (DEXA), 14 hand fat was found to be 25.8±7.1% FFM and this mean value was used to compute total hand volume from the FFM using the density values reported by Brorson et al. 15
Measurement of hand volume by perometry
Hand volumes were measured with an opto-electrical perometer (Perometer, Juzo, Germany) using the protocol previously described. 16 Briefly, participants were positioned sitting with their arm in 90° abduction, palm down, and their middle finger touching the tip of metal plate on the hand rest (Fig. 1). Participants held their digits extended while keeping the thumb adjacent to the index finger.
These measurements of palmar volume include the thumb, unlike those obtained by BIS. Therefore, these data were corrected to provide an estimate of palmar volume only, according to the following equation:
where VolPalm is the palmar volume, VolPer is palmar volume plus thumb volume measured by perometry. This relationship was determined in an independent study using DEXA to measure total hand volume, thumb, and palmar volumes. 14
Effect of postural change on blood volume as measured by impedance
The impedances of both hands were measured whilst the participants had been seated with the arms supported horizontally for 3 minutes. After these measurements, participants were asked to raise their left hands to head height, where the arm was again supported in this position for 3 minutes and the impedance measurements of both hands repeated. This procedure elicits drainage of blood from the hand and arm.
17
The volume of blood drained from the hand during elevation (VolDrain) may be calculated from impedance measurements according to the Nyboer equation:
18
where ρb is the resistivity of blood (135 ohm.cm19); L is the inter-electrode length; ΔR0 is the change in R0 related to the change in blood volume; R0 is the resistance of the hand at baseline. The changes in blood volume of each hand during elevation of the left hand only were calculated.
Data analysis
Total palmar volumes, calculated from the impedance, were compared with the perometric volumes using Pearson's correlation, 20 Lin's concordance correlation, 21 and limits of agreement analysis. 22 Data for males and females were combined for these analyses.
Paired t-tests were used to determine the statistical significance of the effect of hand dominance on hand volume as well as the effect of positional change on the blood volume from impedance values.
Data were analyzed using SPSS for Windows (version 19, IBM), Microsoft Excel (2007), and Medcalc (version 12.1.3).
Results
Hand volume measured by BIS and perometry
The model hand studies showed, as hypothesised, that the impedance at all positions along the thumb remained constant at the value recorded at the base of the thumb (Fig. 2, symbol Δ). Similarly, the impedance of the model hand remained constant as the “thumb” was excised (Fig. 2, symbol ▴). These observations were confirmed by performing repeat BIS measurements using a fine metal electrode moved progressively along a participant's thumb. The measured impedance remained constant at the value measured at the base of the thumb (Fig. 2, symbol ○). These observations confirmed, in accord with the principle of equipotentials, 23 that measurements of impedance along the length of the hand from the metacarpal–phalangeal joint to the ulnar styloid define a hand volume that excludes the thumb.
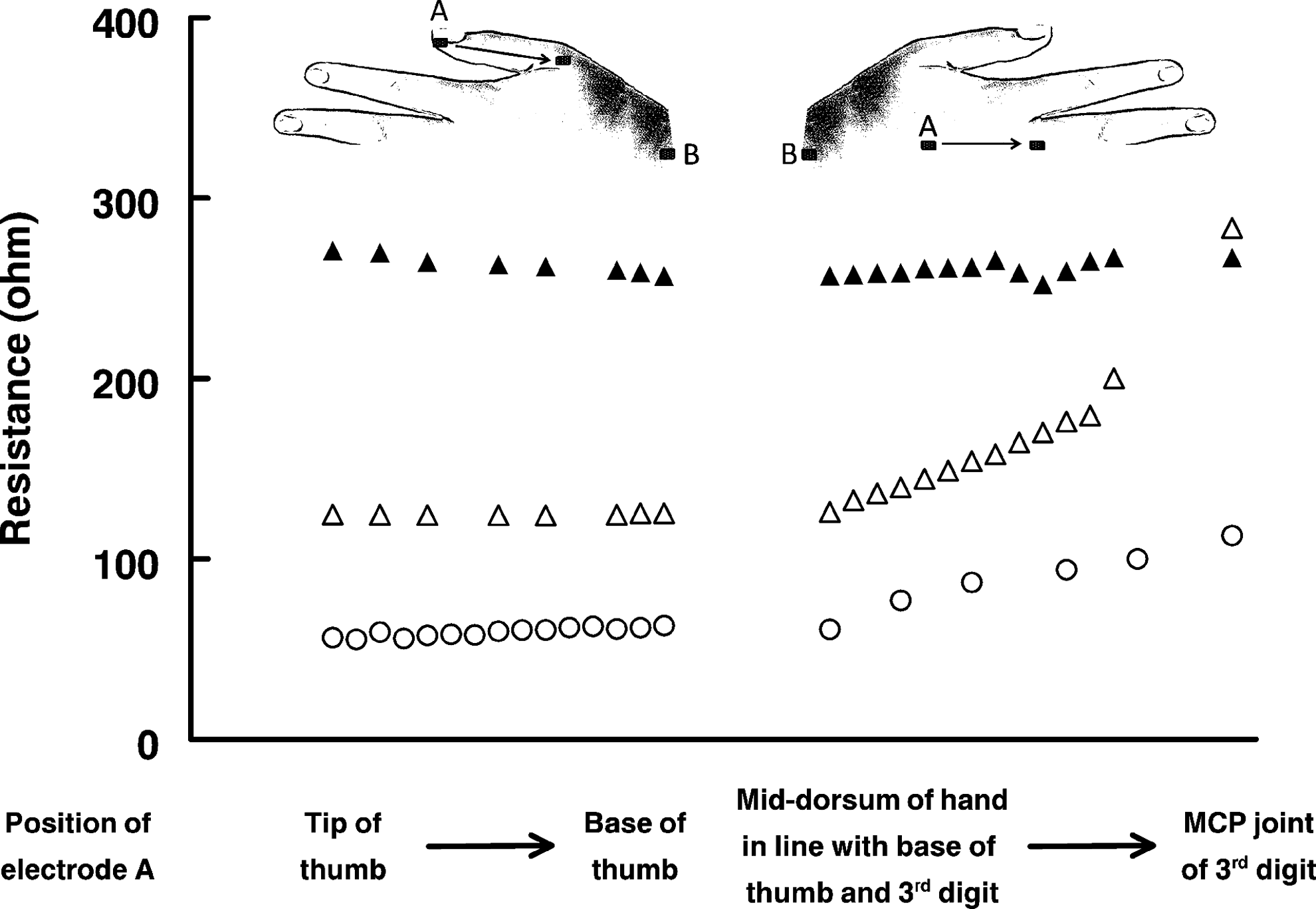
Region of the hand defined by impedance measurements along the mid-line of the dorsum of the hand. Key: ○, Change in resistance between electrodes A and B. Electrode A was relocated progressively along the thumb, and then along the dorsum of the hand to the metacarpal—phalangeal joint of the middle finger of a participant; electrode B was located at the ulnar styloid. Δ, Change in resistance between electrodes A and B of a hand phantom. Electrode A was located progressively along the “thumb” and then along the dorsum of the hand to the “metacarpal—phalangeal joint of the middle finger;” electrode B was located at the “ulnar styloid”; ▴, Change in resistance between electrodes A and B of a hand phantom as sections of the thumb were progressively excised. Electrode A located at the “metacarpal—phalangeal joint of the middle finger of a hand phantom”; electrode B was located at the “ulnar styloid.” MCP, Metacarpal—phalangeal.
Calculations of palmar volumes
Hand tissue fluid volumes, calculated from both bioimpedance and perometry measurements, are presented in Table 2. The group mean differences (biases) in total volumes between methods were 24.6±41.5 ml with limits of agreement of −106.1 to 56.8 ml (−47.0 to 25.2%) for the right hand and 14.5±40.0 ml with agreement limits of −92.9 to 63.9 ml (−43.2 to 29.7%) for the left hand. Total volume and those of the fluid compartments of the right dominant hand were consistently and significantly (p<0.001) larger than those of the left, nondominant hand.
Results presented as mean±standard deviation.
The volume of the palmar region computed from the BIS data obtained when both limbs were horizontal was highly correlated with that computed by perometry (Figs. 3A and B); Pearson's correlation coefficients of r=0.899 (p<0.0001) and r=0.877 (p<0.0001) for the right (dominant) and left (nondominant) hands, respectively. The respective concordance correlation coefficients, however, were rc=0.794 and rc=0.800, indicating that the data did not lie on the line of identity.
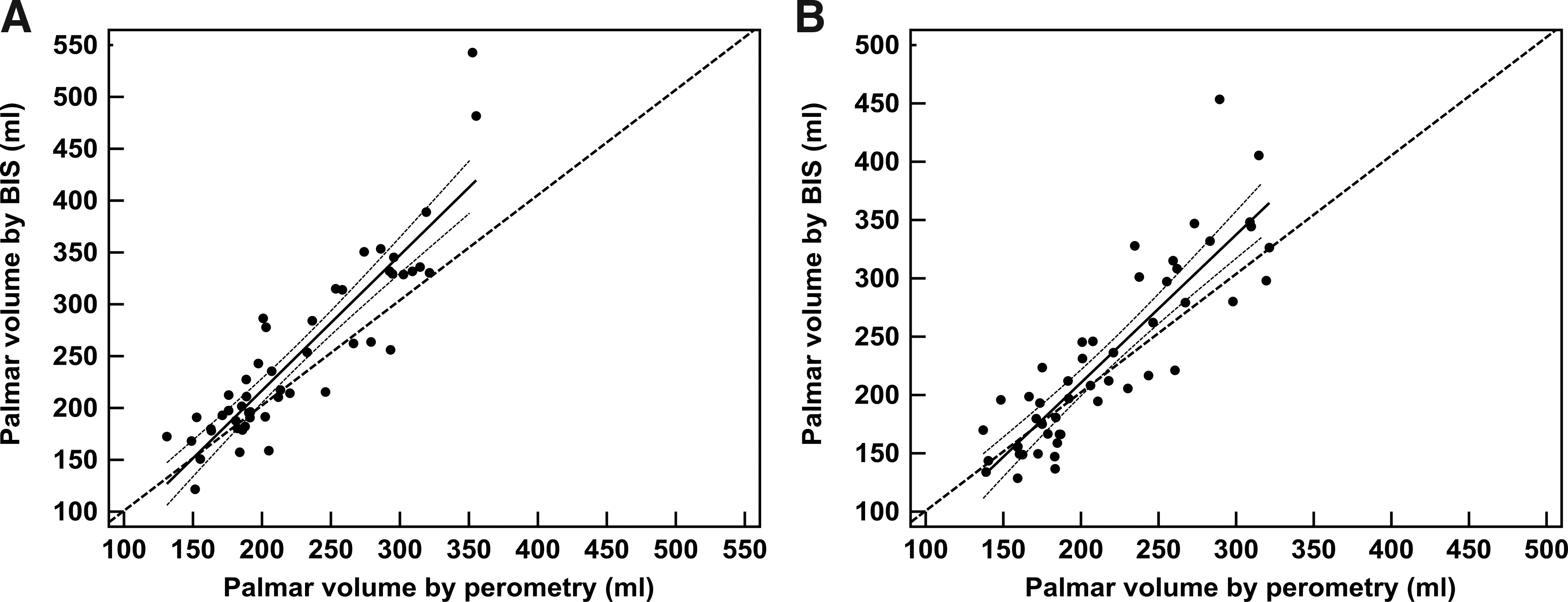
Correlataion of total hand volumes, excluding the thumb, measured by perometry and by bioimpedance spectroscopy. Key:
Effect of postural change blood volume in controls
Elevation of the left hand induced a 6.8±12.9 ml decrease in blood volume as measured by bioimpedance spectroscopy; the corresponding change in blood volume in the stationary right hand was 0.1±8.5 ml. This difference was significant on a paired t-test (p<0.001).
Discussion
The measurement of hand volume raises particular challenges. The irregular shape makes computation of volume from geometric measurements difficult. Typically, volume has been assessed by water displacement. Again, however, this approach is fraught with difficulties. For example, if the volume of the hand excluding the fingers only is required, this necessitates determining three separate volumes: the whole hand, the fingers, and the thumb separately, and computing the volume by subtraction. This approach, while feasible, is time consuming and inevitably has larger associated errors due to error propagation at each step of the procedure. In addition, it is not possible to use water displacement methods where the hand has wounds or dressings for fear of infection, although this has been overcome by the design of some water displacement devices. 24 In this study, we sought to adapt the impedance spectroscopy approach, successfully used to quantitate whole limb volumes, to the measurement of hand volume.
As hypothesized, the thumb was found not to be included in the region measured by bioimpedance using electrodes located along the mid-line of the dorsum of the hand. Similarly, this arrangement of electrodes does not include the fingers. It may be possible to measure individual finger volume using small electrodes located on the digit; indeed, the cylindrical form of a finger renders this a close realization of the underlying impedance equation for volume (Equation 2). However, the requirement for physical separation of the current and voltage electrodes would require the use of point source electrodes.
Hand volume was computed from BIS data using methods previously established in the whole limb or segments thereof. Palmar volumes derived from the BIS data were highly correlated with those determined from perometry measurements. They were, however, not identical, averaging approximately 8% larger than those calculated from perometry. It should be noted that perometry has been shown to provide hand volumes 7.5% larger than those determined by water displacement. 16 The volumes of the dominant hands were significantly larger than those of the nondominant hand. Although the slopes of the correlation lines differed from the lines of identity, these differences were small in magnitude and the regression equations for the data could be used to interconvert between the two methods. Considering the uncertainties in the assumptions required for calculation of volume from BIS measurements,11,15,18,19 this degree of agreement between the methods is notable. Despite this, however, the same caveats apply as to when using BIS to quantify arm volumes; namely that, owing to these uncertainties, for the present it would be prudent to use impedance ratios for comparisons between hands rather than computed volumes. 11
An advantage of the BIS technique over simple measurement of overall volume is its ability to measure the volume of tissue fluid compartments, ECF and ICF. Evidence of the sensitivity of the bioimpedance procedure in this regard was demonstrated by its ability to measure the change in ECF volume as blood, an extracellular fluid, was drained from the hand by the elevation. This sensitivity suggests that the method has the potential to detect small changes in the ECF space due to fluid accumulation in lymphedema. This has been well demonstrated in whole arms and legs; 10 whether this will also be the case for the hand awaits application of the method described here to subjects with lymphedema localized to the hand.
Footnotes
Author Disclosure Statement
Dr. Ward has consulted to ImpediMed Ltd. ImpediMed Ltd. had no involvement in the conception and execution of this study or in the preparation of the manuscript. Dr. Dylke was supported by a biomedical postgraduate scholarship from National Health and Medical Research Council (Australia). Dr. Kilbreath was supported by a career fellowship from the National Breast Cancer Foundation (Australia).
Authors' contribution: Ward conceived the study, undertook data analysis and had primary responsibility for manuscript preparation; Dylke undertook subject recruitment and data collection at University of Sydney, data analysis, and contributed to manuscript preparation; Kilbreath undertook data analysis and contributed to manuscript preparation.