
Abstract
Abstract
Primary lymphedema tarda is considered as a congenital disease with late presentation. Primary lymphedema tarda usually affects lower limbs, and primary lymphedema tarda of the upper limbs usually accompanies lower limb lymphedema. In the current case report, we present an 80-year-old male patient with isolated left upper limb swelling that lymphoscintigraphy imaging proved to be lymphedema.
Introduction
In the current case report, we present a patient with isolated primary lymphedema tarda of the upper limb, which was diagnosed by lymphoscintigraphy imaging.
Case Report
An 80-year-old male was referred for evaluation of isolated swelling of the left upper limb. He had progressive swelling of the arm over the last 6 months. There was no history of infection, rash, pain, weight loss, previous trauma, or surgery. The patient's past medical history did not reveal any relevant disease related to the arm swelling. His family history was unremarkable for any similar illness. On physical examination, he had isolated, painless, marked pitting edema of the left upper limb, involving hand and both forearm and arm without any lymphadenopathy. The radial, ulnar, and brachial pulses were palpable. He underwent various diagnostic procedures such as MRI, duplex ultrasound of the upper extremities, chest X-ray, and high resolution computed tomography of the thorax, as well as biochemical blood and serum tests. All diagnostic tests were within normal limits. Examination of the right upper limb and both lower extremities of the patient were completely normal. He was ultimately referred to the Nuclear Medicine Department for evaluation of lymphatic circulation and confirmation of lymphedema. 99m-Tc-phytate (1 mCi in two divided dose to each limb) was injected into the interphalangeal web spaces of both hands of the patient, and whole body images in anterior and posterior views were acquired 1 and 4 hours post-injection. We used a dual head gamma camera (ECAM Siemens) equipped with a parallel hole low energy high resolution collimator with matrix size of 128×128. On early and late static images of this patient, axillary lymph nodes of the left upper limb were not visualized (Fig. 1) and lymphedema of the left upper extremity was confirmed. The patient underwent conservative treatment and follow-up exam at 1 year revealed no other possible etiology for the lymphedema, which practically confirmed the diagnosis of primary lymphedema tarda. His lymphedema was markedly improved though.
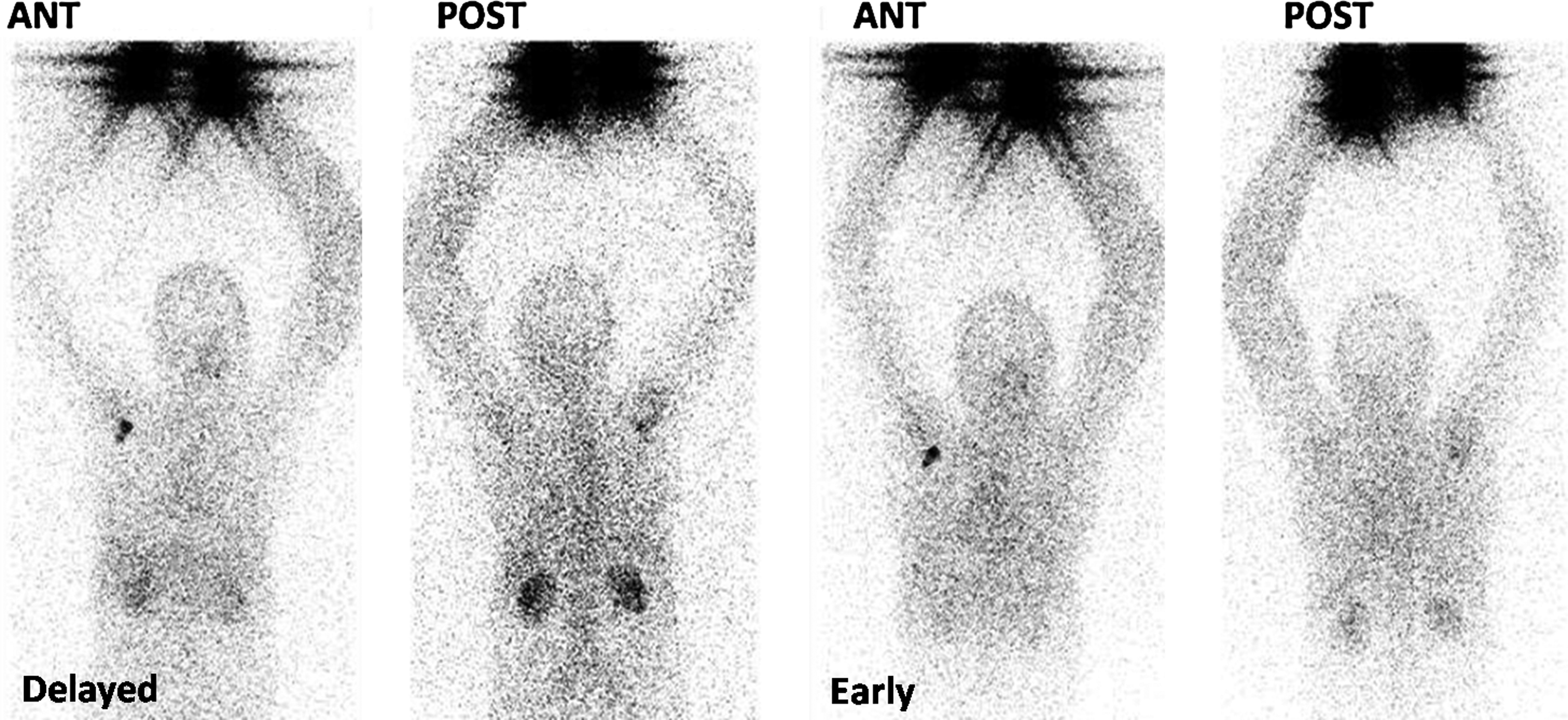
Early and delayed upper limb lymphoscintigraphy images. Note nonvisualization of axillary lymph nodes on the left side that confirms the diagnosis of lymphedema. There is also swelling of the entire left upper extremity.
Discussion
Primary lymphedema tarda of the upper extremities is a rare condition that has not been addressed enough in the medical literature. Diagnosis of lymphedema usually rests on clinical and physical examination and ruling out other causes of limb swelling.7,8 This is not always straightforward, and especially in the early phases of lymphedema presentation, diagnosis can be very difficult. Lymphoscintigraphy is a minimally invasive imaging method of lymphatic system evaluation which is very useful in this clinical situation.8–10 The diagnostic patterns of lymphedema on the lymphoscintigraphy images are: 1. Nonvisualization or delayed visualization of the draining lymph nodes in the inguinal or axillary area, and 2. dermal backflow of the tracer into the dermis. 11 Our case also showed nonvisualization of the axillary lymph nodes on the affected side, which confirmed the diagnosis of lymphedema.
In order to identify any possible etiology for the lymphedema, usually a long list of clinical and paraclincal examinations should be performed. Vascular disorders, systemic diseases (such as rheumatologic disorders), tumors, surgery, trauma, and infections, can cause secondary lymphedema. In our patient, the clinical and paraclinical examinations were unremarkable, and even after follow-up, no pathological condition could be identified. Finally the patient was diagnosed as isolated primary lymphedema tarda of the upper limb.
A few other authors also reported isolated primary lymphedema of the upper limbs.12–15 However, to the extent of our knowledge, only a case by Aslam et al. 15 had only upper limb involvement. They reported an 88-year-old African American male with isolated primary upper limb lymphedema. 15 They also diagnosed lymphedema on the basis of lymphoscintigraphy imaging, as we did in our case.
In a recent study by Vignes et al, lymphoscintigraphy and clinical features of primary upper limb lymphedema was described. 7 Their report is the largest on primary upper limb lymphedema thus far. In their nonhomogenous recruited patients (60 patients), 39 cases had isolated primary lymphedema of the upper extremities. The mean age of onset of lymphedema in their patients was 38.5 years with the range of 3–82 years. This shows that some of the patients in the Vignes et al. report had isolated primary lymphedema tarda of the upper limbs. Their final conclusion was: “Primary upper limb lymphedema appears later in life than lower limb lymphedema without sex predominance. Infectious complications are rare, and patients considered the lymphedema volume stable throughout life”. Vignes et al. 7 did not categorize their patients to precox and tarda and more information in this regard was not available.
Conclusion
Isolated primary lymphedema tarda of the upper limbs is a rare form of primary lymphedema, which can cause diagnostic uncertainty. Lymphoscintigraphy can be used reliably to confirm lymphedema in patients presenting with upper limb swelling in older age. Further classification into primary or secondary lymphedema needs thorough clinical and paraclinical examination.
Author Disclosure Statement
Drs. Shariati, Ravari, Kazemzadeh, and Sadeghi had no conflicts of interest or financial ties to disclose.