
Abstract
Abstract
Background:
To explore what factors affect volume of extracellular fluid (ECF) in the arm on the side of surgery pre- and postoperatively and to determine the value of knowing preoperative ECF volume for diagnosis of lymphedema postoperatively.
Methods and Results:
Women (N=516) with early breast cancer were assessed preoperatively and within 4 weeks postoperatively. Baseline measures included inter-arm ECF ratio, side of cancer, number of nodes involved, and other individual characteristics. Postoperative assessment included inter-limb ECF ratio and details from surgery. The postoperative ECF ratio was categorized as to whether it exceeded previously established thresholds, and the change in ECF was categorized as to whether it exceeded 0.1. Linear regression identified which factors explained the variance for preoperative ECF ratio and the change in ratio. Chi square analysis compared whether women categorized using thresholds were the same as those whose ratio increased >0.1 postoperatively. Postoperative ECF ratio was significantly higher than the preoperative ratio (p<0.001). Women whose ECF ratio exceeded previously established thresholds were not the same as those whose ratio increased >0.1 postoperatively (p<0.001). Only the side of surgery explained the preoperative ECF measure; extent of surgery and actual weight explained the change in ECF ratio.
Conclusion:
The ECF ratio preoperatively is not affected by nodal involvement. The change in ECF ratio is affected by the extent of surgery and body mass. Change from preoperative ECF ratio did identify more women at risk for lymphedema than reliance postoperatively on thresholds, supporting preoperative measures.
Introduction
The value of knowing the preoperative impedance ratio is unclear even though clinicians are advised to measure women preoperatively.3,4 If postoperative impedance ratios classify women appropriately according to established thresholds irrespective of preoperative measures, then preoperative measures with bioimpedance spectroscopy (BIS) would not be necessary. As lymphedema can develop anytime following surgery, what would be critical is for ongoing surveillance of women postoperatively to identify those women in whom the ratio exceeds the threshold. However, there is a possibility that these thresholds are not capturing all women in whom there are increases in ECF. In one of the first studies to describe the use of bioimpedance for early detection of lymphedema, it was also noted that an absolute change in the impedance ratio of 0.10 was clinically significant.5,6 Comparison of women identified by the criterion of change in impedance ratio greater than 0.10, with those identified as having lymphedema according to the population-based thresholds would determine whether preoperative ECF measures are required.
The aims of this study were therefore: 1) to describe the impact of breast cancer and nodal involvement on ECF, as measured by impedance, in the arm at risk prior to and following surgery; 2) to identify what factors affect the volume of ECF in the arm on the side of surgery preoperatively and in the early postoperative period; and 3) to determine the diagnostic value of change in impedance ratio from preoperative ECF values for detection of elevated ECF.
Materials and Methods
Design
Women were recruited after diagnosis of breast cancer but prior to breast surgery. In this longitudinal cohort study, participants underwent baseline assessment prior to surgery and a follow-up assessment within 4 weeks following surgery prior to commencing any adjuvant therapies. At the preoperative assessment, women reported on age, marital status, number of dependents, education, employment, smoking and alcohol consumption, level of physical activity, significant medical history, and regular use of vitamins and medications. The same questions about education, smoking, alcohol consumption, co-morbidities, and physical activity as in the NSW ‘45 and Up’ Study 7 were used. In addition, physical measures of height, weight, shoulder flexion range of motion, and upper limb impedance ratios were obtained.
Within 4 weeks after surgery, weight and impedance ratios were reassessed. In addition, details of breast and axillary surgery, as well as number of nodes involved and removed were obtained from medical records.
Participants
Women (N=516) were recruited from six cancer centers. To be included, women required a diagnosis of unilateral Stage I or II early breast cancer and be available for follow-up assessments. Women were excluded if they presented with metastatic disease, bilateral breast cancer, or were unable to speak or read English. Participant characteristics are reported in Table 1. The study was approved by the Human Ethics Committee at each of the institutions where the study was conducted and all women provided written informed consent.
Excluding woman with brachial plexus injury and with muscular dystrophy.
Metabolic equivalent of a task.
Assessment of ECF
Bioimpedance spectroscopy was used to determine the volume of ECF in the arm. At both measurement occasions, the impedance of each arm was determined using the principle of equipotentials which standardizes for limb length. 8 To measure impedance, women were positioned in lying, with arms positioned by the side and slightly abducted. Jewelry was removed, skin cleaned, and then electrodes placed on the dorsum of the wrists in line with the ulna styloid, on the dorsum of the hands below the third digit, and on the dorsum of the right foot. Data are presented as a ratio of impedance between arms (unaffected:at-risk). 9
Two devices were used to collect data: an SFB7 device and an XCA device (both from ImpediMed Ltd, Brisbane, Australia). The difference between the two machines is that the XCA is a single low frequency device, whereas the SFB7 is a multifrequency device. Previous research shows that the data collected from the XCA are highly concordant with that of SFB7 (rc=0.99; p<0.001). 10
Predictor variables
Variables which might impact on the ECF in the at-risk arm preoperatively included whether the tumor was on the participant's dominant or nondominant side, age, height, weight, body mass index (BMI), smoking, alcohol consumption, amount of physical activity preceding the diagnosis of cancer, and co-morbidities. In addition, the size of the tumor and number of nodes affected by cancer were determined from the medical records.
Variables that might impact on the ECF in the arm on the side of surgery postoperatively included the above as well as the type of breast surgery (wide local excision vs. mastectomy), axillary surgery (sentinel node biopsy vs. axillary node dissection), and number of axillary nodes removed.
Statistical methods
Impedance ratios pre- and postoperatively, as well as the change in ratio, were described. The pre- and postoperative measures were compared with a paired t-test, and limits of agreement analysis was used to assess any bias.
Women were categorized as to whether they exceeded the previously established thresholds for lymphedema: a ratio ≥1.134 for women in whom the surgery was on their dominant side and a ratio ≥1.106 for those in whom the surgery was on the nondominant side. 11 Last, women were categorized as to whether the absolute increase in impedance ratio exceeded 0.10. 5 Chi square analysis was then used to determine whether the same women were identified by both methods.
Multiple regression was used to identify which variables were related to the preoperative impedance ratio and to the change in impedance ratio. For each of the two regressions, participants' characteristics, details of cancer treatment, and physical and self-report measurements were analyzed separately using correlations for continuous data and univariate ANOVA for categorical data. Any variable associated with the outcome with p<0.25 was included in the initial multivariate regression model for that outcome. Variables not statistically significant at p<0.05 were then progressively eliminated, starting with the least significant, prior to checking the fit of the final model. Statistical analyses were performed using the IBM SPSS version 19 for Windows (IBM Corp. Somers, NY).
Results
ECF ratios and presence of swelling
The mean (standard deviation) preoperative impedance ratio was 0.999 (0.051), and ranged from 0.517 in a woman who had a brachial plexus injury affecting her dominant (right) arm to 1.173 in a woman with muscular dystrophy. Excluding these 2 women, 4 women in whom surgery was on the nondominant side exceeded the previously established thresholds, representing <1.0 % of the group (Fig. 1).

Effect of nodal involvement on preoperative ECF ratio. Irrespective of whether women had
Postoperative data were available for 476 (92%) of the cohort. Reasons for missing data included inability to access medical records (N=13), participants' time constraints (N=5), being too unwell (N=1) and missed appointments (N=22). Three women chose to withdraw from the study prior to their postoperative assessment. The mean (standard deviation) impedance ratio postoperatively was 1.015 (0.066), reflecting a small but significant increase from the preoperative ratio of 0.016 (0.061) (paired t-test; t=−5.8; p<0.001; Fig. 2). However, there was poor concordance between the measures (rc=0.453). As this cohort included 58% who only underwent sentinel node biopsy, we repeated the analysis with the subgroup of women who had undergone axillary node dissection (n=183). In this subgroup, the bias was low (3.0%; 95% confidence intervals (CI): −11.0–17.0%), with poor concordance between the measures (rc=0.42).

Histogram of change in ECF ratio from pre- to postoperative assessment. Dashed vertical line indicates an absolute change of 0.1, which is considered clinically significant.2
The impedance ratio increased by ≥0.10 in 32 women (7%) and 24 women exceeded the previously determined impedance threshold 11 following surgery. However, the women identified by the two approaches differed significantly (χ2=148.2; df=1; p<0.001; Fig. 3).
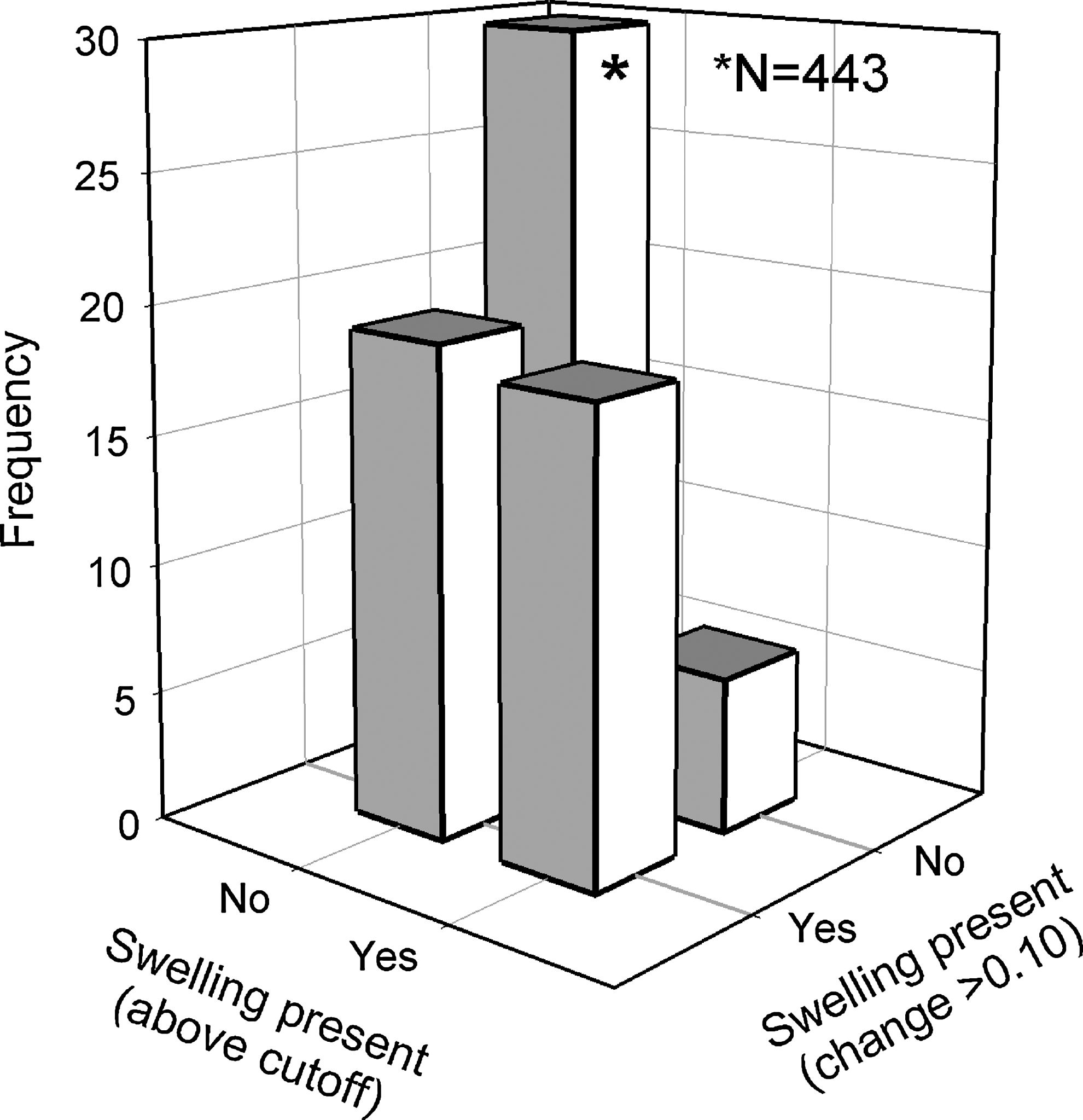
Comparison of classification of women at risk of lymphedema using previously published thresholds and change in ECF ratio >0.1. Note that 443 women scored ‘No’ for both classification schemes. Use of previously established thresholds did not identify 18 women whose ECF ratio increased by at least 0.1 following surgery.
Only 17 women were identified by both approaches as having significant change in their impedance ratio. For women in whom surgery was on their nondominant side, 3 women with postsurgery impedance ratio ≥1.106 had not changed by ≥0.1, and 4 women whose ratio did increase by ≥0.1 were still below the previously established threshold. For women in whom surgery was on the dominant side, the ratio did not exceed 1.134 for 11 women in whom it had increased by ≥0.1. In another 4 women, the impedance ratio exceeded 1.134 but had not changed by ≥0.1.
Factors affecting preoperative impedance ratio
The preoperative impedance ratio was not correlated with age (r=−0.06), absolute weight (r=-0.04), BMI (r=−0.05), size of tumor (r=0.04), or the number of nodes affected by cancer (r=0.04; Fig. 1). In addition, the XCA ratio was not significantly different in the presence of any of the co-morbidities assessed (p=0.8 for depression to p=0.96 for thyroid-related problems).
In the subgroup of women with nodal involvement (n=199; 39%), the median (inter-quartile range) number of nodes involved was 2 (1 to 5). In addition, bivariate analysis for the whole group revealed that smoking, alcohol consumption, and exercise did not affect the preoperative impedance ratio. To examine the effect of dominance on impedance ratio, two women with previous upper limb impairments (childhood brachial plexus injury and muscular dystrophy) were removed. The side on which the cancer presented affected the impedance ratio, with the ratio significantly higher in women in whom the dominant side was affected (1.01±0.045; 95% CI 1.01–1.02) compared to 0.99±0.054 (95% CI: 0.979–0.991) for women in whom surgery was on their nondominant side (Fig. 1; F=44.4; p<0.001).
The two variables included in the linear regression were age and side on which cancer presented. Following removal of age, as it did not contribute to explaining the variance, the only predictor that was related to the impedance preoperative ratio was the side on which the cancer presented, and explained 6.7% of the variance.
Postoperative change in ECF
Bivariate analysis revealed that the change in impedance ratio was related to type of breast surgery (F=6.4; p<0.012) and axillary surgery (F=13.4; p<0.001), and number of nodes removed (r=.21; p<0.01); but not related to side (dominant or nondominant) of surgery (F=1.62, p=0.197), age (r=0.04; p=0.355), or exercise (r=−0.03; p=0.51). In addition, change in impedance was related to absolute weight (r=0.17; p=0.001) and BMI (r=0.17; p<0.001).
Linear regression revealed that change in impedance ratio was significantly related to absolute weight, type of breast surgery, and the number of nodes removed. Women who were heavier and had more extensive surgery had significantly greater change in their impedance ratio. However, overall, this model explained very little of the variance (r=0.28; p<0.001).
Discussion
This is the first longitudinal study in which women were assessed preoperatively with bioimpedance spectroscopy. Prior to surgery, <1% of women were above the ‘threshold’ 11 for lymphedema, but following surgery this percentage increased to 5%. Whereas side of surgery explained the preoperative BIS measure, weight and the extent of surgery explained some of the change in postoperative BIS measure.
The preoperative impedance ratio was not related to number of nodes involved with cancer. Women with up to 40 nodes involved were within the normal range. What these findings indicate is that physiologically, the body adapts to changes that occur over time on the lymphatic system. However, for women predisposed to development of swelling, 12 the sudden impact of surgery can compromise removal of interstitial fluid through the lymphatic system, leading to an increase in ECF. It is likely women with high lymph flow in the arm, such that the lymphatics are already working near capacity, are at risk for significant increase in ECF. 12 Clearly, we have yet to identify predictors of increased flow as the regression model for change in ECF only explained 8% of the variance.
The impedance ratio preoperatively, not surprisingly, was related to side on which the cancer presented. Impedance is inversely proportional to volume of ECF; as the dominant limb typically has more muscle than the nondominant limb, 13 the preoperative impedance ratio was higher when surgery was on the dominant side than on the nondominant side. The impedance ratio and variance for women with cancer on the dominant side were similar to those reported by others.11,14,15 However, the variance for women in whom their cancer was on the side of the nondominant limb was slightly higher, although the means were similar. In our cohort, excluding one woman with past history of brachial plexus injury, the ECF ratio was 0.987 (0.045) compared to 0.986 (0.040). As the thresholds were based on three standard deviations above the mean, this small difference in variance would elevate the threshold to 1.122 compared to 1.106. This value approximates that of the dominant limb more closely, perhaps reflecting the decrease in dominance effect in an older population. 16
One of our aims was to determine the importance of obtaining a preoperative impedance ratio. If the thresholds were effective in categorizing women with significant change in impedance, then it would not be necessary to obtain this measure. However, there was a significant difference between using thresholds and an absolute increase in the impedance ratio by ≥0.10 and our data show that, where possible, the preoperative data are important (Fig. 3). While the thresholds do provide an indication of what is outside the normal range, they fail to identify those women in whom the ratio was initially low (i.e., those who may be 3SD below the mean).
Factors that contributed to the change in the ECF in the arm on the side of surgery were the magnitude of surgery and the weight of the patient. Not surprisingly, the more extensive surgery was associated with significantly larger change in the impedance ratio. The woman's weight at time of surgery was also positively associated with the change in the ratio. Studies dating back to 1957, 17 when breast cancer surgery was more extensive, identified obesity as a predictor of lymphedema. However, even with less extensive surgery, obesity is consistently identified as a predictor of lymphedema in well-designed prospective studies.18–23 The increase in ECF identified postoperatively in the current study is likely not lymphedema but rather transient changes in swelling. 3 However, the changes identified at this time may predispose women to progress, and over time, develop this condition.
Several factors may predispose obese woman to elevated impedance ratios and eventually to lymphedema. Adipose tissue in the arm may provide a physical obstruction with fatty deposits surrounding the vascular system increasing resistance to flow without causing any physical damage to vascular or lymphatic vessels. 24 Another possibility is that, as obesity is associated with decreased levels of physical activity, 25 it is the low levels of physical activity that increase risk of lymphedema. A prospective study that regularly assessed for lymphedema using BIS found that sedentary women were six times more likely to develop lymphedema than women who performed sufficient exercise. 26 Alternatively, it may be related to exercise undertaken by the ‘at risk’ arm. In our recently completed study, upper limb resistance training was protective against elevated BIS ratio in the early postoperative period. 27 Other possibilities include the need for more extensive surgery due to the presence of adipose tissue. 28 Alternatively, fat necrosis may result in delayed healing and secondary infection with regional lymphangitis resulting in lymphatic obstruction. 29 Further research focusing on obese women is required to understand why these women are preferentially at risk for swelling and eventually lymphedema.
In conclusion, the impedance ratio preoperatively is not affected by nodal involvement but by arm dominance. The ECF ratios preoperatively are in the same range as women without breast cancer or lymphedema. The change in impedance ratio, however, is affected by the extent of surgery and body mass. Last, use of thresholds to identify women at risk of lymphedema postoperatively did not capture all women in whom there was an increase of their ECF ratio by >0.1; preoperative measurements of impedance ratios in lymphedema detection therefore do have diagnostic value and where possible, should be obtained.
Footnotes
Acknowledgments
We thank the research and clinical staff who assisted with recruitment and data collection.
Author Disclosure Statement
SLK is a National Breast Cancer Foundation Career Research Fellow. Dr. Ward has consulted to ImpediMed Ltd. ImpediMed Ltd. had no involvement in the conception and execution of this study or in the preparation of the manuscript.
This project was supported by a grant from Cancer Australia and National Breast Cancer Foundation.