
Abstract
Abstract
Purpose:
To determine routes of lymphatic drainage from the heel to the inguinal lymph nodes to assist in the clinical management of lower limb lymphatic disorders.
Methods:
Six lower limbs from three unembalmed human cadavers were studied. Under a surgical microscope, 6% hydrogen peroxide was used to detect lymphatic vessels on the medial and lateral sides of the heel. The lymphatic vessel on either side was then injected with a radio-opaque mixture. The lymphatic vessels were traced, photographed, and radiographed to demonstrate the lymphatic pathways from the heel to the inguinal lymph nodes. The final results were transferred to computer for digital image analysis.
Results:
Two groups of lymph collecting vessels were identified. The medial group, arising from the skin between the medial malleolus and the Achilles tendon, coursed along the medial side of the leg and thigh to the inguinal lymph nodes. The lateral group, arising from the skin between the lateral malleolus and the Achilles tendon, coursed along the postero-lateral side of the leg to the popliteal fossa. Alternative routes were then identified from the popliteal fossa to the inguinal lymph nodes. The number, size, type, and distribution of lymph vessels and nodes were variable from person to person.
Conclusion:
Two different lymphatic routes from the heel to the inguinal lymph nodes have been described. This information upgrades current anatomical knowledge and the results will be of benefit for the clinical management of lower limb trauma and malignancy.
Introduction
T
This study has revealed novel details of various routes of lymphatic drainage from the heel to the inguinal lymph nodes.
Materials and Methods
The study was performed with appropriate institutional ethics approval (approved by the Ethics Committees of Xuzhou Medical College, Xuzhou, China. Program No: xzmc 20130015). Six lower limbs were studied from three unembalmed human cadavers, two male and one female, aged between 72 to 85 (average 77.67 years old). Four lower limbs were harvested by dividing the pubic symphysis and the sacroiliac joints of two cadavers. Two lower limbs were disarticulated at the level of the hip joint from one further cadaver.
Lymphatic mapping commenced at the level of the ankle, between the medial or lateral malleolus and the Achilles tendon. 0.5 mL of 6% hydrogen peroxide (Zhonglian Chemical Co., Ltd, Suzhou, China) was injected into intra- and subdermal layers. Under a surgical operating microscope (Leica M651, Leica Microsytem AG, Heerbrugg, Schweiz), a small skin incision was made and the inflated lymphatic vessel was identified in the subcutaneous tissue. A 30-gauge needle (Zhejiang KDL Medical Equipment Group Ltd., Wenzhou, China) was inserted into the vessel, which was then injected with a radio-opaque barium sulfate mixture (barium sulfate: Shanghai Silian Indusry Co., Ltd. China). The specimen was subsequently radiographed (Fuji FCR IP Cassette: Fiji Film Corporation, Tokyo, Japan; Fuji Computed Radiography Processor: Fuji Film Corporation) to locate the proximal extent of the injected material, at which level further cannulation and injection were performed as described above.
Lymphatic vessels were thus traced, photographed, and radiographed to demonstrate lymphatic routes between the heel and the inguinal lymph nodes. In five specimens, the skin of the lower limb was removed via lateral vertical incision and radiographed after injection had been performed. In one specimen, transverse cross sections measuring 2 inches in thickness were created and radiographed at the levels of the ankle, the mid-leg, the knee, and the thigh after injection. Final images were transferred to computer for digital image analysis. (Dell Vostro 200: Dell Computer Inc. Chinese Division, P.R. China) and analyzed using imaging software (DICOM viewer: OsiriX Imaging Software, osirux@orisix-viewer.com) and Adobe Photoshop (Adobe Photoshop CS5, Adobe Systems Software Co., Ltd, Beijing, China).
Results
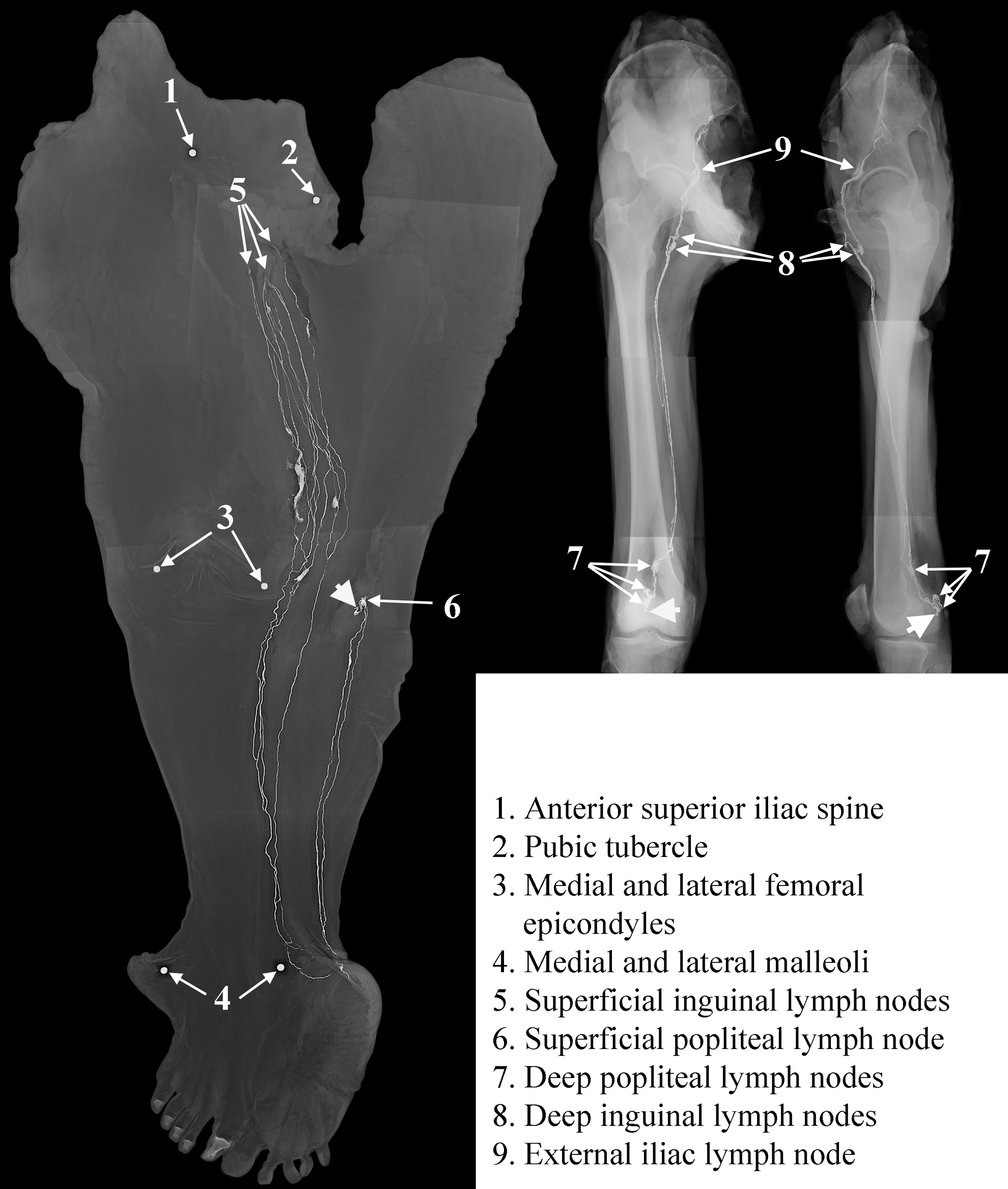
Two different lymphatic drainage routes were identified from their origin at the ankle to the inguinal lymph nodes in the groin. Drainage patterns varied in individual specimens and even between both sides of the same body (Fig. 1).

Radiographs after barium sulfate mixture injection demonstrate lymphatics coursing from the heel to the inguinal region of the lower limbs. The two central radiographs are antero-posterior projections and the two peripheral radiographs are lateral projections.
Antero-medial group of lymphatic vessels
Lymphatics originated from the medial injection point in the skin of the fossa situated between the medial malleolus and the Achilles' tendon. They formed multiple lymphatic collecting vessels traveling with the great saphenous vein (GSV) and its tributaries in the subcutaneous tissue of the antero-medial aspect of the lower limb (Figs. 1 to 5). During their course, lymphatic vessels branched, diverged, or converged, anastomosed with, or crossed over neighboring vessels. In the groin, vessels divided into multiple small branches before entering the superficial inguinal lymph nodes (Fig. 6). In one specimen, a vessel pierced the deep fascia near the groin to reach the external iliac lymph nodes (Fig. 3).
Radiographs after injection of barium sulfate mixture demonstrate lymphatics coursing from the heel to the inguinal region of the lower limbs. The left radiograph displays flattened skin of the lower limb. The central radiograph demonstrates an antero-posterior projection, and the right radiograph demonstrates a lateral projection of deeper tissues of the lower limb. Large arrowheads indicate cut ends of lymphatic vessels.
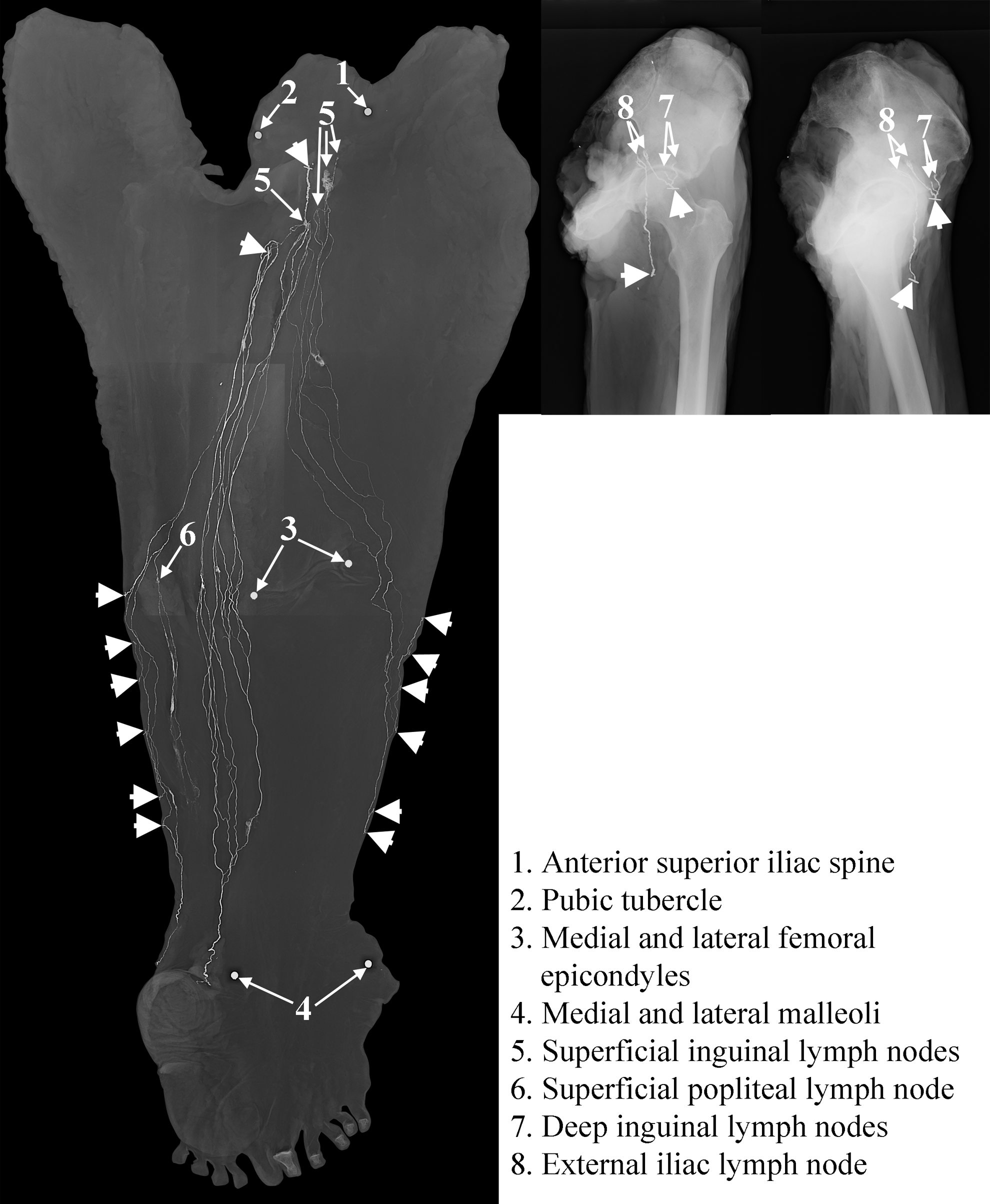
Radiographs after injection of barium sulfate mixture demonstrate lymphatics coursing from the heel to the inguinal region of the lower limbs. (Left) The flattened skin of the lower limb; (Central) antero-posterior projection; (Right) lateral projection of deeper tissues of the thigh. Large arrowheads indicate cut ends of lymphatic vessels.
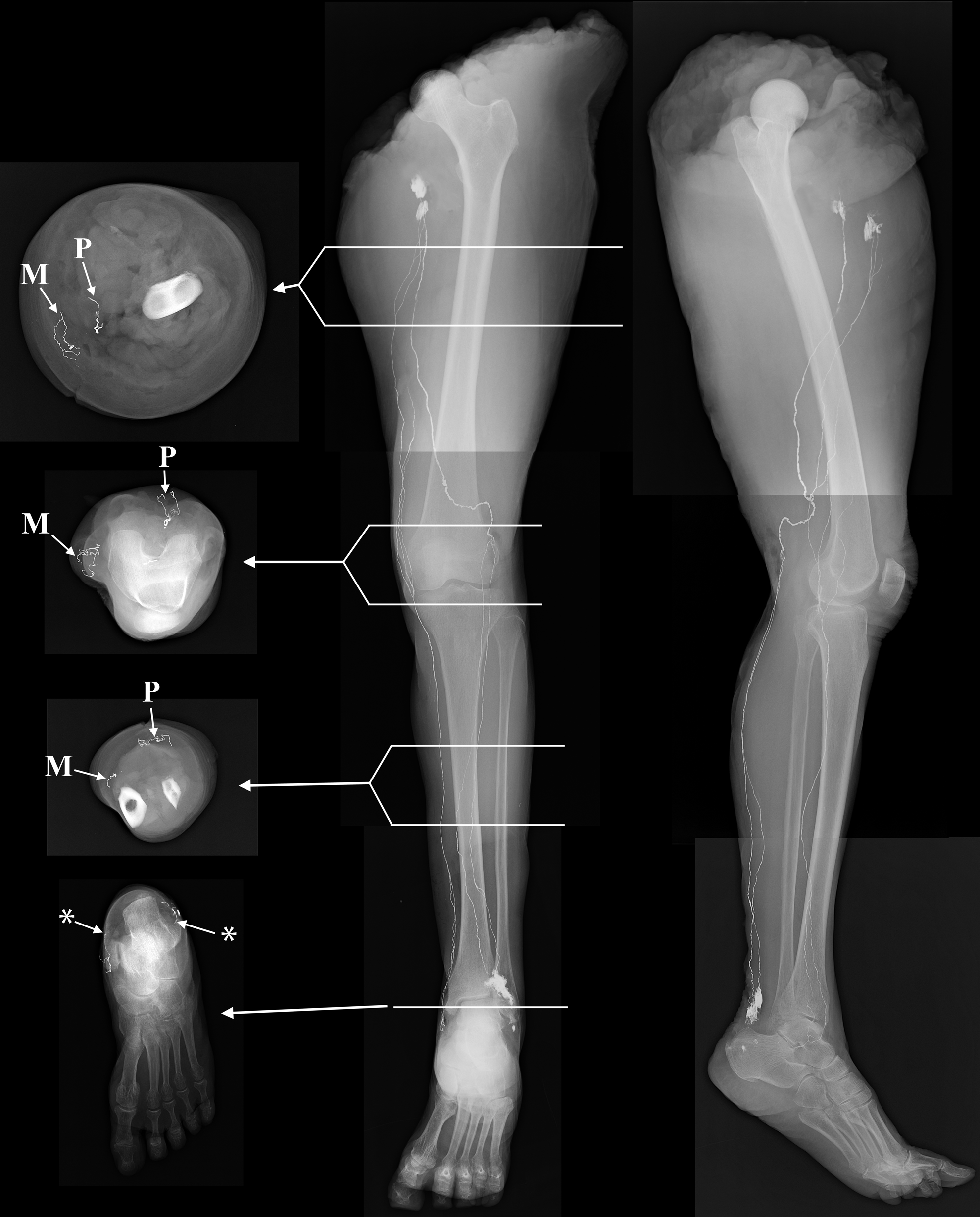
Radiographs after injection of barium sulfate mixture demonstrate lymphatics coursing from the heel to the inguinal region of the lower limbs. The left radiographs demonstrate cross sections through different levels within the leg. The central radiograph demonstrates an antero-posterior projection. The right radiograph demonstrates a lateral projection. P=postero-lateral group of lymphatics; A=antero-medial group of lymphatics; *=initial injection points.

Photograph after injection of barium sulfate mixture demonstrates the antero-medial group of lymphatics travelling with the GSV at the level of the knee.

Photograph after injection of barium sulfate mixture demonstrates the antero-medial group of lymphatics entering the superficial inguinal lymph nodes (LNs) next to the GSV in the inguinal region.
Lymphatic vessel diameters varied from 0.3 mm in the distal leg to 1.6 mm in the proximal thigh (Figs. 1 to 4). Transverse cross-sections demonstrated that lymphatic vessels belonging to the antero-medial group were situated in the subcutaneous tissue of the antero-medial aspect of the lower limb (Fig. 4).
Postero-medial group of lymphatic vessels
Lymphatics originated from the lateral injection point in the skin of the fossa situated between the lateral malleolus and the Achilles tendon. In four cases, these lymphatics formed two collecting vessels that travelled with the small saphenous vein (SSV) and its tributaries in the subcutaneous tissue of the postero-lateral aspect of the lower limb (Figs. 1, 2, 4, and 7). These collecting vessels then passed through the superficial and subsequently through the deep popliteal lymph node(s), situated within the popliteal fossa. In the thigh, they travelled with the superficial femoral neurovascular bundle to terminate in the medial group of deep inguinal lymph nodes (Figs. 1, 2, and 4). In two cases, two different lymphatic pathways were identified according to their origins:
(1) Lymphatic vessels arising adjacent to the SSV in the distal posterior aspect of the leg passed proximally to enter the popliteal lymph nodes. In one case, the efferent vessel of the deep popliteal lymph node then travelled through the thigh with the femoral neurovascular bundle to reach the deep inguinal lymph nodes (Fig. 3 left). In another case, the efferent vessel of the superficial popliteal lymph node passed obliquely through the subcutaneous tissue of the popliteal fossa to join with the antero-medial group of lymphatic vessels on the antero-medial side of the thigh (Fig. 8). (2) Lymphatic vessels arising from the posterior aspect of the lateral malleolus coursed in the subcutaneous tissue before dividing into two branches on the postero-lateral aspect of the leg. These lymphatics crossed over each other twice, first in the subcutaneous tissue of the distal third of the leg, and subsequently in the proximal third of the posterior aspect of the leg. In one case, these vessels then converged with the antero-medial group of lymphatic vessels (Fig. 8). In the other case, lymphatic vessels arising from the posterior aspect of the lateral malleolus coursed proximally in the subcutaneous tissue on the lateral side of the leg before forming two vessel groups at the knee. One group passed obliquely though the anterior aspect of the thigh to drain into the lateral group of inguinal lymph nodes; the other group passed obliquely through the posterior aspect of the thigh to drain into the medial group of inguinal lymph nodes (Fig. 3 left).

Photograph after injection of barium sulfate mixture demonstrates lymphatics running with the SSV and entering the superficial popliteal lymph node in the posterior aspect of the leg.
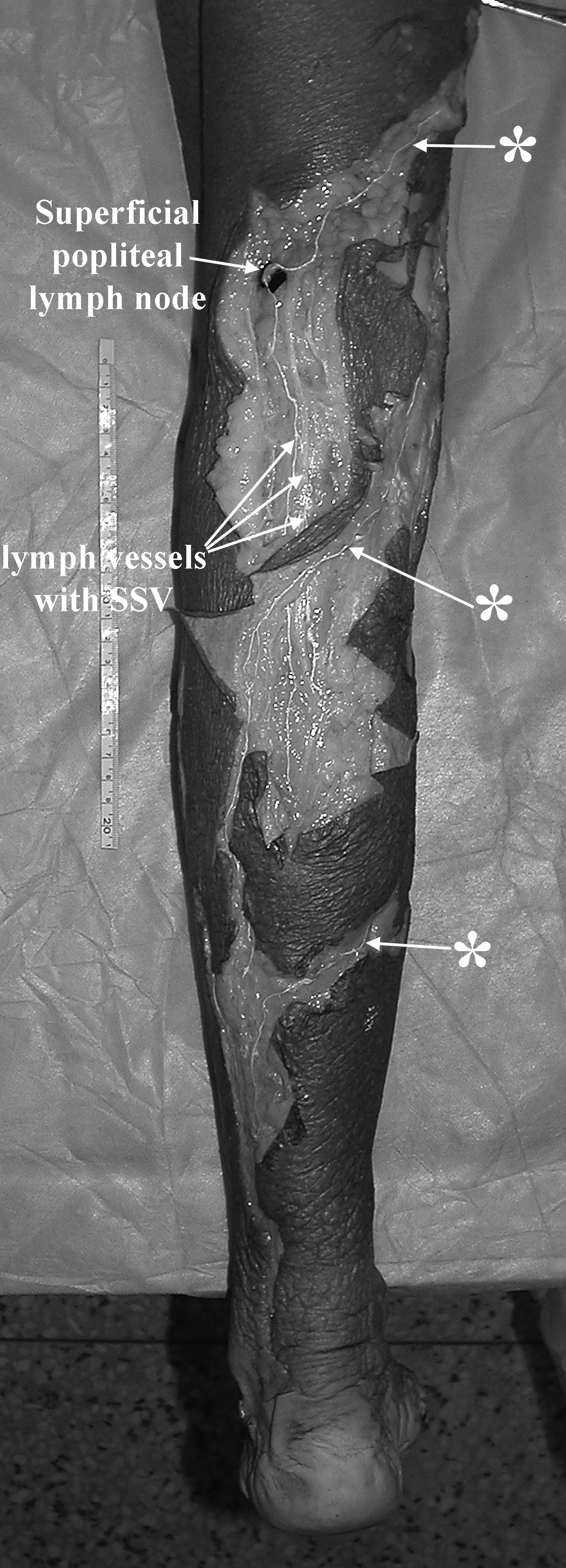
Photograph after injection of barium sulfate mixture demonstrates the distribution of the postero-lateral group of lymphatic vessels in the leg. *=vessels crossing the posterior aspect of the leg to merge with the antero-medial group of lymphatic vessels.
Lymphatic vessel diameters varied from 0.3 mm in the distal leg to 1.8 mm in the proximal thigh. Transverse cross-sections demonstrated that lymphatic vessels belonging to the postero-medial group were situated in the subcutaneous tissue of the lateral side of the foot, the postero-lateral aspect of the leg, the popliteal fossa and, if vessels were running with the superficial femoral neurovascular bundle, the medial intramuscular compartment of the thigh (Fig. 4).
Discussion
Historically, the lymphatic distribution of the lower limb has been described using mercury or dye injection techniques.3,4,6 Superficial lymphatic vessels were presented and described separately from the deep lymphatic vessels of the lower limb. Details of anatomical variation and inter-relationship of these vessels were not previously mentioned. Lymphangiographic investigation of the lower limb, using injection of radio-opaque contrast medium in vivo,7,14,15 has revealed some lymphatic anatomy. However, anatomical details were limited by the use of undissectable living subjects. Lymphoscintigraphy has also been utilized to identify sentinel lymph nodes for biopsy in the treatment of cancer patients.11,12 Three-dimensional and color-coded maps of the lower limb have been created to demonstrate lymphatic drainage patterns in patients with cutaneous melanoma. After analyzing lymphoscintigraphy data collected from more than 5000 patients, one patient with a melanoma situated on the right heel had results that demonstrated lymphatic drainage to the ipsilateral popliteal lymph nodes, ipsilateral groin, and contralateral groin. 12 Recent studies9,10 have shown details of the origin, number, size, presence/absence of valves, drainage patterns, and terminal lymph nodes of the superficial lymphatic vessels of the lower limb. Details of alternative lymphatic drainage routes from the popliteal fossa to the inguinal region have also been described. This study presented two major divergent lymphatic routes from the heel to the inguinal lymph nodes and indicated that: (1) the medial route was constant (Figs. 1 to 5), (2) two previously undescribed posterior routes were found in two cases (Figs. 3 and 8). These data, supplementing the results from previous studies,9,10 may explain some unexpected lymphoscintigraphy findings seen clinically.11–13
Lymphatico-venous anastomoses,16–20 lymphatic vessel grafting,21,22 and free flap tissue transfer using lymph nodes23,24 have all been performed to treat secondary lymphedema in the lower limb. Accurate anatomical understanding of the lymphatic routes9–15,25,26 involved may assist in the preoperative preparation and intraoperative management of these patients, thus affecting their postoperative outcome. It has been mentioned that as many anastomoses as possible should be performed in order to obtain the best clinical results. 27 This study provides a roadmap for surgeons when searching for potential lymphatico-venous anastomotic sites in the affected limb, or lymphatic grafting sites in the contralateral (healthy) limb, particularly where lymphatic vessels are situated close to veins such as the GSV and its branches in the medial aspect of the lower limb (Figs. 1 to 5), or the SSV in the postero-lateral leg (Figs. 1 to 4, 7, and 8). In summary, these results have provided additional information on the superficial lymphatic distribution of the lower limb to complement previous studies.
Conclusion
Detailed lymphatic routes from the heel to the inguinal lymph nodes have been described upgrading our anatomical knowledge. The results will be of benefit in the clinical management of lower limb lymphedema, trauma and malignancy.
Footnotes
Acknowledgments
Many thanks to Professor G. Ian Taylor in the Department of Reconstructive Plastic Surgery, Royal Melbourne Hospital, Australia, for his invaluable support.
Author Disclosure Statement
No competing financial interests exist.