
Abstract
Abstract
Purpose:
To determine the radiologic manifestations of senile lymph nodes in the popliteal fossa for radiologic and clinical application.
Methods:
A total of six lower extremities from four unembalmed human cadavers were studied. Under a surgical microscope, 6% hydrogen peroxide was used to detect the lymphatic vessels commencing from the foot and leg. A 30-gauge needle was inserted into the vessels and injected with a radio-opaque lead oxide mixture. The specimens were radiographed and photographed to demonstrate the lymph nodes in the popliteal fossa. The final results were transferred to the computer for image analysis.
Results:
An average of two lymph nodes (range 1 to 3) were found in the popliteal fossa of the lower extremity. They were divided into superficial and deep popliteal groups. The superficial group was located in the superficial layer of the popliteal fossa around the small saphenous vein (SSV). The deep group was close to the popliteal surface of the femur and always located next to the popliteal vein. All lymph nodes were transparent in appearance and contained coiled lymphatic tubules. The size and density of the tubules varied.
Conclusion:
The radiologic manifestations of senile lymph nodes in the popliteal fossa have been presented and discussed to upgrade our radiologic and anatomical knowledge. This will be of benefit for radiologic and clinical applications.
Introduction
A
Recently, a new radiographic injection technique was developed to re-evaluate the human lymphatic system. 5 The transparent (inactive and/or degenerated) lymph node has been reported using this technique. 6 Anatomical and histopathologic images of lymph nodes in different degenerative stages in the head and neck region have been demonstrated and discussed. 7
In this study, a set of transparent lymph nodes in the popliteal fossa are described and demonstrated by radiographs and photographs. This will add to our clinical and scientific understanding of the stages of lymph node involution.
Materials and Methods
The investigation was performed with appropriate institutional ethics approval. Six lower limbs were disarticulated at the hip joint from four unembalmed human cadavers, two male and two female, aged between 83 to 87 (average 85 years old).
The investigation commenced at the skin area between the lateral malleolus and the Achilles tendon in three unembalmed lower limbs; and at the midpoint of the posterior leg in the remaining three unembalmed lower limbs. 0.5 mL of a mixture of 6% hydrogen peroxide (Orion Laboratories Pty Ltd, WA, Australia) was injected into the dermis and subcutaneous tissue in these areas. The epidermis and dermis were incised carefully and gently under a surgical microscope (Leica M651, Leica Microsystems Ltd, Heerbrugg, Switerland). The distended lymphatic vessel was identified in the subcutaneous tissue of the lateral heel and at the side(s) of the small saphenous vein (SSV). A 30-gauge needle (Precision glide needle: Becton Dickinson & Co, Franklin Lakes, N.J., USA) was then inserted into the vessel and the vessel was injected with a radio-opaque lead oxide mixture (Lead oxide AJAX Chemicals, NSW, Australia and milk powder: Heinz Ltd, Qingdao, China). The specimen was photographed and radiographed (Fuji FCR IP Cassette, and Fuji Computed Radiography Processor, Fuji Film Corporation, Tokyo, Japan) to locate the lymph nodes in the popliteal fossa. The final results were transferred to computer (Dell Vostro 200: Dell Computer Inc. Chinese Division, P.R. China) for image analysis using the DICOM viewer (OsiriX Imaging Software, osirux@orisix-viewer.com) and Photoshop (Photoshop CS5 Vision 12, Apple Computer Inc, USA;).
Results
An average of two lymph nodes (range 1 to 3) were found in the popliteal fossa of the lower extremity. They were divided into superficial and deep popliteal groups and had a bean shape with a mean width of 7.5 mm (range 4–14 mm) and mean length of 13.4 mm (range 8–22.5 mm) (Fig. 1 and Table 1).
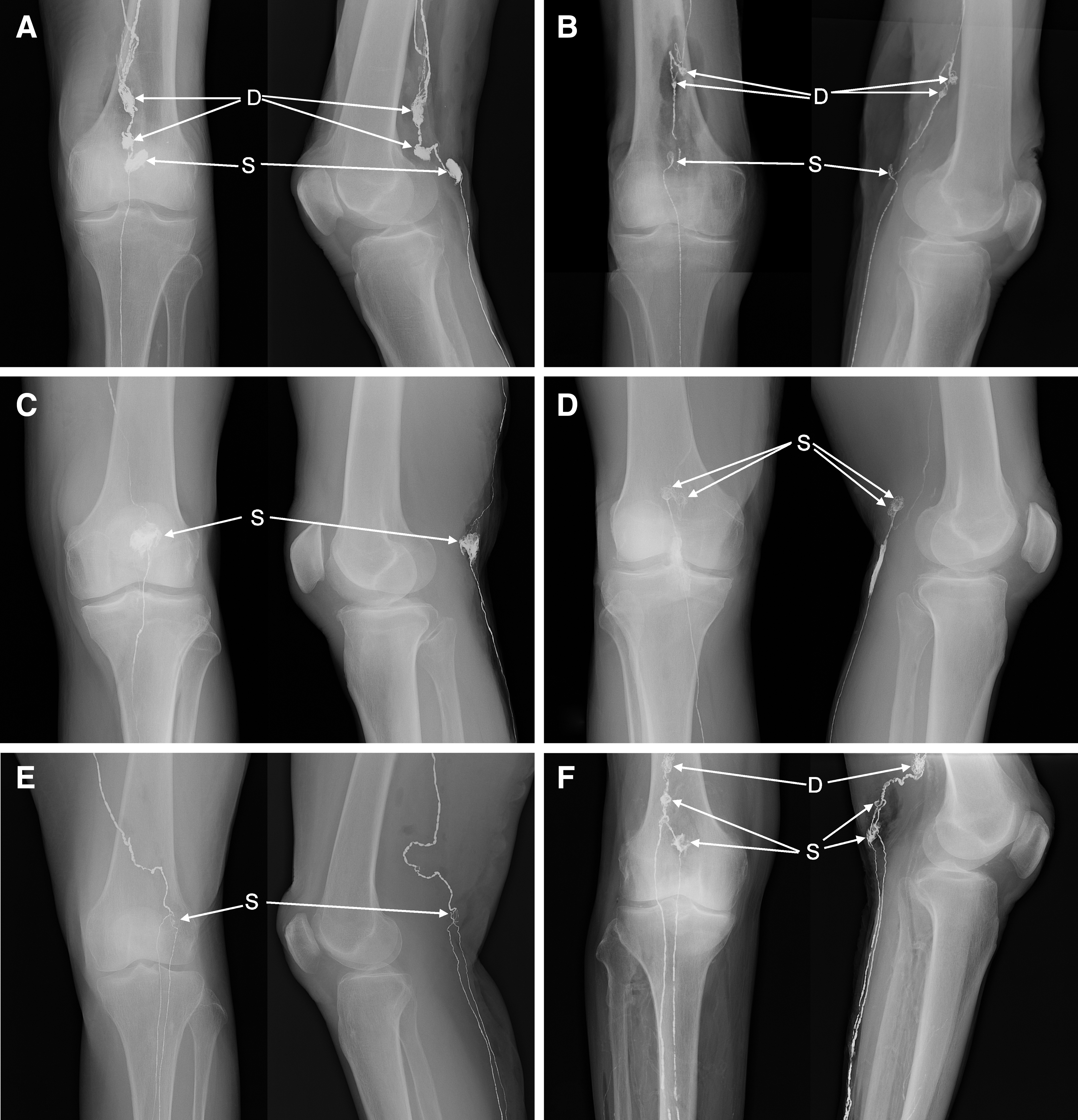
The radiologic manifestations of the popliteal lymph nodes and lymphatic vessels after lead oxide mixture injection. D, deep popliteal lymph nodes; S, superficial popliteal lymph nodes.
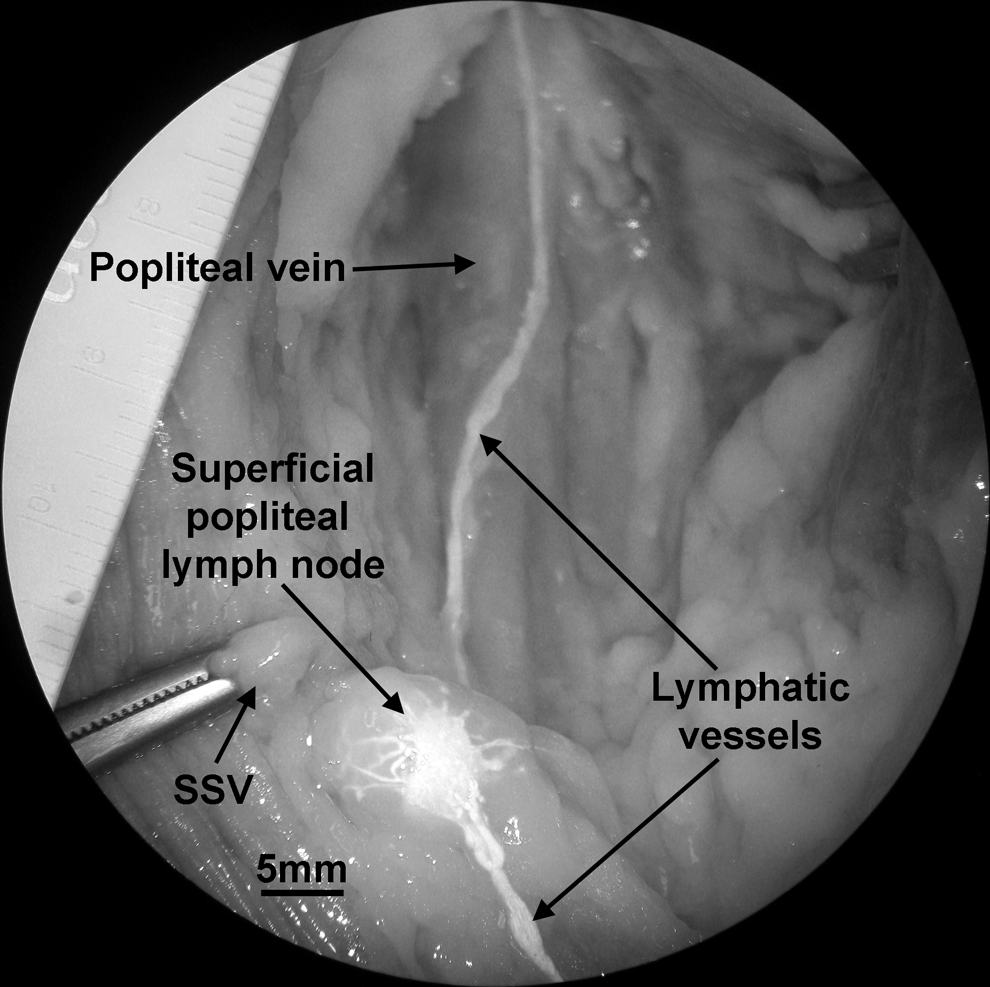
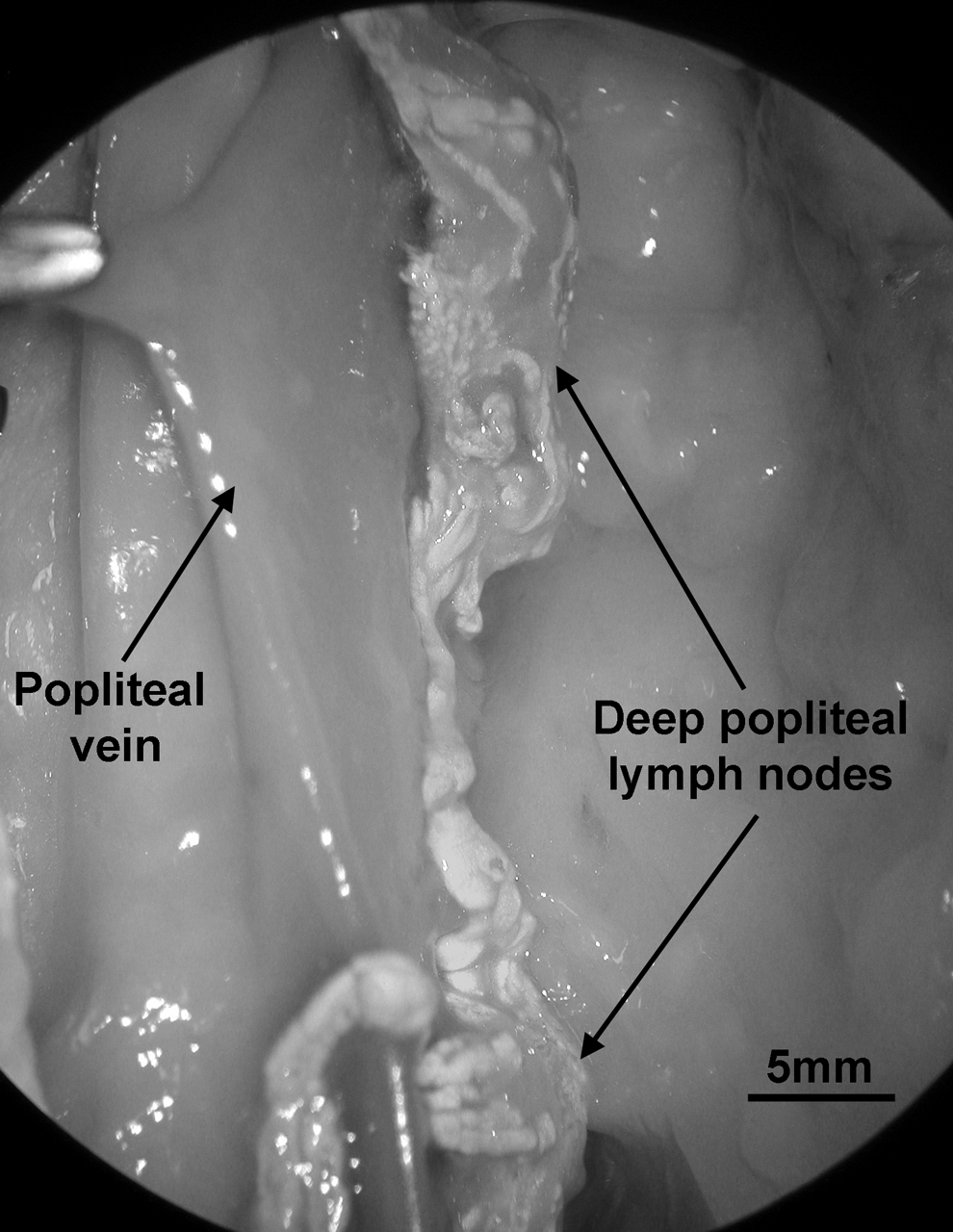
Three specimens contained both superficial and deep groups of nodes. The afferent lymphatic vessels from the leg drained into the superficial popliteal lymph nodes, then through the internodal vessels to reach the deep popliteal nodes and exit these by efferent vessels (Fig. 1A, B, and F). The other three specimens only contained the superficial group with the afferent and efferent vessels (Fig. 1C, D, and E). The superficial group was located in the superficial layer of the popliteal fossa (on lateral views in Fig. 1) around the SSV (Fig. 2). The deep group was close to the popliteal surface of the femur (on lateral views in Fig. 1A, B, and F) and always located next to the popliteal vein (Fig. 3).
The superficial popliteal lymph node (corresponding to the node in Fig. 1D) filled with lead oxide mixture showing its structure.
The deep popliteal lymph nodes (corresponding to the nodes in Fig. 1A) filled with lead oxide mixture showing their structure.
All lymph nodes had a transparent appearance and contained coiled lymphatic tubules that filled with the lead oxide mixture. The size and density of the tubules varied (Figs. 2, 3, and 4).
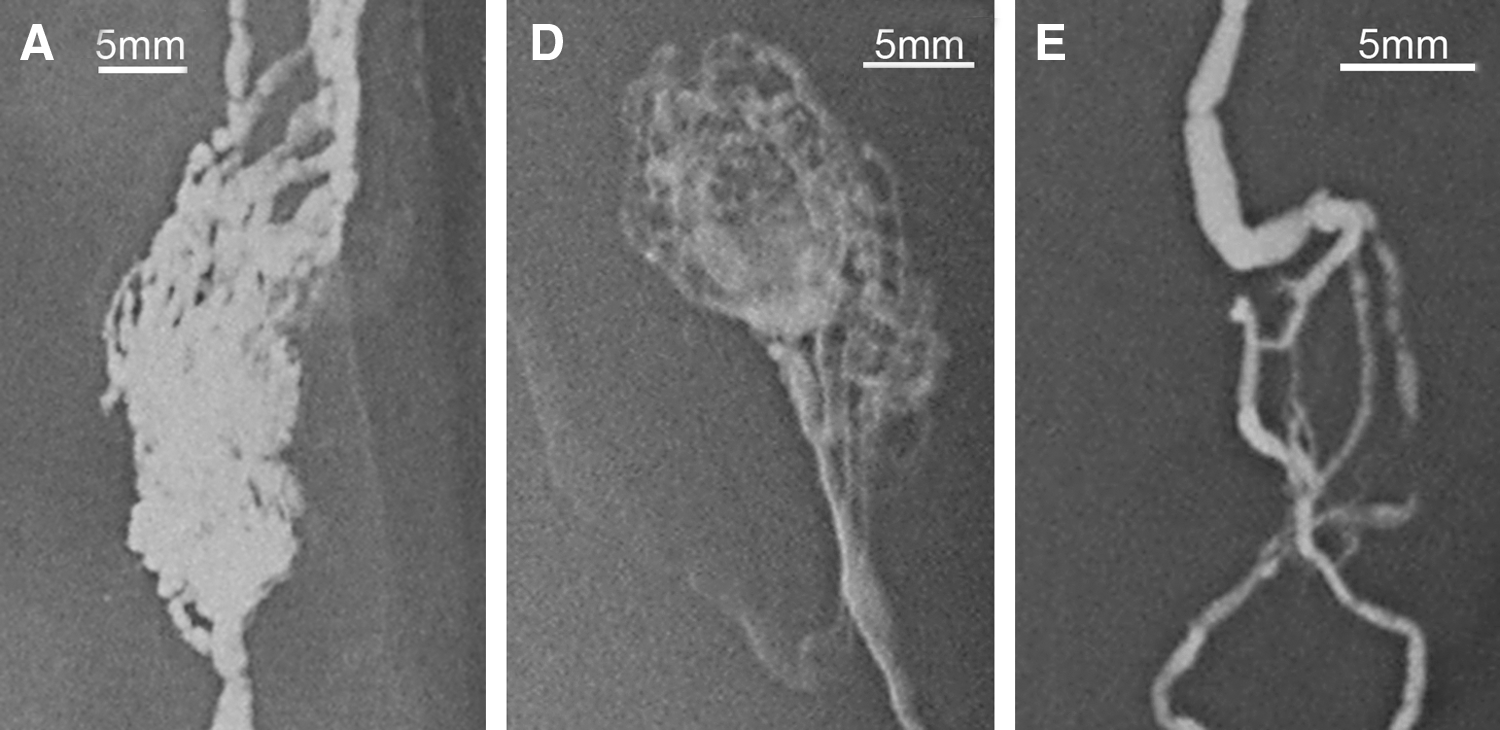
Magnified images captured from Figure 1A, D, and E show the radiologic appearance of the popliteal lymph nodes and lymphatic vessels after lead oxide mixture injection.
Discussion
Lymph nodes have been widely studied in the basic and clinical sciences. Details of morphology, function, histology, pathology, and development of lymph nodes have been presented and discussed.1–4,6–17
Previous studies have shown that lymph nodes start developing in early embryos and are fully developed in the neck, axilla, groin, and the root of the mesentery in fetal life.18–21 Denz (1947), 4 after studying over 300 human lymph nodes, concluded that lymph nodes reached their maximal development in childhood and decreased in size after puberty. The cortical tissue decreased gradually and was confined to islands surrounded by medullary tissue in old age. In some lymph nodes there was a gradual return to the fetal type in extreme old age. Similarly, Young et al. (2000) 3 described that the degenerated lymph node could reach as small as one millimetre in size. It has been reported that senile involution predominately affected the medulla, while the cortex remained unaffected. 1 However, the study might focus on solidified lymph nodes only. In 2008, Pan et al. 6 reported and presented for the first time the transparent (inactive) lymph nodes in the head and neck region. In their subsequent study, 7 lymph nodes were classified as solidified or transparent according to their appearance; active or inactive (degenerated) according to their histopathology; and generating or degenerating lymph nodes according to their stage in the development cycle. Furthermore, it was pointed out that the degenerating process is progressive from solidified to transparent nodes. Senile involution affects all elements of the lymph node including the cortex and medulla. The medulla was affected at the early degenerative stage. The lymph node became gradually transparent as the amount of lymphoid tissue decreased. Degeneration continued until the transparent lymph node became an inactive lymph node without any lymphoid tissue. The amount of cortex and medulla gradually decreased until the lymphoid tissue of the node was totally absent in the late stage of the degenerating process.
Since Kinmonth (1952) 22 first established a technique to record human lymphatic vessels radiologically, human lymph nodes have been recorded on radiographs.14,23 The radiologic appearance of lymph nodes has been described mostly according to their morphology and anatomic distribution in previous reports. In Viamonte's book (1980), 14 a series of lymphangiographic results were presented and described but details of the structure of lymph nodes were not mentioned.
The results from this study have presented and discussed the number, size, appearance, and distribution of popliteal lymph nodes in the elderly using lymphangiography and photography. The detailed radiological appearance of senile human lymph nodes has been shown.
Animal models of the transplantation of lymph nodes have been established in the last century.24–26 Based on results from these experiments, preliminary trials of lymph node transplantation have been attempted clinically for treating lymphedema of the upper extremities.27,28 Procedures have included a vascularized groin free flap containing superficial inguinal lymph nodes that was harvested from the inguinal region and transferred to a recipient site (axillary, elbow, or wrist) on the affected limb for restoring lymphatic drainage function. This study may provide an alternative donor site for lymph node harvest if other sites are unavailable in lymphedema patients.27,28 As superficial and deep popliteal lymph nodes are usually impalpable clinically,1,15 radiological techniques including lymphoscintigraphy,2,8 computed tomography lymphangiography (CTL), 29 and magnetic resonance lymphangiography (MRL) 30 may provide a valuable means of assessing lymph node availability, anatomy, and function, quantitatively and qualitatively. Injection of radioactive or contrast agents in the region between the lateral malleolus and the lateral edge of the Achilles tendon, as described in the Methods section and previously, will effectively outline the superficial and deep popliteal lymph nodes. 31 Clinicians may then assess the suitability of the popliteal fossa as a lymph node donor site. Furthermore, large afferent and efferent lymphatic vessels associated with the superficial popliteal lymph nodes have been demonstrated (Figs. 1, 4) 30 that may assist in lymphatic flap design.
Summary
The radiologic manifestations of senile lymph nodes in the popliteal fossa have been presented and discussed to upgrade our radiologic and anatomic knowledge. This will be of benefit for radiologic and clinical applications.
Footnotes
Acknowledgments
Many thanks to Professor G. Ian Taylor for his invaluable support. Many thanks to the National Health and Medical Research Foundation for funding this research, the Royal Melbourne Hospital, the Department of Anatomy at the Xuzhou Medical College in China, and the Department of Anatomy and Cell Biology at the University of Melbourne for their support.
Author Disclosure Statement
No competing financial interests exist.