
Abstract
Abstract
Background:
An increase in lymph flow from melanomas to draining lymph nodes has been reported in animal studies. It has been postulated that this contributes to metastatic potential of cancers. Data from animal studies are not easily extrapolated to humans; animal studies use immunosuppressed animals modified to overexpress lymphangiogenic growth factors, injected with human tumor cell lines, or manipulated to develop aggressive tumors. Human studies are required to investigate lymph flow in humans with cancers such as melanoma.
Methods and Results:
The present study aims to quantify the removal rate constant k (a measure of local lymph flow per unit volume of distribution of the radiotracer) from the vicinity of melanomas, benign nevi, and normal skin in humans in vivo using quantitative lymphoscintigraphy (QL). 16 patients with pigmented lesions underwent QL to quantify k near the lesion (kperilesion) and in contralateral matched normal skin (kcontrol). The lesions were then excised and, based on histological outcome, the patients were divided into two groups: benign nevus (n=9) and melanoma (n=7). There was no difference between kperilesion and kcontrol in either the benign naevus (p=0.29, paired t test) or the melanoma group (p=0.93). kperilesion in melanomas (0.233±0.123% min−1) was not increased relative to kperilesion in benign nevi (0.376±0.231% min−1, p=0.16, unpaired t test).
Conclusions:
We found no evidence for increased lymphatic drainage in melanoma relative to benign nevi or normal matched skin in humans.
Introduction
1. An increase in peritumor lymphatic vessel density, giving tumor cells greater access to lymphatic vessels (the conduits for metastasis to lymph nodes).4,5
2. An effect on immune cell infiltration and function in tumors, thus altering the immune response to cancer rather than simply influencing lymphatic density and function. 6
3. An increase in local lymph flow. Lymph flow from some malignant tumors is reported to be increased7–9 and is associated with higher rates of metastasis in animal models. 10 An increase in lymph flow could be mediated indirectly, via the effects of lymphangiogenic growth factors on blood vessels. In pathological conditions, VEGF-C and -D have angiogenic effects; 11 VEGFR-3, normally absent from blood vessels, is found on the microvasculature in melanoma.12,13 Lymphangiogenic factors could increase endothelial hydraulic conductance14–16 or expand the microvascular bed and increase solute and water flux in tumors, 17 thus increasing capillary filtration and lymph flow.
The postulated link between lymph flow and malignant progression is based on studies in mice only. Lymph flow studies often use immunosuppressed animals modified to overexpress lymphangiogenic growth factors and then injected with human tumor cell lines or manipulated to develop aggressive tumors. Studies on humans are essential if the relationship between lymph flow and metastasis is to be adequately investigated; to date, no studies have measured local lymphatic drainage in human melanoma in vivo, prior to excision.
Local lymph flow is measured in humans using quantitative lymphoscintigraphy (QL). Typically, a plasma protein of hydrodynamic radius 3.6–5.6 nm is labeled with a gamma-emitting radioisotope and injected as a small interstitial depot into the tissue to be studied. The radiolabeled macromolecules are taken up and cleared exclusively by lymphatic vessels. The lymphatic clearance of radiotracer from the depot is expressed as the removal rate constant, k, which equals the local lymph flow per unit volume of distribution of the radiotracer. 18 Technetium-99m (99mTc) bound to human immunoglobulin G (HIG) (Mw∼150,000, hydrodynamic radius∼5.6 nm) has been used extensively in QL to assess local lymph drainage in humans.18–21 Bilateral QL was carried out using 99mTc-HIG in the present study to test the following hypothesis: patients with melanoma (potentially metastatic) but not those with benign nevi will have higher interstitial fluid drainage rates from the perilesion area than in matched normal skin.
Patients and Methods
Research Ethics Committee approval was obtained (Protocol number 07/H0803/155) and all patients gave informed written consent. The study was carried out in accordance with the Declaration of Helsinki (2008) of the World Medical Association and was approved by the Administration of Radioactive Substances Advisory Committee of the United Kingdom (ARSAC). Patients with suspicious moles due for excision were recruited from the skin cancer screening clinics at St. George's and Kingston Hospitals, London, UK. Local lymphatic drainage was measured by quantitative lymphoscintigraphy (QL)18–21 in 16 patients prior to excision of the moles. The intradermal route for injection of radiotracer was chosen because moles are cutaneous and intradermal depots access initial lymphatics rapidly; thus, studies were completed in ∼60 min allowing for excision of the mole on the same day.18,22,23 Experiments were performed in a temperature-controlled laboratory. The patients acclimatized to their surroundings for 30 min beforehand. Skin temperature prior to commencement was 29.8±3.1 (SD)°C for the benign naevus group and 29.3±2.4°C for the melanoma group (YSI 4600 digital thermometer; Henlys Medical, Welwyn, Hertfordshire, UK). QL was performed at two skin sites. The first site for injection of radiotracer was selected 2–3 mm from the mole edge, and the second (control) site was the mirror image position on the opposite side of the body. A mirror image site is essential for the control, because the lymphatic density in the dermis and the lymphatic removal rate constant differ between anatomical sites and k shows bilateral symmetry.20,24 An injection of 99mTc-HIG (Technescan HIG, Mallinckrodt, Petten, Netherlands), 0.51±0.05 MBq (n=16) in 0.05 mL, was performed intradermally at each site using a steel microneedle of 0.2 mm outer diameter (Unimed, Zurich, Switzerland). A good injection into the upper dermis takes 30–60 s and is characterized by the sensation of resistance when giving the injection and the appearance of a raised, blanched, blister on the skin.
Radioactive counts from the depot were recorded using two 2″ sodium iodide scintillation detectors with a photopeak of 140 keV (digiBASE, Scintivision-32 software; Ortec, Wokingham, Berkshire, UK). The detectors were housed in cylindrical silver steel collimators (height 32.0 cm, outer diameter 10.9 cm, inner diameter 6.5 cm) at 20 cm above the apertures. The detector-collimator units (‘probes') were mounted on a trolley-based gantry system (Rotary Engineering, Wokingham) to enable precise three-dimensional positioning (Fig. 1). The probes were positioned vertically over the perilesion and control sites so that the midpoints of their apertures were directly over the depots and ∼1 mm above the skin surface. A circle was drawn on the skin around each collimator so that small movements by the patient during the experiment were easily noticed and could be corrected for by adjusting the position of the probe. Acquisitions (100 s) were performed every 5 min for 60 min. The lesions were then excised and, based on histological outcome, the patients were divided into two groups: benign nevus or melanoma (Table 1).

A patient undergoing quantitative lymphoscintigraphy. The mole is on the right upper chest; the control site is at the mirror image site on the left upper chest. The scintillation detectors (D) were housed in collimators mounted on a trolley-based gantry system (G). The detectors could be positioned over the skin sites using a 3-dimensional positioning mechanism.
BN, benign nevus; MM, malignant melanoma.
The radioactive counts (with the background level subtracted) were corrected for decay using the equation: N=N 0 e-γt, where N=corrected count, N 0 =uncorrected count, γ=decay constant for 99mTc (0.0001923 min−1) and t=time since injection (min). The corrected counts were then converted to fractions of the count recorded at time zero and the natural logarithms of the fractional counts were plotted against time (Fig. 2). The negative slope of the mono-exponential regression line through the points, fitted using linear regression analysis and multiplied by 100, gave the removal rate constant k (% min−1) (ie, the % of labeled tissue fluid volume cleared of the radiolabelled solute per unit time). 18 Although the slope of the regression line is negative, results for k are expressed as positive values throughout this article. Higher values for k indicate faster clearance rates.

Determination of the removal rate constant, k, in a patient with melanoma. Natural logarithms of the fraction of radioactive counts remaining were plotted against time from injection and the slope was fitted by linear regression analysis, giving k (% min−1). kcontrol was slightly faster than kperilesion in this patient.
Linear regression analysis was performed using Microsoft Excel; other analysis was performed using Prism 4.03 (GraphPad, La Jolla, California). Results are presented as the mean±standard deviation (SD), with the mean±standard error of the mean (SEM) in the figures. Student's paired t test was used to compare perilesion k (kperilesion) with control skin k (kcontrol) within each group. Between-group analyses (melanoma vs. benign nevi) were performed using the unpaired t test. Significance was accepted at p<0.05.
Results
Of the 16 patients, 9 were subsequently found to have a benign nevus and 7 were diagnosed with a melanoma (Table 1). None of the patients diagnosed with melanoma had metastatic melanoma at a mean follow-up time of 18 months (range 12–28 months).
In the melanoma group, the mean kperilesion (0.233±0.123% min−1) was almost identical to kcontrol (0.242±0.116% min−1); the slight difference was not significant (n=7, p=0.93, paired t test; Fig. 3). Likewise, there was no significant difference between kperilesion in the benign nevus group (0.376±0.231% min−1) and kcontrol (0.467±0.447% min−1, n=9, p=0.29, paired t test; Fig. 3). Although mean k in control skin in the benign nevus group appears faster than in the control skin of the melanoma group, the difference was not significant (p=0.22, unpaired t test). Excluding the outlying high value for kcontrol in the benign naevus group (1.563% min−1) resulted in a slower mean k of 0.330±0.187% min−1 (p=0.65 for kperilesion vs. kcontrol, paired t test). When the perilesion site in the melanoma group was compared with the perilesion site in the benign nevus group, there was no significant difference (p=0.16, unpaired t test), and any trend was towards a slower, not higher, value in the melanoma group.
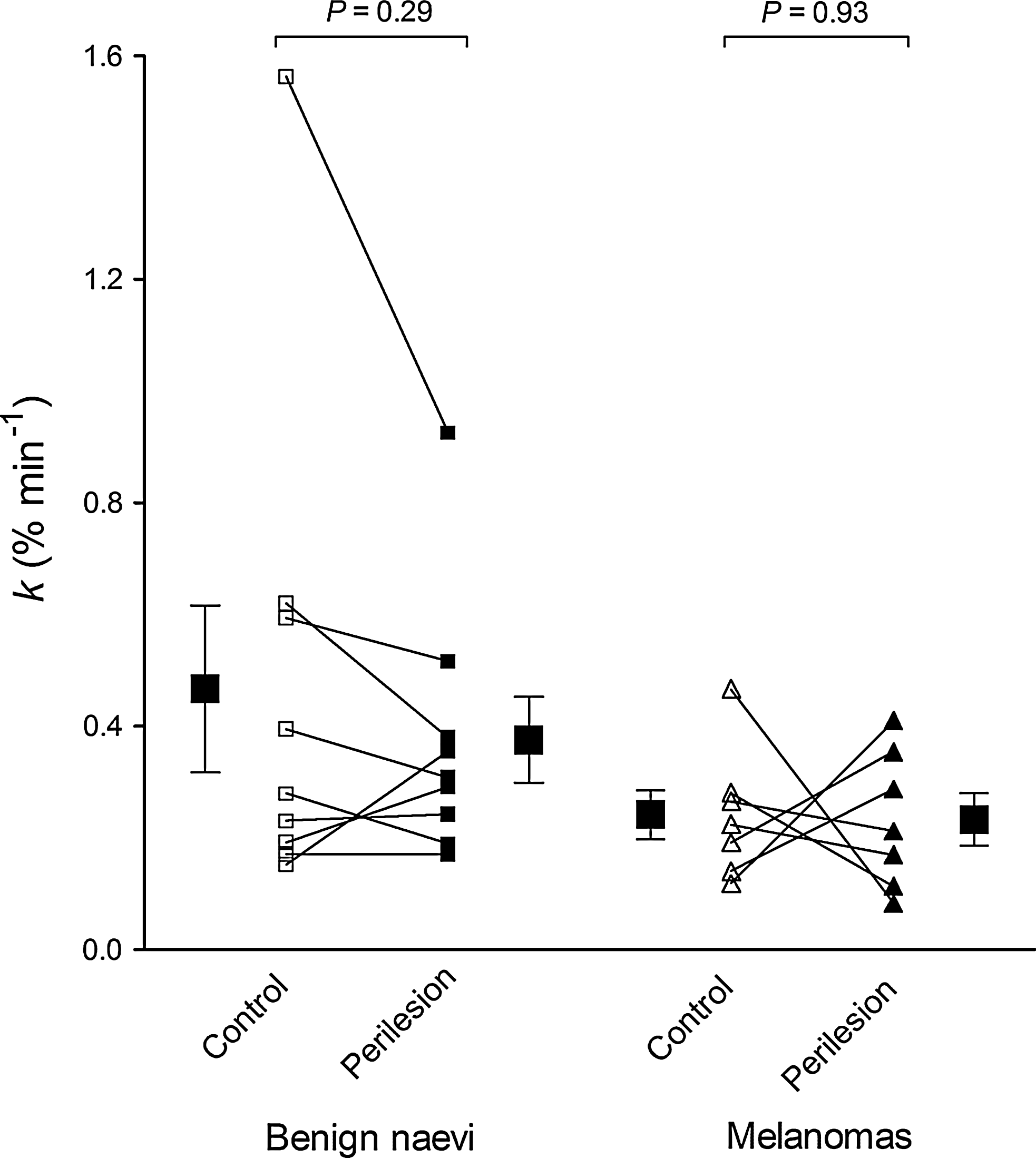
Paired plot of control and perilesion removal rate constant (k, % min−1) in benign nevi (n=9) and melanomas (n=7). Means and SEM are also shown. There were no significant differences between kperilesion and kcontrol in the benign nevus group (p=0.29, paired t test) or the melanoma group (p=0.93). There were similarly no differences between benign and malignant groups in kcontrol (p=0.22, unpaired t test) or kperilesion (p=0.16). In the benign nevus group, an outlying measurement accounted for the relatively high mean k.
Discussion and Literature Review
The results showed that there was no increase in macromolecular clearance rate from perilesion sites relative to matched normal skin in either melanomas or benign nevi. This indicates that, contrary to the tested hypothesis, lymph drainage rate is not increased in the vicinity of melanoma, despite the postulated link between lymph flow and malignancy.
The present study is, to our knowledge, the first study to employ QL to quantify lymph flow in humans with melanoma. The evidential basis of the lymph flow-malignancy link is derived mainly from studies in mice, some of which used QL to quantify lymph drainage. Higher removal rates were seen in mice with footpad melanomas compared with those without footpad tumors, interpreted as evidence of higher lymph flow from tumors relative to normal skin. 8 The arrival time of nanoparticles at a specified site along the lymphatic pathway after intradermal injection near B16-F10 melanomas in the mouse footpad has also been used as an indicator of lymph flow. 7 High levels of nanoparticles appeared within 2 min in the tumor-draining popliteal node, whereas in the contralateral control leg (no tumor) the popliteal lymph node signal was seen 30 min after injection. The authors concluded that lymph flow to tumor-draining lymph nodes is increased and may actively promote tumor metastasis. Other researchers have measured lymph velocity and lymphatic width in mice with tumors overexpressing VEGF-C. 10 Although lymph fluid velocity in the peritumor lymphatics of VEGF-C-overexpressing lesions was decreased, dilatation of these vessels resulted in a 40% increase in the total volumetric flow compared with lesions that did not overexpress growth factors. The study relied on the assumption that lymphatic width, as measured from a 2-D image obtained using lymphangiography, can be used to calculate cross-sectional area but this can only be done if the cross-sectional area is circular and not elliptical. Moreover, the authors used the maximum width in a lymphangion to calculate the cross-sectional area, but this did not take into account that cross-sectional area will vary along the length of a lymphatic.
In summary, lymph ‘flow’ studies often used immunosuppressed animals modified to overexpress lymphangiogenic growth factors and injected with human tumor cell lines or manipulated to develop aggressive tumors. If lymph flow in humans with cancers such as melanoma is to be investigated, human studies are required. Evidence in humans is very limited. In melanoma patients who had already undergone primary excision of the tumor, 99mTc-nanocolloid was injected intradermally around the scar site and its transit time to the sentinel lymph node measured. 25 Perilesion injections were also performed in patients with surgically untouched melanomas. It was found that none of the patients with slow drainage (defined as a transit time>20 min) were found to have a positive SLNB, whereas 14% of fast drainers were found to be SLNB positive. This study was taken as evidence that a fast transit is associated with metastatic potential, 26 but the study did not distinguish patients who had injections around surgical scars from those who had an intact melanoma, and surgery is known to disrupt lymphatic pathways. Therefore the study measured transit time to sentinel lymph nodes in a mixed population of patients, mostly with scars rather than melanomas. In addition, the sites of the injections were not taken into account; injections performed closer to draining lymph nodes may result in faster appearance times regardless of the lymph drainage rate.
Our study is the first study to measure lymphatic drainage rates around melanomas prior to excision in humans. For intradermal injections of 99mTc-HIG in the second webspace of the hand of healthy volunteers k is 0.125±0.015% min−1. 23 In our study, mean k in normal matched skin in the benign nevi and melanoma groups is 0.330% min−1 and 0.242% min−1, respectively. The higher values for k in normal skin in our study may be due to the different anatomical sites or a deeper injection by O'Mahony et al.; subcutis k is much slower than dermal k. 23 There was no statistically significant difference between perilesion and control k in either the melanoma or the benign nevus group, indicating normal lymphatic flows. This does not support the widely held belief that there is increased lymph drainage from tumor-bearing skin relative to normal skin, and that this contributes to metastatic potential.
In conclusion, although animal studies have led researchers to postulate that lymph flow is increased in cancer and that this contributes to metastatic potential, the studies should be interpreted with caution; lymph flow has not been measured directly in cancer, and animal models are often immunosuppressed and implanted with large volume aggressive cancers. Our study measured perilesion lymph drainage in humans with melanoma or benign nevi and compared this with matched control sites. We found no evidence for increased lymphatic drainage in melanoma, either relative to benign nevi or normal matched skin.
Footnotes
Acknowledgments
We thank the patients who participated in this research. We also thank Cancer Research UK for funding this project and Medical Physics, St George's Hospital, for technical support.
Author Disclosure Statement
The authors received funding from Cancer Research UK. No competing financial interests exist.