
Abstract
Abstract
Background:
Factors associated with lymphedema development after breast cancer surgery are not well established. The purpose is to assess the value of patient, disease and treatment-related factors predicting lymphedema development.
Methods and Results:
This study included 371 women with primary invasive breast cancer treated surgically between 2005 and 2009 with follow-up until December 2011. At each follow-up visit, both upper limb circumferences were measured at seven points to calculate the upper limb volume. Kaplan-Meier and Cox regression models for survival were applied. By the end of the follow-up period, 33.4% of women (n=124) had developed lymphedema. According to volume, lymphedema at diagnosis was mild in 78.5%, moderate in 19.0%, and severe in 2.5% of them. A 77.4% of lymphedema had enough clinical relevance to be treated. The probability of developing lymphedema within 12, 24, and 36 months post-surgery was 28.7% (95%CI 24.1–34.0%), 34.6% (95%CI 29.5–40.2%), and 38.3% (95%CI 32.8–44.3%), respectively. High stages, axillary lymph node dissection, chemotherapy, radiotherapy, and postoperative seroma were predictors of lymphedema in the bivariate survival analysis. Only axillary lymph node dissection and radiotherapy maintained their significance in the multivariate model. When the analysis was restricted to patients who underwent axillary lymph node dissection, the number of nodes excised did not influence the occurrence of lymphedema.
Conclusions:
Axillary lymph node dissection and radiotherapy affected lymphedema development. This study provides support that breast cancer patients with such characteristics should be closely monitored, especially during the first year after surgery.
Introduction
I
Lymphedema is a chronic condition that tends to progress and cause physical, functional, psychological, and social morbidity in breast cancer patients.2–5 The frequency of upper limb lymphedema varies according to the population studied, the definition of the outcome, assessment methods, and the follow up period. For this reason, the incidence of this condition varies from 11 to 65%.3,6–11
The factors associated with lymphedema development after breast cancer surgery are not well established. The most widely accepted is the nodal surgical approach, while there is still some controversy surrounding factors such as overweight/obesity,3,6,10–18 radiotherapy,3,6,7,9–11,13–17,19,20 and chemotherapy.3,6,9–11,16,17,19,20 In addition, few studies focus on the effect of postoperative hematoma, seroma, or infection.21,22
Numerous publications have demonstrated the importance of axillary lymph node dissection in lymphedema development (ALND).6,8,9 Moreover, some authors report that the number of excised nodes is related to the risk of developing lymphedema,3,6,11,17,19,20 but this point is still controversial.14,23 Other authors suggest that the risk of developing lymphedema after breast cancer surgery varies according to the combination of exposures to sentinel lymph node biopsy (SLNB) or ALND, chemotherapy, and radiotherapy treatments.9,16
This article aims to investigate patient, disease, and treatment-related characteristics of the development of lymphedema in a cohort of breast cancer patients admitted to an outpatient rehabilitation setting.
Patients and Method
This study was approved by the hospital Ethics Committee and was conducted in accordance with the Declaration of the World Medical Association.
This retrospective longitudinal study was carried out in a general teaching hospital primarily serving a population of more than 300,000 inhabitants. In this center, we have a multidisciplinary breast cancer unit that includes follow-up in the rehabilitation ward after ALND, and more recently (since 2007–2009) after SLNB.
Eligible patients were women diagnosed for primary breast cancer, operated on between January 2005 and December 2009, and having at least one visit in the rehabilitation setting after surgery. Patients were excluded when they had a stage IV tumor (n=6) or bilateral synchronic disease (n=17). A total of 371 patients were finally included.
All data were extracted from the hospital records by the breast cancer rehabilitation specialist and by a trainee in rehabilitation medicine, except for tumor and treatment characteristics that were obtained from the hospital-based cancer registry.
The tumor stage at diagnosis was classified according to the version of the pathological TNM classification used at the time of diagnosis. Information on biomarker expression (estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and Ki67 index) was retrieved from the clinical chart. Immunostaining for ER, PR, and HER2 was carried out as previously reported. 25 An immunohistochemical test was performed to identify cells stained for Ki67 (MIB-1 clone, Dako, Glostrup, Denmark). The positivity index (%) was determined by the number of Ki-67 positive cells among the total number of tumor cells counted. Based on the expression of these biomarkers, tumors were classified into four subtypes. Tumors expressing ER and/or PR and HER2-negative and low Ki67 index (<20%) were classified as Luminal A type. Tumors expressing ER and/or PR and HER2-negative and a high Ki67 index (≥20%) were considered as Luminal B type. Tumors that were ER-negative, PR-negative, and HER2-negative were considered triple negative type, and finally HER2-positive tumors, irrespective of the ER or PR results, were considered HER2-positive.
The post-surgical complications considered were hematoma, infection, seroma, or other wound problems. The seroma diagnostic criterion was a persistent liquid collection that required aspiration after removal of surgical drains.
Patients who attended the rehabilitation program were evaluated by the same specialist at the 1st, 6th, and 12th postoperative months and yearly thereafter. The rehabilitation controls followed a protocol and included: height and weight, symptoms referred to upper limb and surgical area, and a clinical examination specially directed to surgical scars and skin condition, upper limb neurological assessment, shoulder range of motion, and lymphedema. Lymphedema was determined by measuring the circumference of both upper limbs at seven points. Lymphedema was then diagnosed when there was a difference of 2 cm or more at any circumference point, except for the hand and chest where lymphedema was considered in the event of a thicker skin fold and congruent symptoms. The upper limb volume was calculated using the pyramid frustum formula as described by Taylor et al. 26 The excess volume was the difference between the affected and unaffected arm, expressed in mL and as a percentage of unaffected arm volume. Lymphedema was classified according to severity as mild (excess volume <20%), moderate (20% to 40%), and severe (>40%). 27 All moderate and severe lymphedema were treated with complex decongestive therapy, whereas mild lymphedema was treated whenever the symptoms were clinically relevant or when there were infectious complications.
Statistical methods
The beginning of follow-up was the date of surgery. The main outcome of interest was development of lymphedema. The end of follow-up for those who developed lymphedema was the date when the patient noticed it, or if this was not possible, the date when the doctor diagnosed the lymphedema. Patients were censored if they were lost to follow-up or died, or had not presented lymphedema at 31 December 2011. If, during follow-up, a woman was diagnosed with contralateral breast cancer (n=6), she was censored at that time.
In order to investigate the effect of the number of dissected lymph nodes in the development of lymphedema, we also performed an analysis including only cases that underwent ALND.
The baseline covariates studied were age, body mass index, tumor stage, histological grade, cancer subtype, side of treatment, type of breast cancer surgery, SLNB or ALND, post-surgical complications, chemotherapy, radiotherapy, and hormonotherapy. In order to investigate the prognostic effect of radiation dose, an analysis was added including only cases undergoing radiotherapy.
Kaplan-Meier survival curves were plotted. Hazard ratios (HR) and 95% confidence intervals (95%CI) were estimated using Cox models. All variables that reached p value <0.15 in the bivariate analysis were considered for the multivariate model. A variable had to have a p value <0.05 to remain in the model. All analyses were performed using Stata version 8.0 (Stata Corporation, College Station, TX).
Results
The patients' median age at cancer diagnosis was 59.1 years (range 28–88 years). Their median body mass index was 27.0 kg/m2 (range 13.4–48.2 kg/m2). Approximately half the women (51.2%) had stage II breast cancer at diagnosis. The great majority of patients were treated with conservative breast surgery (78.7%). 295 women underwent ALND (79.5%) and 76 patients underwent SLNB. The median number of excised nodes in the SLNB group was 2 (range, 1–7 nodes) and for those submitted to ALND the median number of lymph nodes dissected was 15 (range 1–43 nodes). Patient, tumor, and treatment characteristics are listed in Table 1.
BMI, body mass index (kg/m2); bSCF, supraclavicular fossa.
cases submitted to axillary lymph node dissection; **cases submitted to radiotherapy.
Among the 371 women included, 124 (33.4%) developed breast cancer-related lymphedema at the end of the follow-up. Ninety-six of these patients (77.4%) received lymphedema treatment. Table 2 shows lymphedema characteristics according to treatment (2 cases with thoracic lymphedema and 1 case of upper limb lymphedema with no data available are not included in the table). Among the remaining 121 cases, there were 95 mild, 23 moderate, and 3 severe cases of lymphedema.
A total of 83.4% of lymphedema appeared during the first year after surgery. The median follow-up period for those who did not present the outcome was 24.4 months (range, 0.7–75.6 months). The probability of developing lymphedema within 12, 24, and 36 months post-treatment was 28.7% (95%CI 24.1–34.0%), 34.6% (95%CI 29.5–40.2%), and 38.3% (95%CI 32.8–44.3%), respectively (Fig. 1).
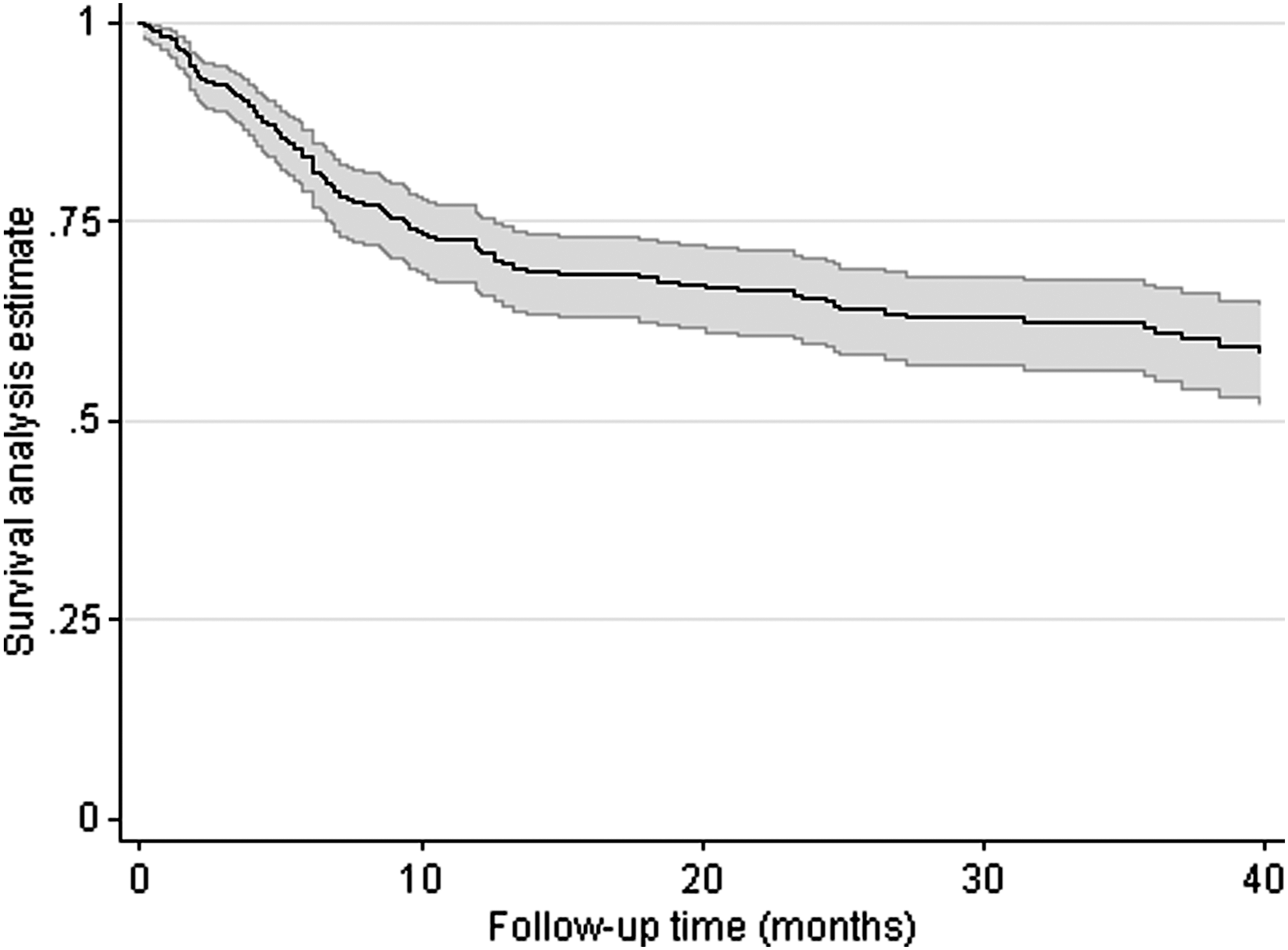
Kaplan-Meier estimated probability of detecting lymphedema following breast cancer surgery.
The bivariate Cox analysis is shown in Table 1. Patients with breast cancer in higher stages, those who underwent ALND, chemotherapy, radiotherapy, and presence of seroma after surgery, presented an increased risk of developing lymphedema. Age at diagnosis of breast cancer, baseline body mass index, histopathological grading, breast cancer subtype, surgery on the dominant side, type of breast surgery, and dose of radiation therapy did not affect lymphedema development. Surgical complications such as hematoma, infections, and other complications also did not affect the occurrence of lymphedema.
Table 3 shows the results for multivariate analysis. Only ALND and radiotherapy maintained their significance in the Cox model. Patients who underwent ALND presented an increased risk of developing lymphedema (HR=13.53, 95%CI 4.30–42.45) compared to those without ALND. A higher risk of developing lymphedema was also observed for patients who received radiotherapy, irrespective of its location.
SCF, supraclavicular fossa.
The results were very similar when survival analysis was performed using lymphedema needing treatment as the outcome (data not shown). The number of excised nodes did not affect the excess lymphedema volume (p value=0.401, Fisher's exact test).
Among patients with ALND, 41.0% developed lymphedema, whereas for SLNB there were only 4.0% (3 patients). Among the SLNB patients who developed lymphedema, all 3 cases were mild. The patients' body mass indexes were 26.89, 34.13, and 34.34 kg/m2, respectively, and none of them had post-surgical complications. Two were treated with breast conserving surgery and breast radiotherapy and the third one was treated by mastectomy and did not receive radiotherapy.
Discussion
In this study 124 women developed lymphedema at the end of the follow-up (33.4%). The predictors of breast cancer-related lymphedema were ALND and radiotherapy. In most cases (83.4%), lymphedema appeared in the first year after surgery. Most of the lymphedema diagnosed (77.4%) had enough clinical relevance to be treated.
The frequency of lymphedema registered in this study (33.4%) was similar to that reported previously. In a systematic review performed by Lee et al., 7 the frequency of lymphedema ranged from 0 to 34% when arm lymphedema was defined as a difference between upper limbs of ≥2 cm in circumference at any reference point. In a more recent study, Norman et al. 8 observed that the 5-year cumulative incidence of lymphedema was 42%.
In regard to the axillary procedure, only 3 cases of lymphedema were observed in the SLNB group (3.95%), and 121 in the ALND group (41.0%). These results are in line with those reported by Wernicke et al. 28 with 4.6% for SLNB and 34.8% for ALND, and those described by Goldberg et al. 14 with 5% lymphedema after SLNB, although their follow-ups were longer. However, Gartner et al. 9 reported a higher incidence of lymphedema for SLNB patients at 26 months after surgery (13% had lymphedema after SLNB and 36% after ALND).
Among the studies reviewed, there was a tendency to report a higher incidence of lymphedema when the studies were questionnaire-based3,9,12,16 than when they were performed by clinical measurements.6,10,13–15,19,20,29,30 In this case, although we measured perimeters, our estimates were closer to the studies performed by self-reported information. This difference may have been due to the diagnostic criteria we applied that included lymphedema in hand, wrist, and chest wall. The diagnostic criteria for lymphedema based on a difference 2 cm or more in a perimeter measure, is one of the most widely accepted and used because it is easy to obtain in clinical settings and is reliable. However, this criterion enabled distal lymphedema, which affects the hand and wrist, to be underdiagnosed because, in this area, differences of less than 2 cm could correspond to clinical relevant lymphedema. At the other extreme, differences of 2 cm above the elbow are not always lymphedema and, if so, very often do not have clinical relevance. Finally, chest wall lymphedema could not be measured by perimeter comparison.
Most of the lymphedema detected were on the upper limb of the affected side. In three cases there was lymphedema in the chest area. One of them affecting the upper limb and chest area, while the other two lymphedemas only affected the chest area. All three cases received ALND and radiotherapy, 2 involved mastectomy, and 1 was breast conserving.
Regarding excess volume, it is interesting to note that 21.5% of cases with lymphedema were either mild to severe at diagnosis. The mean excess volume for the whole sample was 277.78 mL (SD 226.52 mL), which means 13.05% (SD10.10 mL). Few authors gave information about lymphedema measurements. Among them, Helyer et al. 10 reported a mean change of 286 mL at 20 months of follow-up, which is very close to our results. Herd-Smith et al. 20 observed a mean measured perimeter excess of 23.7% in patients with lymphedema.
The predictor factors associated with lymphedema in the multivariate analysis were ALND and radiotherapy. We obtained a HR of 13.83 (95%CI 4.30–44.47) for ALND patients to develop lymphedema compared to SLNB. In a systematic review, Lee et al. 7 reported that the prevalence of lymphedema was lower in patients treated with SLNB than ALND. Our results are in accordance with this, and other recent studies.6,9,16 However, other authors reported no association between lymphedema and the axillary surgical approach.3,10,11,15
On the other hand, in this study the number of dissected nodes did not show any significant association with lymphedema. To date there is still a controversy over whether the number of lymph nodes removed is or not an independent predictor for lymphedema, while some authors reported significant association,3,6,11,17,19,20 others did not find any effect.10,13,14 Goldberg et al. 14 suggested that lymphedema could be more closely associated with the global disruption of the lymphatic channels, rather than with the number of nodes dissected.
Radiotherapy was the other predictor factor for lymphedema identified in this study. The effect of radiotherapy on lymphedema development is not consistent. While various authors observed a significant effect,7,9,15,20 others found no association.3,6,10,11,13,14,16,17 In their review, Lee et al. 7 concentrated on the influence of radiotherapy and reported that patients treated with radiation had an Odds Ratio of 1.46 (95%CI 1.16–1.84) compared to those not treated with radiation. In our study, patients who underwent radiotherapy showed a HR of more than 3 compared to those not radiated. When the different radiated areas were analyzed, the results were very similar. No significant differences were observed for radiotherapy doses.
We did not find prognostic effect of other analyzed variables. We could not explain why BMI did not achieve significance in the present study. We considered baseline the best time point to compare BMI patients with and without lymphedema, because BMI was recorded at the same time point for both groups. However, the time point when lymphedema was diagnosed was different for every patient, and it would not have had an equivalent time point to compare to the group without lymphedema. Petrek et al. 12 followed a cohort for 20 years and found that weight gain since surgery was a predictive factor for lymphedema, and that current body weight strongly correlated with weight at cancer diagnosis. Ridner et al. 18 stated the value of baseline BMI as independent risk factor for lymphedema; they found that breast cancer survivors whose BMI was ≥30 at the time of breast cancer treatment were approximately 3.6 times more likely to develop lymphedema than those with a BMI<30. In our study, we used an equivalent BMI classification; however it should be taken into consideration that our patients had lower median baseline BMI than those of Ridner et al. 18 study (27.0 vs. 28.8 kg/m2).
In an attempt to jointly assess the severity of lymphedema by objective measures as well as by the symptoms it causes, patients were classified into those who needed treatment and those who did not. However, the survival analysis did not differ substantially from the results obtained with all lymphedema patients.
This study has limitations. It was not possible to include all women who underwent surgery in our center. A comparison of both groups showed that those included in this study were younger (58.97 vs.62.02 years, p=0.001), presented tumors in a more advanced stage, and a larger proportion of them underwent mastectomy, ALND, chemotherapy, and radiotherapy (data not shown). In an attempt to exclude selection bias, we analyzed only those cases that underwent ALND as almost all of these cases are referred to rehabilitation. Radiotherapy continued to be significant and no other factor was identified.
To our knowledge, this is the first study that investigates factors associated with the development of lymphedema in our setting. The lymphedema was assessed by specialists using objective measurement methods and graded according to severity and need for treatment.
Both ALND and radiotherapy increased the risk of lymphedema in breast cancer patients, which should be taken in consideration. These patients should know they have an increased risk of lymphedema and should be instructed about lifelong measures to avoid it. Certified lymphedema specialists must systematically follow-up these patients, at least in the first year, in order to detect and treat lymphedema as soon as possible.
The fact that lymphedema appeared during the first year in 83.4% of cases, and the fact that 77.4% of lymphedema needed to be treated, underlines the importance of systematic monitoring of these patients.
Conclusions
In conclusion, most lymphedema developed during the first year after surgery. Only ALND and radiotherapy were associated with the development of lymphedema. Identification of these factors could help understand and plan the prevention and control of lymphedema in breast cancer survivors.
Footnotes
Acknowledgments
The authors wish to thank Dr. Josep Corominas, who helped us with the subtype classification of breast tumors; and Dr. Javier Sanz, who helped with radiotherapy information.
Author Disclosure Statement
No competing financial interests exist.