
Abstract
Abstract
We describe an unusual presentation of lymphedema due to constriction of the left upper extremity in a 71-year-old woman. The patient reported an onset of left upper extremity swelling 6 months prior to presentation, after she slept wearing a magnetic health bracelet. However, she was not accurately diagnosed until she visited our department. The diagnostic workup included a history and laboratory and radiologic findings, which were all normal except for the swollen upper extremity and findings on lymphoscintigraphy. She was diagnosed as suffering from chronic lymphedema due to constriction that only affected her left arm. She underwent complete decongestive therapy and achieved mild improvement of her swelling.
Introduction
Case Report
A 71-year-old female was admitted to the rehabilitation department for swelling of the left upper extremity (Fig. 1). The onset of swelling was 6 months prior to presentation to our institution. She reported having worn a magnetic health bracelet on her left wrist while sleeping one night. When she awoke the following day, she noticed that the left upper arm was swollen and that the bracelet had moved from her wrist to her upper arm and was constricting her upper arm. After removing the bracelet, she noted a superficial skin lesion and a small ecchymosis and swelling on the left upper extremity, but she thought that it would improve spontaneously and she did not seek treatment. However, 2 months later, the swelling persisted without improvement and she visited another hospital. She underwent vascular CT of the upper extremity and laboratory tests for evaluation of the vascular system, but she was told that she did not have a specific vascular problem. She wanted to seek proper treatment for reducing swelling of the left upper extremity, but did not know it. Therefore, she decided seek Oriental medicine and underwent moxa cautery on the left upper extremity several times. However, the swelling did not improve and actually worsened. Around the time of presentation, the swelling had increased with an accompanying sensation of warmth, a change in the color of the skin, and intermittent pain of the left upper extremity. These symptoms prompted her to visit our hospital.

A photograph of the patient's left upper extremity at the time of her initial presentation to our department. Swelling is seen on the left upper extremity. The photograph shows scars from moxa cautery (arrow), a thickened skin fold at the wrist, and redness on the forearm.
She had taken methimazole (Methimazole®) and levothyroxine sodium (Synthyroxine®) for hyperthyrodidism for 13 years and had taken telmisartan (Micardis®) and bisoprolol hemifumarate (Concor®) for hypertension for 10 years. She had a history of total hip replacement due to avascular necrosis of the right femoral head 7 years prior to presentation, and she had undergone an aortic valve replacement due to severe aortic stenosis 3 years prior to presentation, for which she took acetylsalicylic acid (Aspirin protect®). She did not have other relevant family or medical history for swelling and history of lymph node dissection on axilla area.
On physical examination, we did not see any mark indicative of constriction, hemorrhage, or change in pigmentation of the skin. Motor, sensory, and muscle stretch reflexes of both upper and lower limbs were absolutely normal, and there were no pathologic reflexes. The swelling extended from the fingers to 10 cm above the elbow. Hyperkeratosis and a scar from moxa cautery were seen on the forearm (Fig. 1). There was a deep skin fold at the wrist, but there was no pitting or swelling. There was an area of expanding erythema, warmth, and redness on the arm. These findings suggested stage III lymphedema with infection of the left upper limb.
The circumference of the right/left upper limbs, measured using the tape method, were 21.5 cm/27.9 cm, 23.5 cm/29.5 cm, 26 cm/31.8 cm at 10 cm distal to the elbow, at the elbow, and 10 cm above the elbow, respectively, and the circumference of the left upper extremity was, on average, 6 cm greater than that of the right upper extremity.
Laboratory analysis revealed that the erythrocyte sedimentation rate was increased to 91 mm/h (normal: 0–39), but the complete blood count, sedimentation rate, urinalysis, liver function tests, including the serum albumin concentration, the renal and the thyroid function tests, and rheumatoid factor were all normal.
We checked the echocardiogram to evaluate for congestive heart failure, and the exam showed no abnormal findings. Vascular CT of the left upper extremity did not reveal any pathologic findings, including deep vein thrombosis and vascular anomaly. The Tc-99m human serum albumin lymphoscintigraphy (Fig. 2) revealed the absence of flow at the left upper extremity and the axillary lymph nodes on the left.
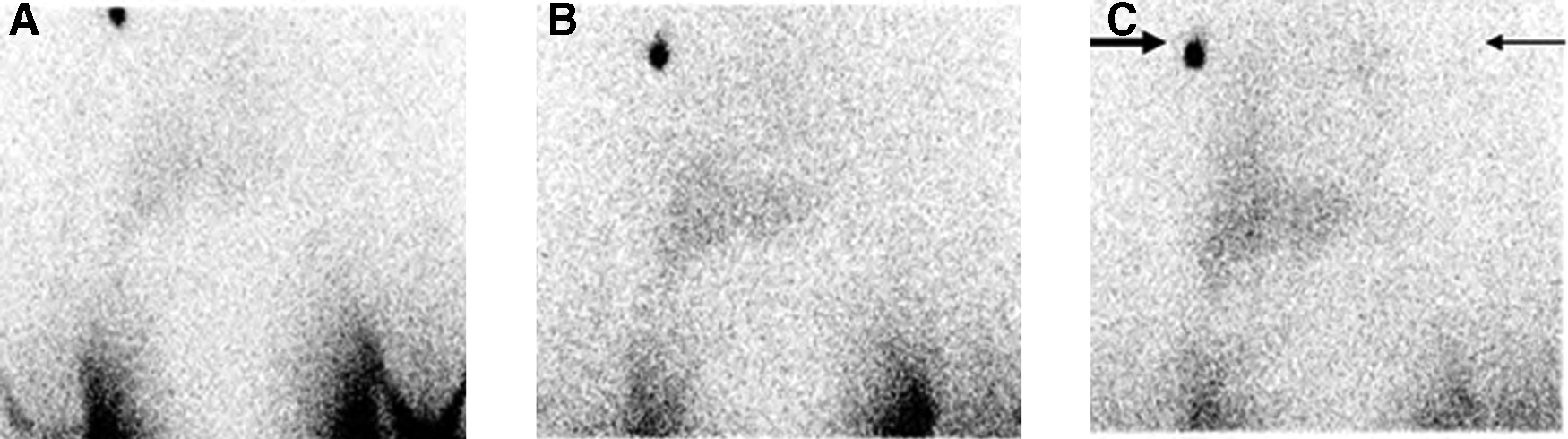
Upper extremity lymphoscintigraphy obtained
The diagnostic workup led to the diagnosis of chronic lymphedema due to constriction. In order to improve the infection, we prescribed vitis vinifera (Entelon®) and antibiotics and close observation until the warmth and redness on the swelling subsided. After 1 week of drug therapy, she underwent complete decongestive therapy (CDT) that consisted of skin care, manual lymph drainage, a compression bandage, and daily exercise.
During the treatment with CDT, we checked the circumferences of the left upper extremity using the tape method. The circumferences were decreased from pretreatment measurements by about 1.9 cm at 10 cm below the elbow, 1.0 cm at the elbow, and 1.0 cm at 10 cm above the elbow. The skin and subcutaneous tissue of the left upper extremity became smoother and softer, and the redness and sensation of warmth had resolved.
Discussion
Lymphedema is a condition in which lymph accumulates in the subcutaneous tissue because the transport power of the lymph system is decreased. It can be categorized according its cause into primary lymphedema and secondary lymphedema. Secondary lymphedema has obvious causes, such as surgery, radiation therapy, trauma, infection, malignant tumors, congestion, and chronic vein thrombosis, whereas primary lymphedema has no obvious causes.1–3 Congenital or genetic disorders of the lymph system cause primary lymphedema. The appearance of primary lymphedema becomes apparent with the presence of exacerbating factors, but prior to that time is often asymptomatic. 4
Worldwide, the number of people reaching old age is contributing to a rise in the prevalence of painful musculoskeletal conditions. 5 Magnetic bracelets have been used as a “cure” for arthritis since the beginning of the Common Era. 6 Some literature shows that participants who wear commercially available magnetic devices experience significantly improved pain outcomes compared with those who receive control devices.7–9 In Korea, many older people who are oriented toward Oriental medicine wear magnetic bracelets to improve their health conditions and reduce musculoskeletal pain. In our case, the patient typically wore the health bracelet without problems. Generally, people do not develop swelling secondary to compression from magnetic health bracelets because they stretch easily. However, our patient developed swelling in her arm.
Physical trauma may cause a reduction of the transport capacity of the lymphatic system at a level below the normal amount of lymphatic load. If the lymphatic system was healthy before the traumatic event, severe trauma with excessive scaring is usually necessary to cause post-traumatic secondary lymphedema. In a lymphatic system with an already reduced transport capacity, as in the case of congenital malformation, the balance between lymphatic load and transport capacity is often very fragile. Even minor trauma can cause the onset of post-traumatic primary lymphedema like this case. 4
In our case, we have two questions. The first question is whether her lymphedema represents simply a case of secondary lymphedema due to constriction. We feel that the pressure from the magnetic health bracelet and the duration and frequency that she wore it were not sufficient to develop mechanical insufficiency of the affected lymphatics. Her constriction was only present for one day. Therefore, we feel that she may have primary lymphedema with congenital dysplegia of her left arm. The force and pressure of constriction could be the aggravating factor that led to the development of lymphedema. The second question is why her swelling became chronic lymphedema, lasting more than 6 months. Usually, post-traumatic lymphedema does not become chronic. We considered that moxa cautery can induce infection that develops into an inflammatory process. Moxa cauterization has repeatedly been associated with several adverse events, such as burns, allergic reactions, and infections. However, the actual incidence of such adverse events is unknown. 10 Park et al. 11 reported that the magnitude of the risk associated with moxa cauterization is not well established and that caution should be employed when using it in routine health care.
To diagnosis lymphedema, we completed a full physical examination and history to rule out other risk factors. Patients with secondary lymphedema have a characteristic clinical history that often includes surgery, radiation therapy, trauma, or inflammation. However, it is very difficult to diagnose primary lymphedema because primary lymphedema, including aplasia, hypoplasia and hyperplasia of the lymphatics, is a silent disease. Furthermore, in some cases, lymphedema can occur after minor injury, such as an injection, sprain, burn, or bug bite, which would not significantly damage the lymphatics in most people. In our patient, we did not identify whether the pressure and constriction were enough to affect her lymphatics or there was underlying predisposition due to congenital dysplagia of the left upper extremity.
Lymphedema has recently become an interesting topic for physicians because in many patients lymphedema causes weakness, mild pain, and discomfort, as well as serious worsening of the quality of life. Many physicians have an interest in patients with lymphedema that is focused only on breast cancer-related lymphedema. 12 Only a few experts can diagnose and properly treat lymphedema due to other causes. Our patient did not receive a proper diagnosis and did not properly self-treat, as moxa cautery can lead to the development of infection in the arm and aggravate the symptoms.
The most important elements of lymphedema treatment are early diagnosis and early treatment, which can effectively prevent the progression of lymphedema. However, if diagnosis is delayed, as it was in this case, fibrosis of the lymphatic system prevents effective treatment. 13 So even though we tried to reduce the lymphedema, the effect was not complete. Early diagnosis and early treatment seems to be the best choice for these patients. Therefore, we are reporting a rare case of lymphedema due to constriction caused by a magnetic health bracelet. This case demonstrates that lymphedema can develop in older people, who often do not have adequate information about lymphedema. We recommend that physicians exercise caution in the treatment and diagnosis of swelling of the extremity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.