
Abstract
Abstract
Background:
A few studies about lymphoscintigraphy in breast cancer patients have reported a correlation between decreased sentinel lymph node (LN) uptake and increased risk of axillary involvement with the hypothesis of blocked lymphatic passage of radiotracers by metastatic burden. This study is designed to investigate whether the visible internal mammary LN of lymphoscintigraphy (IM-LPS) is related to axillary LN metastasis, rather than identifying sentinel LN in the internal mammary area.
Methods:
We retrospectively reviewed medical records of 401 breast cancer patients who underwent sentinel lymphoscintigraphy using Tc-99m phytate and subsequent axillary LN dissection. The IM-LPS was divided into positive or negative groups, and axillary lymphoscintigraphy (A-LPS) was visually graded into four groups according to the method suggested by Lee et al. 1 To evaluate the relation of positive IM-LPS and A-LPS pattern with axillary LN metastasis, multivariate logistic regression analysis was done with covariates of Memorial Sloan-Kettering Cancer Center model.
Results:
Positive IM-LPS was found in 32 patients. On the univariate logistic regression analysis, positive IM-LPS (p=0.01) and A-LPS pattern (p<0.05) successfully predicted the axillary LN status. On the multivariate logistic regression model, positive IM-LPS (OR 2.6362; 95% CI 1.0382–6.6938; p=0.04) and group II A-LPS (OR 1.9773; 95% CI 1.1336–3.4491; p=0.01) remained statistically significant variables for the predictor of axillary LN metastasis.
Conclusion:
This study suggests that IM-LPS and A-LPS pattern might be useful to show the burden of axillary LN metastasis in breast cancer patients, as an indicator of altered lymphatic pathway.
Introduction
T
As a result of the ease and accuracy of detecting the sentinel node, preoperative breast lymphoscintigraphy and intraoperative gamma probe localization have become standard practice in many institutions. 4 SLNB can prevent complete axillary LN dissection in patients in whom the sentinel LN is found to be free of metastasis. 5 Intraoperative lymphatic mapping and SLNB have been rapidly and widely adopted as oncologic equivalents to elective LN dissection. 6 However, the impact of the detection of internal mammary sentinel nodes during lymphoscintigraphy is still controversial in regard to staging and managing breast cancer. Sentinel LN mapping with lymphoscintigraphy often identifies non-axillary nodes, although the ability to identify these nodes does not imply a clinical benefit for biopsy or removal.7–10
This study is designed to investigate whether the visible internal mammary LN of lymphoscintigraphy is related to the burden of axillary LN metastasis. We hypothesized that internal mammary nodal drainage on preoperative lymphoscintigraphy may identify breast cancer patients at risk for axillary LN metastasis through alternative drainage routes.
Material and Methods
Patients
From January 2010 to December 2011, 401 female patients who were given a pathologic diagnosis of breast cancer were retrospectively enrolled in the study. All the patients underwent fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (F-18 FDG PET/CT) within median 14 (1–54) days before surgery. No patient has received neo-adjuvant chemotherapy.
Lymphoscintigraphy
111–185 MBq of Tc-99m phytate (Fujifilm, Japan) in a 0.3 mL normal saline was injected intradermally in the periareolar area within the tumor-bearing breast quadrant. Static images were obtained using with a dual-headed gamma camera (Vertex Plus (V60), ADAC, Milpitas, CA) equipped with low-energy high-resolution collimators. The energy discriminator was centered on 140 keV photopeak of Tc-99m with a symmetric 20% window. Sequential static images were obtained at 5 min, 15 min, 30 min, and 45 min until the sentinel LN is identified. Two sets of static images were obtained routinely: early anterior planar view was obtained at 5 min after injection and the second one was obtained at 15 min after injection. In the case of nonvisualization of lymphatic flow at the first planar view, gentle massage was applied on the breast for approximately 5 min to improve lymphatic drainage.
SLNB and complete axillary lymph node dissection
SLNB was performed with intraoperative blue dye mapping along with intraoperative gamma probe detection. After induction of general anesthesia, 3–5 mL of indigocarmine was injected into the subareloar area immediately before making an incision. The Tc-99m phytate was injected within 6–18 hours before the surgery and a hand-held gamma-probe was used to assist in the detection of sentinel LN. An incision was placed over the greatest activity in the axilla and radioactive sentinel LNs were removed until counting rates dropped to background level. The removed sentinel LNs were sent to the pathology department and complete axillary LN dissection was performed when sentinel LN was positive for metastasis.
Data analysis and statistics
The lymphoscintigraphy was visually categorized according to the following patterns: lymphatic flow, draining LN basin, and intensity of uptake. Images were interpreted by two trained nuclear medicine physicians. The anterior image obtained 5 min and 15 min was used in the present study. First, the lymphoscintigraphy was categorized according to internal mammary sentinel LN visualization. The positive internal mammary sentinel LN lymphoscintigraphy (IM-LPS) was defined when the first draining LN basin was the internal mammary area, regardless of delayed axillary LN visualization. Otherwise, the lymphoscintigraphy was categorized as negative IM-LPS. Second, the axillary lymphoscintigraphy (A-LPS) was visually graded into four groups regardless of internal mammary sentinel node visualization, according to the method suggested by Lee et al. (Fig. 1). 1 Group I was defined when lymphoscintigraphy showed only focal sentinel LN activity at axillary area. Group II lymphoscintigraphy showed axillary sentinel LN activity with lymphatic flow activity to the axillary area. Group III showed only lymphatic channel to axillary area without definite axillary sentinel LN activity. In the case of no sentinel LN, activity was seen on lymphoscintigraphy, which was categorized as group IV.

The visual grading system of axillary lymphoscintigraphy pattern.
Chi-square test was used to compare proportions. The logistic regression was used to analyze the relationship between pathologic axillary LN metastasis and the following factors: the lymphoscintigraphy pattern, positive metastasis on F-18 FDG PET/CT, nuclear grade, tumor size, lymphovascular invasion, multifocal breast cancer, estrogen receptor (ER) status, and the number of negative sentinel LN (the number of negative sentinel LNs among dissected LNs). The tumor size and the number of negative sentinel LN were considered as continuous variables. The statistical analyses were performed using MedCalc® for windows version 12.0.4.0; p value less than 0.05 was regarded as significant.
Results
Clinical characteristics
The clinical and pathologic characteristics of the 401 patients are shown in Table 1. All patients were female and the median age was 53 years (range 29–83 years). The number of SLNB was median 3 (range 2–19) and the total number of dissected axillary LN was median 6 (range 2–38).
Others* include invasive mixed ductal and lobular carcinoma, mucinous carcinoma, tubular carcinoma, metaplastic carcinoma, adenoid cystic carcinoma, myoepithelial carcinoma, invasive tubulolobular carcinoma, intracystic papillary carcinoma, invasive apocrine carcinoma.
A-LPS, axillary-lymphoscintigraphy; DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; IM-LPS, internal mammary-lymphoscintigraphy; N, number.
Pathologic axillary LN metastasis
Focally increased F-18 FDG uptake at ipsilateral axillary LN were observed in 92 patients (22.9%) and 69 of 92 (75%) patients diagnosed as axillary LN metastasis on final pathologic exam. Among the 309 patients without F-18 FDG uptake at axillary LN, 73 patients (23.6%) diagnosed with axillary LN metastasis. Positive IM-LPS was observed 32 patients (8.0%) and 18 patients (56.3%) with positive IM-LPS showed axillary LN metastasis. Among 369 patients with negative IM-LPS, 124 patients (31.4%) showed pathologic axillary LN metastasis. The A-LPS group was observed in 150, 129, 26, and 96 patients in order. The more pathologic axillary LN metastasis was observed as the group increased: 23.3%, 45.0%, 50%, and 37.5% in each group (p=0.02) (Table 2).
A-LPS, axillary-lymphoscintigraphy; F-18 FDG PET/CT, F-18 fluorodeoxyglucose positron emission tomography/computed tomography; IM-LPS, internal mammary-lymphoscintigraphy.
Internal mammary visualization on lymphoscintigraphy
In the prediction of pathologic axillary LN metastasis, the univariate analysis was performed with the variables of IM-LPS status, A-LPS pattern, positive F-18 FDG PET/CT scan, nuclear grade, tumor size, lymphovascular invasion, multifocal breast cancer, ER status, and the number of negative sentinel LN (Table 3). The positive IM-LPS successfully predicted pathologic axillary LN metastasis (odds ratio (OR) 2.5403; 95% CI 1.2229–5.2771; p=0.01) when compared with negative IM-LPS. The A-LPS categorization was correlated with the axillary LN metastasis: group II with OR 2.6841 and p=0.0002, group III with OR 3.2857 and p=0.0065. Group IV (OR 1.9714; p=0.0176) showed relatively low OR than group II and group III. The rest of the variables, including nuclear grade, tumor size, lymphovascular invasion and multifocal breast cancer, which were already known as predictors of axillary LN metastasis, showed statistically significant result except the ER state.
A-LPS, axillary-lymphoscintigraphy; IM-LPS, internal mammary-lymphoscintigraphy; LN, lymph node; N/A, not available; OR, odds ratio.
On the multivariate analysis using the variables with p value less than 0.02 on univariate analysis, positive IM-LPS (p=0.04), group II A-LPS pattern (p=0.01), positive F-18 FDG PET/CT (p<0.0001), tumor size (p=0.04), lymphovascular invasion (p<0.0001), multifocal breast cancer (p=0.009), and ER status (p<0.0001) remained statistically significant variables. The results of group III and IV A-LPS pattern and nuclear grade were not available on multivariate analysis.
Discussion
The present study examined whether internal mammary visualization on preoperative lymphoscintigraphy with subareolar injection is associated with axillary LN metastasis in patients with breast cancer. We found that patients with internal mammary drainage have more axillary LN metastasis than those without internal mammary drainage.
A few previous studies reported a correlation between decreased LN uptake and increased risk of axillary involvement.1,11,12 A reasonable explanation for this phenomenon would be that the lymphatics become progressively infiltrated with tumor cells, blocking the passage of radiotracers. 11 This explanation was supported by a recent study conducted by Lee et al. 1 The authors used the grading system that reflects the degree of impairment of lymphatic transport. They found that, as the grade increases, the radioactivity of the upstream lymphatic vessels increases while that of the sentinel LN decreases. The major explanation of this phenomenon was that a higher grade pattern is related to a greater lymphatic tumor burden, and this may be related to an increased likelihood of nonsentinel LN metastasis. Moreover, there is a case report about nondetection of sentinel LN with lymphoscintigraphy as a result of massive malignant invasion in a LN, in a patient with malignant melanoma. 13
We used a grading system similar to that of Lee et al. 1 with the Tc-99m phytate as a radiotracer instead of Tc-99m human serum albumin. The Tc-99m phytate colloid can be formed in situ in the blood by interacting of the phytate ligand with calcium content in serum. 14 We found that the large number of patients showed axillary LN metastasis in higher grade of lymphoscintigraphy. However, in grade IV, the proportion was slightly decreased compared to that of group II and III. There may be a false negative rate secondary to shine through from injection site because we used only anterior view of image without lateral or oblique view.
This finding could be extended to the explanation of the correlation of positive IM-LPS with axillary LN metastasis. Among the patients with positive IM-LPS, 56.3% (18/32) of patients showed axillary LN metastasis, whereas 31.4% (124/369) of patients with negative IM-LPS were diagnosed with pathologic axillary LN metastasis. In general, internal mammary sentinel LN drainage is found in up to approximately 25% of patients during preoperative lymphoscintigraphy.9,15,16 The internal mammary LN is usually visualized simultaneously with axillary LN, and the incidence of isolated lymphatic drainage to internal mammary LN has been estimated to be 1%–8%.10,16–19 Comparable to previous reports, 8.0% of our patients showed internal mammary sentinel LN uptake on lymphoscintigraphy and isolated IM-LPS drainage was found in 3.24% (13/401) of patients.
The lymphatic drainage of the breast is poorly understood. Several investigators have shown discordant drainage patterns from injections of localizing agents into the subareolar plexus, subdermal breast tissue, and the deep breast parenchyma.18, 20–22 Generally it is shown that with deeper injections, a higher visualization rate of extra-axillary drainage is seen compared with superficial injections.23,24 The intraparenchymal injections consistently visualize a more diverse pattern of lymph flow. Specifically, the internal mammary chain and supraclavicular nodes are commonly seen after intraparenchymal injection, and injection in different quadrants of the breast also show different patterns of localization. 21 In the present study, Tc-99m phytate was injected in the periareolar area in all patients interadermally, therefore we suppose that there was no influence on uptake in internal mammary basin on lymphoscintigraphy according to injection site.
The uptake of internal mammary LN on lymphoscintigraphy does not represent metastasis in the internal mammary LN basin. 9 The previous study also suggested that predominant drainage to the internal mammary LN area is not associated with internal mammary LN involvement and long-term outcome, even in the theoretical overestimation of internal mammary LN containing micro or macro metastasis at the time of diagnosis. 25 In the present study, internal mammary LN metastasis was compared to F-18 FDG PET/CT results. F-18 FDG PET study is known to be effective in detecting metastasis in LN of patients with breast cancer (sensitivity 94%). 26 We observed that only 2 patients with positive IM-LPS showed internal mammary LN metastasis on F-18 FDG PET/CT. In this case, the internal mammary visualization on lymphoscintigraphy could be supposed as sentinel LN. However, there were large metastatic tumor burden in axillary basin in 2 patients (Fig. 2). This finding supports the theory of an internal mammary pathway as an altered lymphatic flow result of interrupted axillary flow due to metastastatic tumor cells.
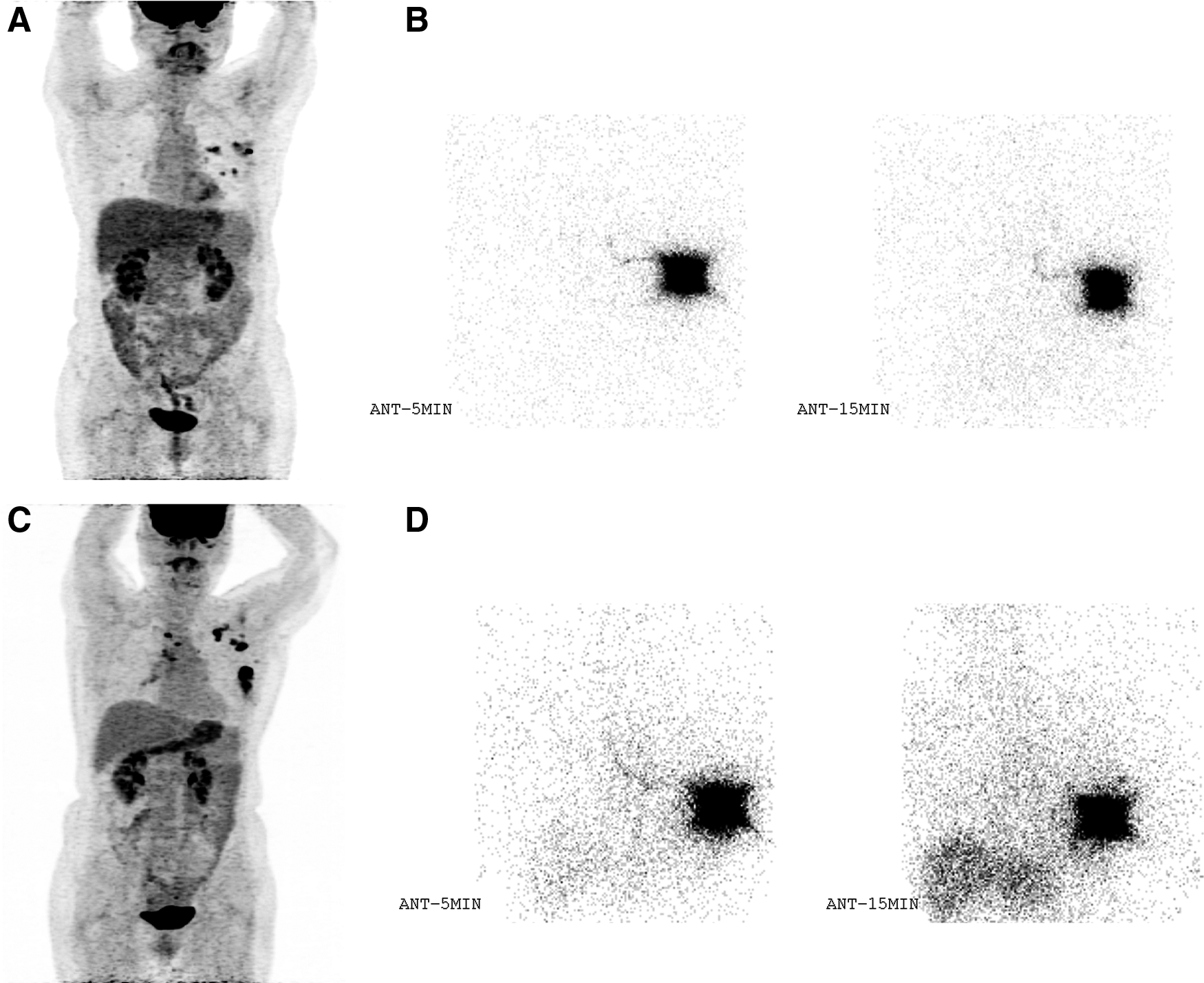
The patients with positive internal mammary lymphoscintigraphy showing large metastatic burden in ipsilateral axillary lymph node area on F-18 FDG PET/CT.
Recently, new imaging agents have been used to image the lymphatics and SLN with MRI and optical techniques, and new fluorescent nanoparticles such as upconverting nanocrystals are potential future agents. 27 Also, in addition to these imaging agents, a bimodal nanoparticle contrast agent should be attempted for visualization of SLN on breast cancer in the future. 28
Conclusion
This study suggests that IM-LPS and A-LPS patterns might be useful to show the burden of axillary LN metastasis in breast cancer patients, as an indicator of altered lymphatic pathways.
Footnotes
Acknowledgment
This work was supported by a 2-Year Research Grant of Pusan National University.
Author Disclosure Statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.