
Abstract
Abstract
Background:
Lymphatic drainage of renal cell carcinoma is unpredictable. Renal lymphatics directly joining the thoracic duct without traversing any lymph nodes have been described in cadaver studies, yet to date, this has never been visualized using functional imaging in vivo.
Methods and Results:
Patients with renal tumors <10 cm (cT1–cT2) and clinical absence of metastases (cN0, cM0) took part in a prospective institutional review board approved study investigating sentinel node mapping. After ultrasound-guided percutaneaus intratumoral injection of 99mTc-nanocolloid (0.4 mL, 200 MBq) the day before surgery, planar sequential lymphoscintigraphy was obtained after 20 min and 2–4 h. Subsequently, SPECT/CT imaging was performed. Of 42 patients, 4 showed early lymphatic drainage following the course of the thoracic duct on lymphoscintigraphy and SPECT/CT images. In one patient, this was observed without any retroperitoneal lymph node interposition. In relation to patients with sentinel nodes on SPECT imaging the frequency of this drainage pattern was (4/22) 18.2%.
Conclusions:
SN mapping of renal tumors using functional imaging modalities such as lymphoscintigraphy and SPECT/CT enables identification and sampling of sentinel nodes outside the area of routine dissection. Direct aberrant drainage through the thoracic duct can be observed in vivo as demonstrated in this study. This may support a hypothesis for certain anatomical metastatic sites and the failure to demonstrate a survival benefit of retroperitoneal lymph node dissections in renal cell carcinoma.
Introduction
L
Lymphatic drainage from the kidney is generally considered to be directed towards the hilar region branching off into the paracaval, interaortocaval, or para-aortic retroperitoneal lymph nodes, depending on the tumor side. However, the lymphatic drainage of renal tumors may not always follow the known pattern, as has frequently been found for other tumor entities. We previously described that the majority of SNs in renal cell carcinoma (RCC) were not located in the hilar region, but had a retrocaval, interaortocaval, or para-aortic predilection. 3 In addition, renal lymphatic tributaries directly joining the thoracic duct without traversing any lymph nodes have been described in cadaver studies.5,6 However, direct lymphatic drainage through the thoracic duct has never been visualized using functional imaging in vivo to date. The purpose of this retrospective analysis was to evaluate the frequency of renal lymphatic drainage patterns along the thoracic duct in a series of patients from a feasibility study and an ongoing phase II imaging study using lymphoscintigraphy and SPECT/CT.
Material and Methods
Patients
The patients described in this study have been extricated from a series of 42 patients who underwent SN mapping for kidney cancer in a feasibility study and an ongoing phase II imaging study. Both studies were approved by the local ethical committee and registered under www.ccmo.nl (NL16017.031.07; NL26406.031.08). The ongoing phase II trial is designed to detect a 25% location of SNs on imaging outside the locoregional retroperitoneal lymphatics (alpha of 0.05, power of 80%) and will require 40 patients. All patients signed written informed consent and were informed about the objective of the studies. Inclusion criteria were as follows: renal tumor <10 cm (cT1–cT2), no metastatic disease on imaging and clinical examination (cN0, cM0), age >18 years, life expectancy >3 months, WHO performance status 0 or 1 and fit for surgery). Patients with prior systemic treatment were not included.
Lymphatic mapping
The radiocolloid (99mTc-nanocolloid) was injected percutaneously (0.4 mL, approximately 200 MBq) into the tumor guided by ultrasound the day before surgery as described previously. 7 Planar lymphoscintigraphy was obtained after 20 min and 2–4 h. Subsequently, SPECT and low-dose CT were acquired (SymbiaT, Siemens, Erlangen, Germany), and corresponding axial 2 mm slices were generated. After correction for tissue attenuation and scattering, the SPECT and CT images were fused (Osirix Dicom Viewer). Using multiplanar reconstruction, fused images were displayed together with SPECT and CT and cross-reference lines allowed the navigation between axial, coronal, and saggital views. Additionally, fused SPECT/CT was three-dimensionally displayed using volume rendering assigning different colors to vessels, muscle, bone, skin, and radioactive lymph nodes. The nodes appearing on (early) planar lymphoscintigraphy were considered to be SNs. Nodes appearing on the delayed images in the same stations were considered to be second echelon nodes.
Intraoperative procedure
The approach for renal surgery was decided per case. SNs were intraoperatively localized using a gamma ray detection probe (Neoprobe, Hamburg, Germany) in combination with a portable gamma camera (Sentinella, Valencia, Spain) as previously described. 7 Patent blue was not used. SNs were separately excised, followed by a retroperitoneal LND. As all three patients were part of aforementioned feasibility trial, only SNs that could be approached through the access for renal surgery were removed following the study protocol. 3
Results
Of 42 patients, 4 showed early lymphatic drainage following the course of the thoracic duct on lymphoscintigraphy and SPECT/CT images. In 20 patients, no SN could be visualized by SPECT/CT. In 3/20 patients, hilar active nodes were found during surgery. In relation to patients with SNs on SPECT imaging the frequency of this drainage pattern was (4/22) 18.2%.
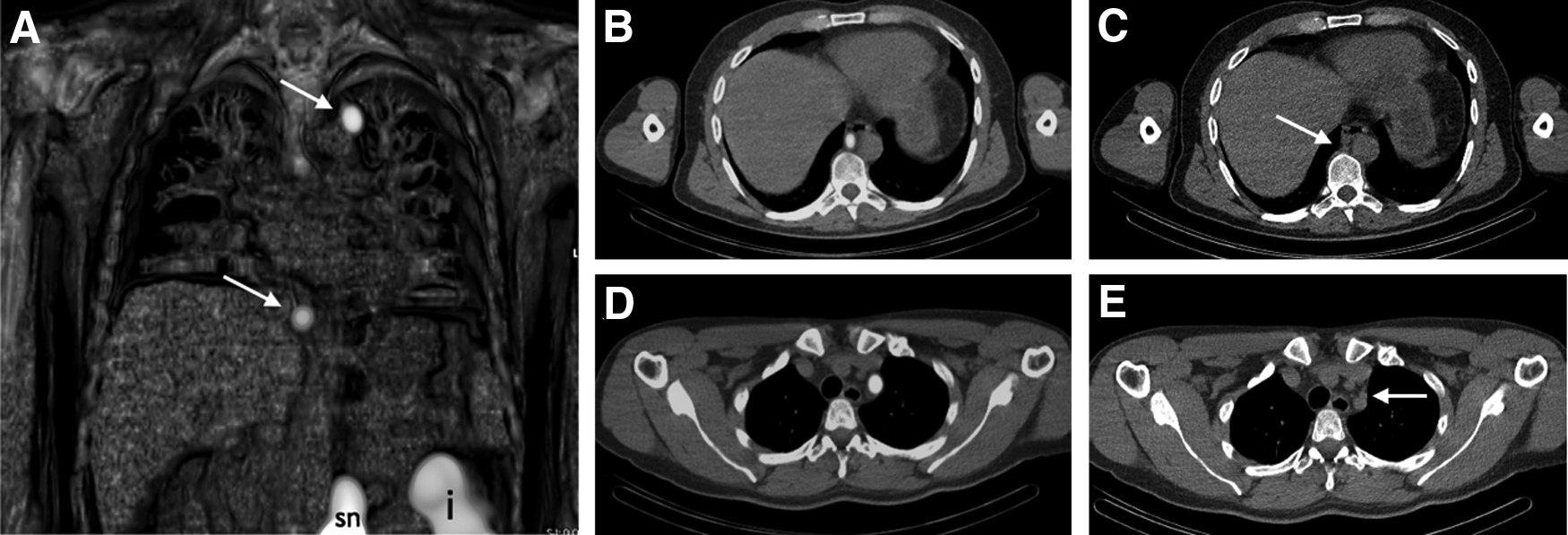
The first of these 4 cases was a 57-year-old man diagnosed with a lower pole tumor of the right kidney (diameter 6 cm). There was no evidence for distant metastases on CT imaging (cT1bN0M0). Preoperative planar lymphoscintigraphy after 2 h showed a first draining LN (Fig. 1A), corresponding with an interaortocaval SN on SPECT/CT (Fig. 1B, C), and a second LN located paracavally (Fig. 1B, D). However, lymphoscintigraphy also revealed focal uptake in the left supraclavicular area without interposition of retrocrural or mediastinal LNs (Fig. 2A). SPECT/CT enabled tracer localization alongside the subclavian vessels, with elongated accumulation in the supraclavicular area (Fig. 2E) corresponding with a dilated duct on CT (Fig. 2F). After nephrectomy, the interaortocaval and paracaval SNs were excised followed by LND in the standard template for right-sided RCC. Histopathology revealed a clear cell RCC (Fuhrmann grade III). No metastases were found in the excised LNs.

Common drainage pattern in a patient with a kidney tumor in the right lower pole.
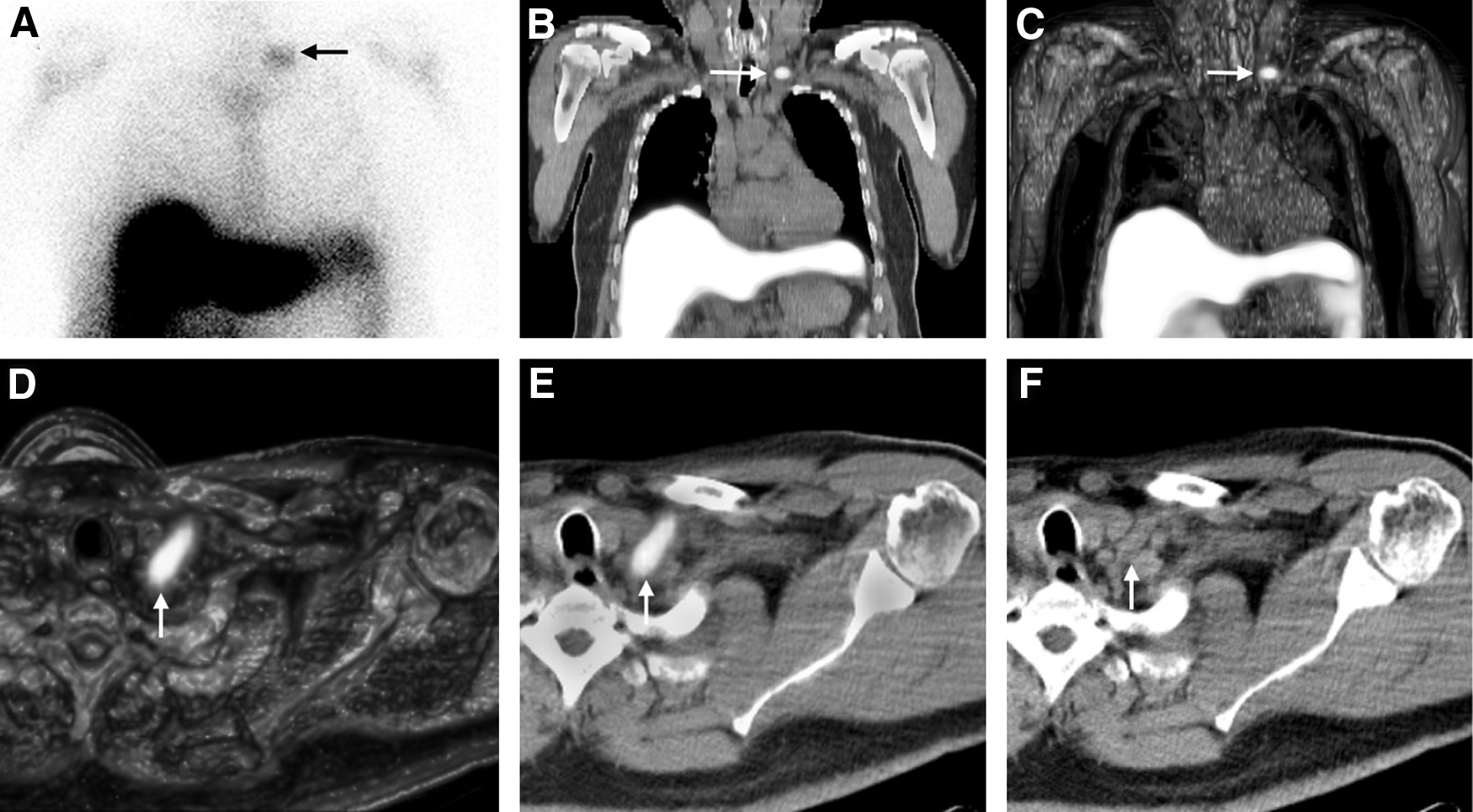
In the same patient as in Figure 1, focal tracer uptake is seen in the left supraclavicular area (arrow) as seen on the planar anterior image performed 2 hours after tracer injection
The second case was a 39-year-old man who presented with macroscopic hematuria and an upper pole mass of the left kidney. CT revealed a tumor of 5.5 cm diameter and no enlarged LNs (cT1bN0Mx). Early preoperative planar lymphoscintigraphy showed para-aortic, infradiaphragmatic, as well as mediastinal lymphatic drainage. SPECT/CT after 2 h enabled accurate anatomical localization of all radioactive nodes (Fig. 3). At laparoscopic nephrectomy, a chain of para-aortic radioactive SNs was removed, followed by left-sided standard template LND. Histopathology revealed papillary RCC type II in the primary tumor, two para-aortic SNs contained metastases of this subtype, all other excised nodes were tumor negative.
Mediastinal drainage in a patient with a kidney tumor in the left upper pole.
The third case was a 63-year-old man diagnosed with a cT1bN0M0 right upper pole tumor (6 cm diameter). Preoperative planar lymphoscintigraphy in combination with SPECT/CT showed no drainage to retroperitoneal SNs, but did reveal elongated mediastinal activity along the course of the thoracic duct (Fig. 4). Due to extreme obesity, LND was abandoned during partial nephrectomy. Histopathology revealed a clear cell RCC Fuhrman grade II.
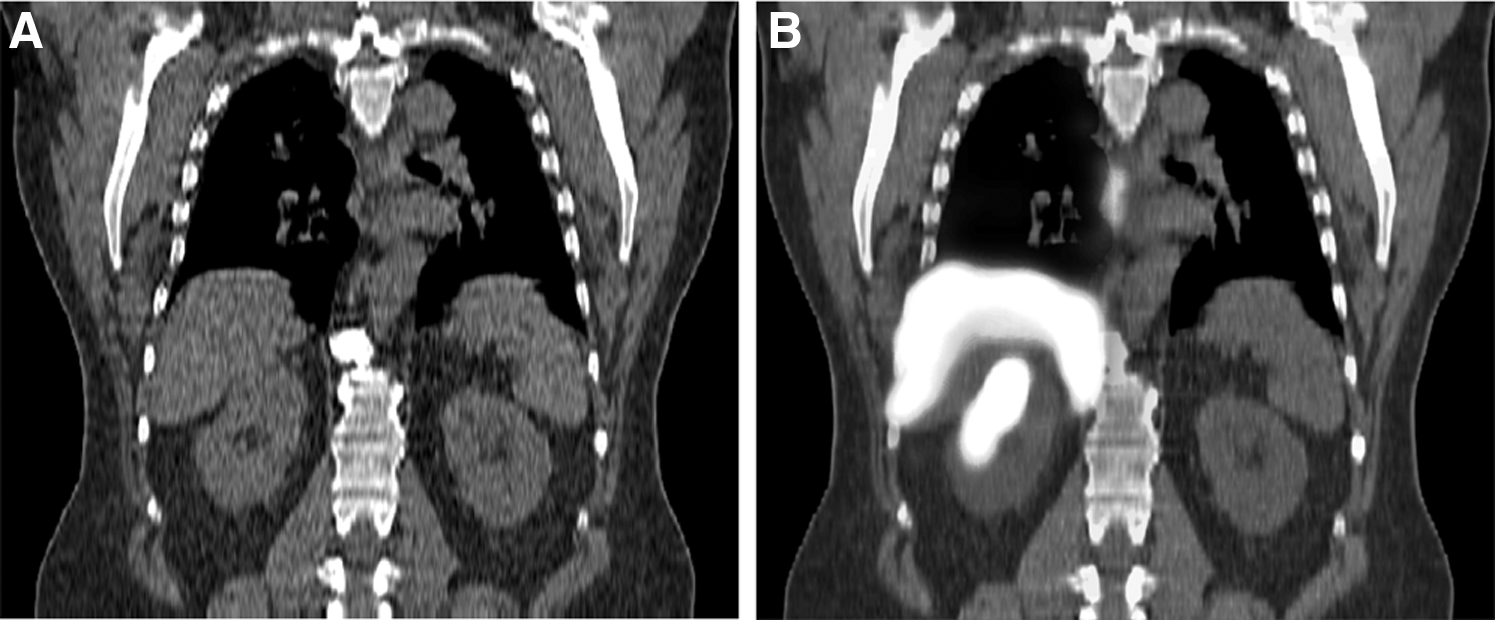
Mediastinal drainage along the course of the thoracic duct in a patient with no drainage to retroperitoneal SNs after intratumoral tracer injection in the right kidney.
In the fourth case, ultrasound revealed a lower pole tumor of the left kidney (5.4 cm diameter) and possible liver metastases in a 43-year-old woman. Subsequent biopsies and PET/CT did not confirm distant metastases (cT1bN0M0) and robot assisted laparoscopic partial nephrectomy and SN dissection were performed. Lymphoscintigraphy and SPECT/CT revealed drainage to two para-aortic SNs together with evident left supraclavicular tracer accumulation without any mediastinal or infradiaphragmatic interposition, most likely due to drainage along the thoracic duct (Fig. 5A–D). Both para-aortic SNs were excised followed by standard template LND. All harvested LNs proved tumor negative at histopathology. The primary tumor was a chromophobe RCC.

SN mapping in a patient with a tumor in the left kidney.
Discussion
Traditionally, lymphatic drainage from the kidney is considered to be directed towards the hilar region branching off into the paracaval, interaortocaval, or para-aortic retroperitoneal lymph nodes depending on the tumor side. Clinically, however, isolated mediastinal and pulmonary lymph node metastasis are more frequently observed in RCC compared to tumors in other organs.8,9 The lymphatic drainage of renal tumors may therefore not always follow the expected pattern, as has repeatedly been found for other tumor sites. 10
Renal drainage patterns were previously assessed by analyzing lymphatic metastases within lymphadenectomy specimens or on autopsy. In a cadaver study by Saitoh et al. that included over 1800 cases of renal cell carcinoma, a wide diversity in location of lymph node metastases was observed. 11 The interesting finding that ipsilateral renal hilar lymph node metastases were only found in 7%, while pulmonary lymph node metastases were found in 66.2%, retroperitoneal in 36%, para-aortic in 26.8%, and supraclavicular in 20.7%, suggests that single lymph node metastases without interposition of hilar metastases might occur. Yet, since most patients had multiple lymphatic metastases, it was not possible to pinpoint which node was involved first. Single lymph node metastases have been described by Hultén et al. in a supraclavicular lymph node in 1 patient and an iliac LN in 2 patients without any further metastasis. 12 A left supraclavicular lymph node metastasis found in another case at our institute is exemplified in Figure 5E. Furthermore, Johnsen et al. detected single lymph node metastases in 10 patients, with a single mediastinal, supraclavicular, and axillary node in respectively 8, 1, and 1 patients. 13 These lesions may chronologically be the first site of metastasis.
SN mapping using lymphoscintigraphy and SPECT/CT after intratumoral injection of a radiotracer may help to support the hypothesis that aberrant lymphatic drainage can be a cause for isolated mediastinal and supraclavicular lymph node metastases that are frequently observed in renal cell carcinoma.8,9,14–16 Clinically, a possible explanation might lie in direct drainage through the thoracic duct. In this study, we described four patients with kidney tumors scheduled for SN mapping showing supraclavicular and mediastinal drainage on preoperative lymphoscintigraphy. The anatomical information provided by fused and volume rendered SPECT/CT enabled the exact localization of the accumulated radiotracer. The mediastinal and supraclavicular lymph nodes observed in cases 1, 2, and 4 are connected with the thoracic duct, which has valves to prevent reflux and may distribute the tracer along these basins, forming indirect evidence for drainage along the thoracic duct. Moreover, in one patient (case 3), elongated mediastinal drainage was observed without any other lymph node interposition, suggesting direct drainage through the thoracic duct (Fig. 4).
Our findings are supported by a study from Assouad and Riquet et al. who injected normal kidneys of 26 cadavers with a blue modified Gerota mass and dissected lymph vessels until their termination.5,6 Renal lymphatics reached distant nodes as classicaly described (eg, retrocaval, para-aortic). More surprising, however, posterior lymphatic vessels connecting to the thoracic duct were also found in all cases, in several (38% on the right and 16% on the left), even directly without interposition of any lymph node. Such posterior renal tributaries leading directly to the thoracic duct may also explain why supraclavicular activity was observed with simultaneous activity in retroperitoneal SNs, but without any mediastinal interval nodes in case 1 and 4. In addition, the frequently observed isolated mediastinal lymph node metastases in RCC may be a consequence of this drainage pattern. As the thoracic duct drains into the subclavian vein with subsequent circulation into the lungs, it was argued that the lung may be one of the primary metastatic landing sites. 5 More intriguingly, it may explain why retrospective studies and prospective randomized trials of LND in RCC fail to demonstrate an undisputable survival benefit for dissection of clinically insuspicious retroperitoneal lymph nodes. 17 Future (cadaver) studies using lymphatic mapping techniques may help substantiate this assumption.18,19
The feasibility of lymphoscintigraphy of kidney tumors has been previously demonstrated in two pilot studies.3,4 In our previous series of SN mapping in the first 20 included kidney cancer patients, intratumoral tracer injection also led to drainage outside the locoregional retroperitoneal lymphatics in two (out of 14) patients (mammary chain, mediastinal, pleural), though there was simultaneous retroperitoneal drainage. 3 Six patients, however (30%), showed no lymphatic drainage on the preoperative images. This may be explained by lack of drainage through lymphatic vessels or loss of tracer to the bloodstream during injection. Another possible explanation might be direct drainage to the thoracic duct without any interposition of lymph nodes that was missed on the early planar images. In the study by Sherif et al. of 13 patients, the percentage of cases with no visualized lymphatic drainage was considerably lower (9%). 4 In this study however, injections were placed in the periphery of the tumor instead of intratumorally, which may lead to the depiction of lymph nodes on the preoperative images (which were all localized within the locoregional retroperitoneal templates), but may not necessarily reflect the lymphatic drainage of the tumor itself. 20 In this series, one patient had two tumor positive SNs at histopathology. The fact that all other excised lymph nodes during retroperitoneal LND were tumor negative, confirms the feasibility of SN procedure in kidney cancer patients, although more extensive research is needed to further substantiate the diagnostic and therapeutic value of renal SN biopsy. Our retrospective study is further limited by absence of histological examination of the extra-retroperitoneal nodes. The primary endpoint of the ongoing trial is analysis of potential metastatic landing sites on SPECT/CT imaging in vivo and not the clinical significance of the SN technique in renal cancer. It was therefore deemed unethical to extend harvesting of SNs into the thoracic area without further proof that SN mapping has clinical relevance in renal cancer.
Conclusion
SN mapping of renal tumors using functional imaging modalities such as lymphoscintigraphy and SPECT/CT enables identification and potentially sampling of SNs outside the area of routine dissection. Although SNs from the kidney are mainly localized in the para-aortic, paracaval, and interaortocaval region, direct aberrant drainage through the thoracic duct occurs as demonstrated in this study. This drainage pattern may be associated with the frequently observed isolated mediastinal lymph node metastases in RCC as well as the lung being the primary metastatic site. In addition, it may support a hypothesis why randomized trials of LND in RCC have not demonstrated an impact on survival.
Footnotes
Author Disclosure Statement
All authors have no conflicts of interest or financial ties to disclose.