
Abstract
Abstract
Background:
The aim of this study is to investigate the effect of both inguinal exploration and deep venous thrombosis on lymphatic flow in an experimental model of unilateral acute obstruction of the femoral vein.
Methods and Results:
Eighteen male New Zealand White rabbits were the subjects of this study. The rabbits were divided into three groups; Group 1 (n=6, control), Group 2 (n=6, sham), and Group 3 (n=6, operation). After the lymphoscintigraphy was performed on the Group 1 animals, the rabbits in Group 2 and Group 3 underwent intervention. In Group 3, the femoral vein was clipped and excised. In Group 2, an inguinal incision was performed and the clip materials were placed beneath the femoral vein. After the surgical intervention, lower extremity lymphoscintigraphy by subcutaneous administration of Tc-99m nanocolloid was performed in dynamic and static manner in Groups 2 and 3 on the second, fifteenth and thirtieth days after the operation. Unilateral impairment of the lymphatic flow in the operated extremity was observed in Group 3 in the early and late postoperative period but unilateral lymphatic impairment was observed in Group 2 in only the late postoperative period.
Conclusion:
The lymphatic impairment in an operated extremity might be the consequence of surgical intervention rather than acute venous obstruction in cases where both situations are observed.
Introduction
Deep venous thrombosis is a life-threatening condition and also an etiology of secondary lymphedema. 4 Lymphoscintigraphic studies have shown that patients with varicose veins had impaired lymphatic function in the affected extremity 5 and that surgical correction of chronic venous impairment restored lymphatic function. 6 Although there are several reports about lymphatic impairment in deep venous thrombosis,7,8 to our knowledge this is the first study showing the effect of both acute deep venous thrombosis and inguinal surgery on the lymph flow. The aim of this study is to analyze first the effect of acute obstruction of the femoral vein and, second, inguinal surgery on the lymphatic flow of the lower extremity by lymphoscintigraphy in an animal model.
Materials and Method
Animals
Eighteen male 5–6-month-old New Zealand White rabbits approximately 3 kg in weight were the subjects of this study. The rabbits were divided into three groups; Group 1 (n=6, control), Group 2 (n=6, sham), and Group 3 (n=6, operation). A flow chart of the procedures that were performed in all groups is shown in Table 1. All animal protocols were approved by the Institutional Animal Care and Use Ethic Committee. The study was conducted according to National Institutes of Health Guide for the Care and Use of Laboratory Animals and Helsinki Declaration revised in 2008. None of the animals were sacrificed after the study.
LS, Lymphoscintigraphy.
Anesthesia
The animals were sedated by intramuscular administration of 35 mg/kg ketamine and 20 mg xylazine before all the imaging and surgical procedures.
Lymphoscintigraphy
After surgical intervention, lower extremity lymphoscintigraphy was performed in a dynamic and static manner in the control group and in Groups 2 and 3 on the second, fifteenth, and thirtieth days after the operation. Lymphoscintigraphy was performed by subcutaneous administration of 0.5 mCi (18.5 MBq) Tc-99m nanocolloid (Nanocoll,GE Healthcare Ltd, UK ) bilaterally from the dorsal face of the hind limbs (corresponding to the area between the second and third fingers) by a gentle massage without any extra maneuvers. Sequential images (each image 30 sec for 5 min) and static images on the fifth minute and the first hour were obtained by a double head SPECT Gama camera (GE Infinia 2, Israel) equipped with low energy all purpose collimator. The dynamic images were also analyzed. However, the flow curves did not provide sufficient data, probably due to the low radioactivity dose.
Interpretation of the images
The interpretation of the lymphoscintigraphy images was performed visually by an experienced Nuclear Medicine physician in blind manner in all animals. The absence of or reduction in tracer uptake in inguinal lymph nodes versus the healthy site or the bilateral absence of inguinal lymph nodes in the late phase images were accepted as impairment of lymphatic flow.
Surgery
The rabbits in the sham and the operation groups underwent the operation unilaterally. After the removal of the fur and surgical cleaning of the right inguinal region, exploration was performed by a 2 cm length incision just beneath the arcus inguinalis; the liberation of the femoral vein was performed later on. Since the femoral artery and vein are located superficially, the incision was small and the surgical procedure was performed with minimal interruption of the surrounding tissues in order to spare the lymphatic system. An additional procedure was not performed for the protection of lymphatic system. In the sham group, clipping materials were placed in the tissues adjacent to the femoral vein without clipping in order to protect the lymphatic system from the adverse effect of the surgery. In Group 3 two clips 1 cm apart were placed in the femoral vein and the flow was terminated.
Results
In the bilateral lower extremity, lymphoscintigraphy images of Group 1, bilateral lymphatic collectors, and inguinal lymph nodes were observed symmetrically. The presence of the lymph nodes and lymph collectors was clearly demonstrated both in the control group and in some of the animals from Group 2 and 3. This easily allowed us to discriminate the absence or reduction of the lymphatic collectors and lymph nodes from normal tracer distribution. Dermal backflow or other clues of lymphedema were not observed in any of the animals. Since the lymph nodes were not necessarily observed in the early phase (fifth minute) images, the late phase (first hour) images of the animals were interpreted. Two rabbits, one from Group 2 and one from Group 3, died after the first scintigraphy (Day 2) and two rabbits in Group 3 and one in Group 2 died after the second scintigraphy (Day 15). Unilateral impairment of lymphatic flow in the operated extremity was observed in Group 3 in the early and late postoperative periods (second, fifteenth, and thirtieth days) (Fig. 1a, b). However, unilateral lymphatic impairment was observed in Group 2 in the late postoperative period (Days 15 and 30)(Fig. 2a, b). Lymphoscintigrapy findings in Group 2 and 3 in the late phase images in postoperative Days 2, 15, and 30 are summarized in Table 2. Exceptionally, one rabbit from Group 2 had impaired lymph flow in all scintigraphies and one rabbit from Group 3 had impaired lymph flow in the late phase. The lymphatic flow in one rabbit from Group 3 improved in the second and the third scintigraphies after impairment in the early postoperative period (Day 2).
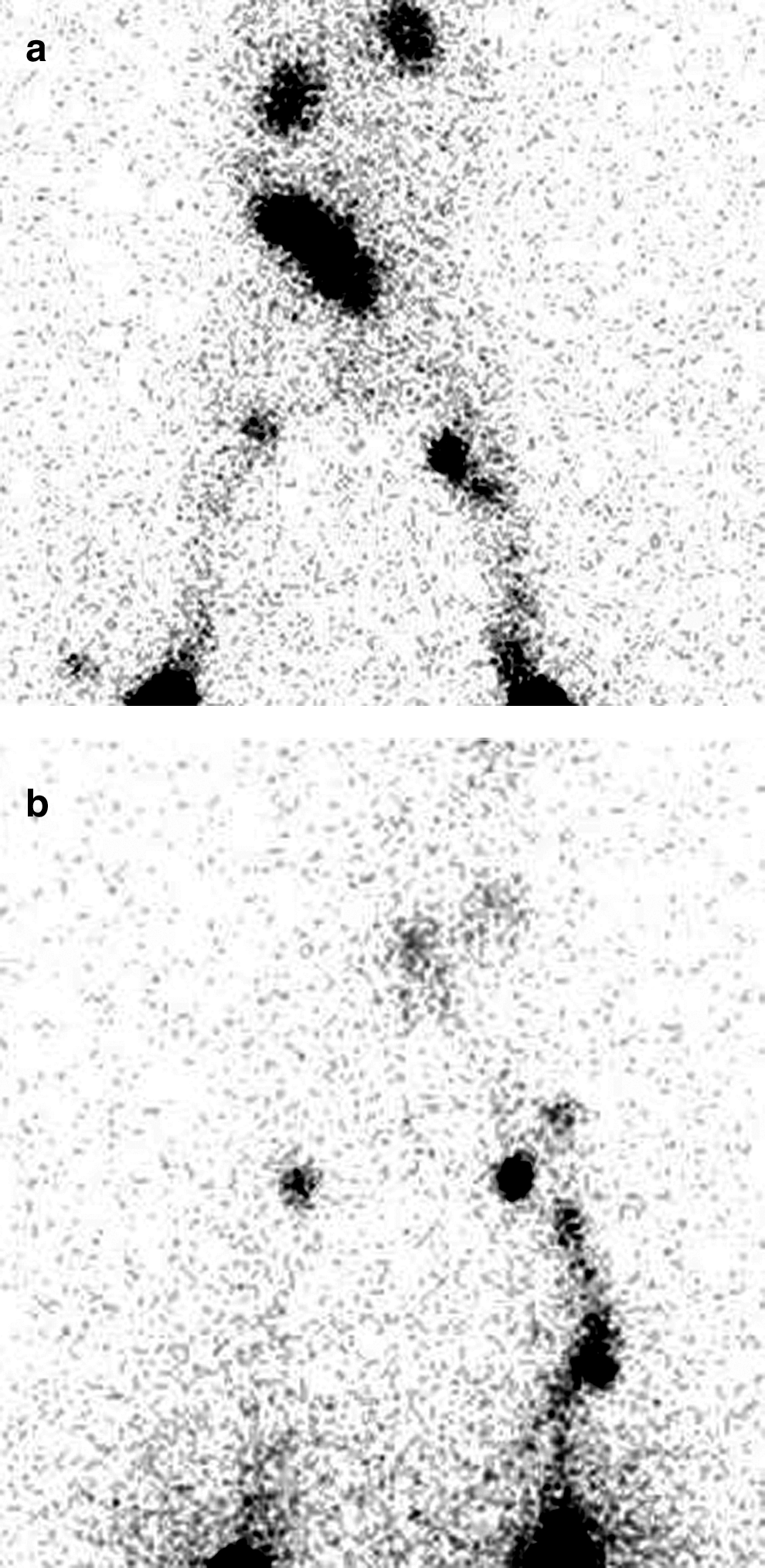
Anterior projection lymphoscintigraphy images of bilateral lower extremity in the late phase (first hour) in Group 3. Unilateral impairment in the inguinal lymph nodes in the operated site in all scintigraphy episodes (Day 2
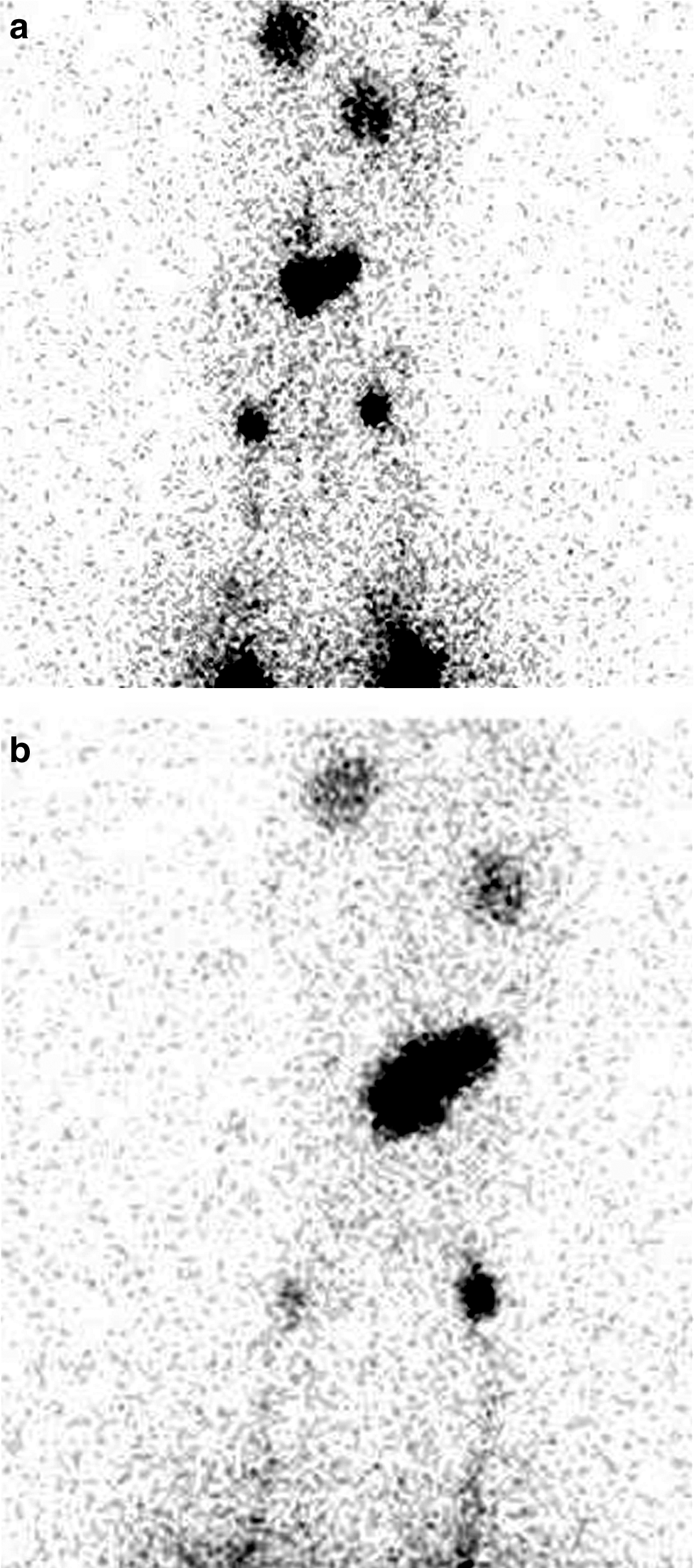
Anterior lymphoscintigraphy images of bilateral lower extremity in the late phase (first hour) in Group 2.
U refers to unilateral and B to bilateral visualization of the lymph nodes.
Discussion
According to our findings, surgical intervention is a factor in the impairment of lymphatic flow in the late postoperative period. Additionally, obstruction and interruption of the femoral vein causes impairment of the lymphatic flow in the earlier postoperative period. The possible mechanism of the lymphatic interruption during femoral vein occlusion might be related to the replacement of the lymphatic system with the venous system for the drainage function or more severe traumatic effects of the surgery. However, the late phase lymphatic impairment in Group 2 was probably due to adhesions after the surgery.
Lymphatic dissection related to cancer surgery causes lymphedema, especially in combined surgical management, and surgery in addition to radiotherapy.9,10 In a previous report, the rate of lymphedema complication in a group of patients who underwent pelvic and para-aortic lymphadenectomy for gynecologic malignancies was found to be 24%. 11 The same researchers suggested that if the surgical approach could be modified, the severity of lymphedema might be reduced. However, in our study, we documented that only surgical incision might be the cause of impairment of lymphatic flow. Additionally, Haaverstad et al. have shown that the rate of leg edema after femoropopliteal bypass surgery is not reduced by the modification of the surgical approach. 12
Since it has been demonstrated that noninvasive evaluation of the lymphatic system by lymphoscintigraphy is possible, 13 lymphoscintigraphy is the preferred method for the identification of the presence and the etiology of lymphedema. Previously the etiology of edema was classified as lymphedema and venous edema. 14 However, deep venous thrombosis has recently been included on the list of the etiology of secondary lymphedema. 4 Probably chronic or acute obstruction of the venous system produces lymphedema progressively, but the timing of the onset of lymphatic pathology is less clear. The information regarding the lymphatic changes in acute obstruction is insufficient as the important point in acute venous obstruction is the venous pathology, and thus lymphatic problems in acute venous obstruction have not been investigated. To our knowledge, this is the only study analyzing the lymphatic pathologies in an acute venous thrombosis model. In previous studies the negative effect of venous surgery in the lymphatic system has been demonstrated in saphenous segment resection for arterial reconstruction.6,14 Lymphatic impairment due to venous pathologies might be the consequence of the decreased drainage of extracellular fluid by the lymphatic system rather than a poorly functioning venous system.17,18 Another possible cause of lymphatic impairment in venous insufficiency might be the localization of the lymphatic collectors in close relationship with the main artery and the vein. Inflammatory reactions and mechanical factors might influence the lymphatic collectors and/or lymph nodes. Previous studies in humans who underwent venous excision operations (saphenous venous excision) have shown that the venous destruction causes lymphatic impairment. However, these studies did not include patients with total obstruction of the venous system.6,16 In our study, a total venous occlusion model was realized in rabbits. Furthermore, total and irreversible interruption of the femoral vein was performed in order to obtain total blockage of the venous system without any possibility of recanalization in order to mimic acute deep venous thrombosis. The aim of forming the Group 2 was first to exclude the effect of surgical trauma on the lymphatic system, and second to investigate the effect of surgery on the lymphatic system. Although we successfully demonstrated the surgical effect on the lymphatic system, we were unable to exclude the effect of surgery in a deep venous thrombosis group. We might only speculate that acute deep venous thrombosis of the femoral vein causes lymphatic impairment in early postoperative days. However, more severe surgery might be the main reason of the lymphatic blockage. Further studies are warranted in order to discriminate between these two pathologies.
The limitations of this study were the death of some rabbits during the study, the lack of late images (3 h after the injection), and the failure of the study to distinguish the traumatic effect of surgery from the effect of acute deep venous thrombosis in the lymphatic system.
As a conclusion, the incision only—and not the additional manipulation—might be the consequence of the impairment of the lymphatic system after surgical approaches. Additionally, acute deep venous thrombosis leads to lymphatic interruption in an earlier postoperative period than the incision does.
Footnotes
Author Disclosure Statement
The authors have no conflict of interest and no financial interests exist.
The study was supported by Firat University Scientific Research Projects.