
Abstract
Abstract
Background:
Lymphatic stomata are small lymphatic openings in the serosal membrane that communicate with the serosal cavity. Although these stomata have primarily been studied in experimental mammals, little is known concerning the presence and properties of lymphatic stomata in the adult human pleura. Thus, adult human pleurae were examined for the presence or absence of lymphatic stomata.
Methods and Results:
A total of 26 pulmonary ligaments (13 left and 13 right) were obtained from 15 adult human autopsy cases and examined using electron and light microscopy. The microscopic studies revealed the presence of apertures fringed with D2-40-positive, CD31-positive, and cytokeratin-negative endothelial cells directly communicating with submesothelial lymphatics in all of the pulmonary ligaments. The apertures' sizes and densities varied from case to case according to the serial tissue section. The medians of these aperture sizes ranged from 2.25 to 8.75 μm in the left pulmonary ligaments and from 2.50 to 12.50 μm in the right pulmonary ligaments. The densities of the apertures ranged from 2 to 9 per mm2 in the left pulmonary ligaments and from 2 to 18 per mm2 in the right pulmonary ligaments. However, no significant differences were found regarding the aperture size (p=0.359) and density (p=0.438) between the left and the right pulmonary ligaments.
Conclusions:
Our study revealed that apertures exhibit structural adequacy as lymphatic stomata on the surface of the pulmonary ligament, thereby providing evidence that lymphatic stomata are present in the adult human pleura.
Introduction
T
Lymphatic stomata are small openings that enable direct communication between the lymphatic lumen and the serosal cavity. 7 Since apertures in the diaphragmatic peritoneum were first described, 8 numerous investigators have confirmed the existence of lymphatic stomata not only in the peritoneum but also in the pleura of various types of mammals, such as rabbits, 9 rats,9–11 sheep,12,13 monkeys,14,15 golden hamsters, 16 and mice. 17 A large proportion of the liquid in the pleural cavity is presumed to exit by bulk flow not by diffusion or active transport. 5 Because erythrocytes within the pleural cavity are absorbed intact and in almost the same proportion as the liquid and protein, 18 Broaddus and Light predicted the existence of a major exit route via holes large enough to accommodate sheep erythrocytes (diameter, 6–8 μm), making the pleural stomata the only possible exit (diameter, 10–12 μm) into the pleural lymphatics. 5 However, these stomata have not been established in the adult human pleura. 19 Gaudio et al. studied visceral, mediastinal, diaphragmatic, and costal pleural samples obtained from 30 human adults, but they were unable to assess lymphatic stomata. 20 Peng et al. observed several gaps between mesothelial cells in two of eleven adult human parietal pleural samples; however, it is uncertain whether these gaps directly communicated with the submesothelial lymphatics in their study. 21 Liu et al. reported that the adult human pulmonary ligaments were characterized by the presence of stomata; 22 however, their study did not demonstrate lymphatic stomata properties. The lack of morphological evidence of lymphatic stomata prompted us to examine the adult human pleura.
The pulmonary ligament is a double-layered structure of pleura that connects the visceral pleura on the lower medial aspect of the lung to the parietal pleura on the mediastinum. The ligament extends downward in a sheet-like manner from the level of the lower pulmonary vein toward the diaphragmatic pleura, where it either is fixed or terminates in a free falciform border. 23 The aim of this study was to ascertain the presence of lymphatic stomata in the adult human pulmonary ligament.
Materials and Methods
Adult human autopsy cases encountered at Yokohama City University Hospital and Tokyo Medical University Hospital between 2004 and 2012 were examined in the present study. The criteria for inclusion in the study were as follows: 1) autopsy was conducted within 5 hours after death, and 2) pulmonary ligaments were grossly intact and free from adhesion. Twenty-six pulmonary ligaments (13 left and 13 right) were obtained from 15 Japanese cadavers (13 men and 2 women; mean age, 66.5 years) and were eligible for inclusion in the study. The clinicopathological features are summarized in Table 1. After gross examination, the pulmonary ligaments were gently excised without touching the surface; cut into small portions along a horizontal (short axis) direction; and fixed in 10%–20% neutral-buffered formalin for histological and immunohistochemical studies, 4% paraformaldehyde for enzyme histochemistry, and 2.5% glutaraldehyde in 0.1 mol/L cacodylate buffer for ultrastructural studies. The upper and middle regions of the pulmonary ligament were mainly used for enzyme histochemistry, whereas the lower region was mainly used for electron microscopic and immunohistochemical studies.
n/e=not evaluated because of pleural adhesion.
After fixation for 3 days at 4° Celsius, enzyme histochemistry was performed using 5′-nucleotidase to investigate the submesothelial lymphatics of the pulmonary ligament according to the method described previously. 24
Ultrastructural studies were performed as follows. After glutaraldehyde fixation, the samples were postfixed in cacodylate-buffered 2% osmium tetroxide for 2 h, dehydrated in ethanol, and subsequently dried using the t-butyl alcohol freeze-drying method. 11 The specimens were sputter-coated with gold and observed under a scanning electron microscope (S-4800; Hitachi; Tokyo, Japan). 11 Transmission electron microscopy was also conducted under a microscope (H-7500; Hitachi). 25
A light microscopic study was performed using serial 2-μm tissue sections obtained from formalin-fixed, paraffin-embedded tissue blocks; 50 serial sections per sample were used for hematoxylin and eosin staining and immunohistochemistry in series. Immunohistochemistry was performed using an autostainer (Histostainer, Nichirei, Tokyo, Japan), antibodies against cytokeratin CAM5.2 (CAM5.2, mouse IgG2a, Becton Dickinson, San Jose, CA, USA) as a marker for mesothelial cells, D2-40 (equal to podoplanin) (D2-40, mouse IgG1, Signet Laboratories, Dedham, MA, USA) as a marker for lymphatic endothelial cells and mesothelial cells and CD31 (JC/70A, Dako, Glostrup, Denmark) as a marker for lymphatic and blood vascular endothelial cells, and a detection kit (Histofine Simple Stain MAX PO, MULTI, Nichirei) according to the manufacturers' instructions. The alveolar epithelium and the lymphatic and blood vascular endothelia of the lung were used as positive controls for the immunohistochemistry. For negative controls, the primary antibodies were omitted during the staining procedure.
Indirect immunofluorescence was performed using a double-staining method for CAM5.2 with Alexa Fluor 488-conjugated goat anti-mouse IgG2a antibody (Invitrogen, Carlsbad, CA, USA), and D2-40 with Alexa Fluor 555-conjugated goat anti-mouse IgG1 antibody (Invitrogen) as well as 4′,6-diamidino-2-phenylindole (DAPI) (Roche Diagnostics, Mannheim, Germany). 26 To observe the immunofluorescent images, a fluorescence microscope (BX51, Olympus, Tokyo, Japan) was employed.
Three-dimensional histological image reconstruction was performed using serial tissue sections stained with CAM5.2 and D2-40 antibodies, a virtual slide scanner system (Nanozoomer 2.0RS, Hamamatsu Photonics, Hamamatsu, Japan), and TRI/3D-SRF2 software (Ratoc System Engineering, Tokyo, Japan). 27
From the serial tissue sections, the sizes and frequencies of the apertures fringed with endothelial cells and directly connected to the pleural cavity with submesothelial lymphatics were measured over approximately 1-mm2 regions of serosa. The sizes and frequencies of apertures between the right and left pulmonary ligaments were compared using a paired Wilcoxon rank sum test with SPSS 18.0 (SPSS, Chicago, IL, USA).
Results
Enzyme histochemistry with 5′-nucleotidase revealed a rich submesothelial lymphatic network in the pulmonary ligament (Fig. 1). Lattice-like lymphatic networks were visible with numerous blind-ended initial lymphatics and irregularly dilated lymphatics. The fractions (area densities) of these superficial lymphatics were approximately 25%–35%. The dimensions of these superficial lymphatics varied greatly (1–420 μm). Ill-defined valve-like structures were observed in these superficial lymphatics. The dimensions of the initial lymphatics ranged from approximately 1 to 4 μm.

Scanning electron microscopy revealed primarily three types of serosal membranes in the pulmonary ligament: 1) flattened with scarce microvilli; 2) intermediate; and 3) cuboidal and microvilli-rich mesothelial cells (Fig. 2). The membranes composed of cuboidal and microvilli-rich mesothelial cells tended to accompany several apertures between them. However, the shapes and sizes of these apertures were diverse. Some apertures were circular, whereas others were irregular; some were small or narrow, such as clefts, whereas others were large enough for a cell to pass through. Gullies on the pleural surface were often too deep and dark to determine whether these apertures continued to the submesothelial lymphatic lumen. Measuring the precise size of the apertures was difficult due to their irregular shapes.

Scanning electron micrographs of the surface side of the pulmonary ligament.
Transmission electron microscopy revealed the presence of apertures in the serosal membranes that directly communicate with submesothelial lymphatic capillaries (Fig. 3). The orifices of these apertures were fringed with cytoplasmic elongation of submesothelial lymphatic endothelial cells. The sizes of these apertures were diverse; several apertures were small with overlapping endothelial cells, whereas others were large enough for a cell to pass through and did not exhibit overlapping endothelial cells.
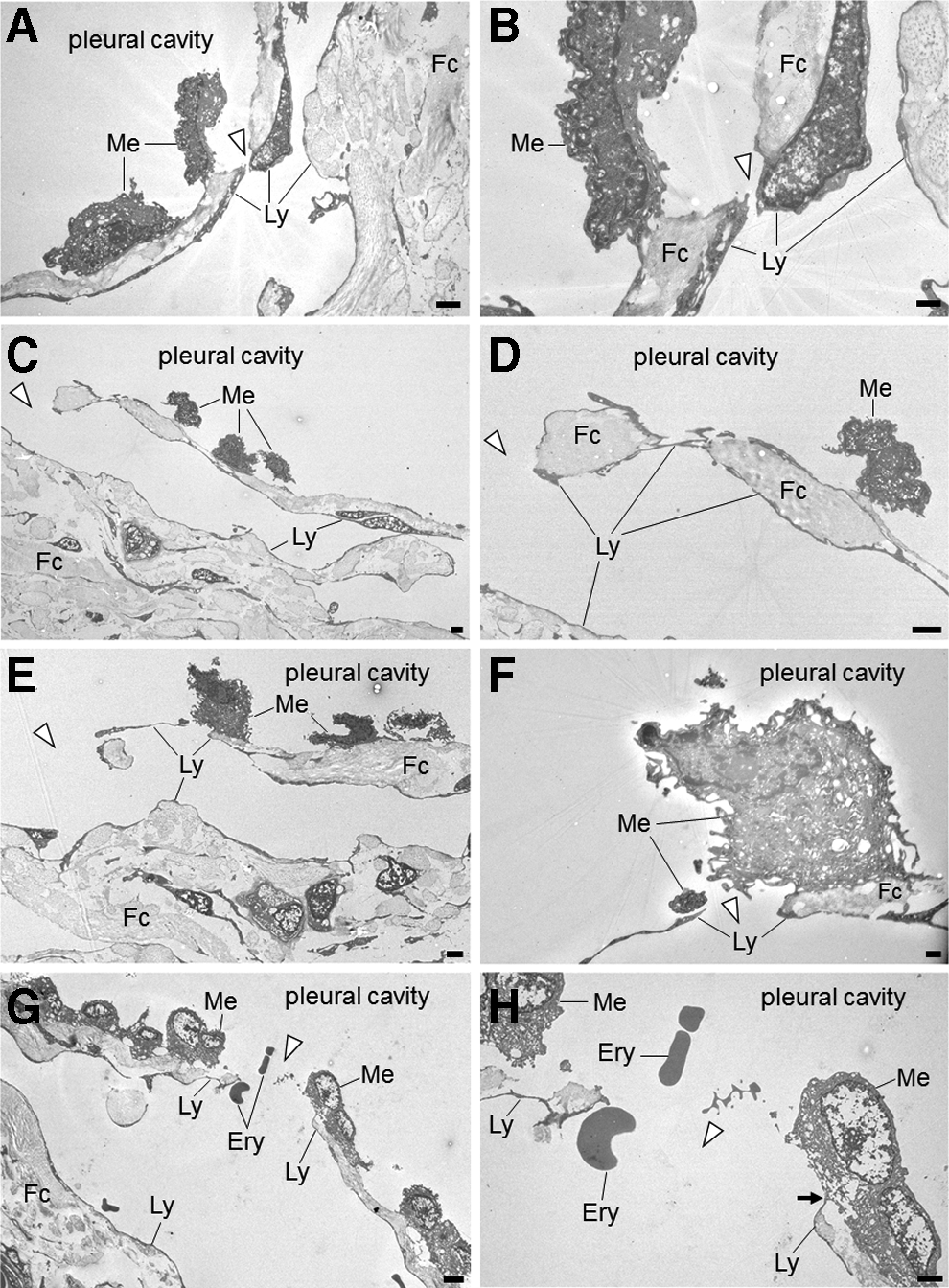
Transmission electron micrographs of the pulmonary ligament. Panels on the right side are enlargements of details presented in the panels on the left.
Our histological study revealed that the surface of the pulmonary ligament was covered by a monolayer of mesothelial cells (Fig. 4). In the immunohistochemical studies, the positive and negative controls yielded the appropriate reactions. The mesothelial cells were immunohistochemically positive for CAM5.2 (Fig. 4D) and D2-40 (Fig. 4E) and negative for CD31. Beneath the mesothelial layer, we observed an abundance of cistern-related dilated lymphatic capillaries. The endothelial cells of these lymphatic capillaries were immunohistochemically positive for D2-40 (Fig. 4E) and CD31 (Fig. 4F) and negative for CAM5.2 (Fig. 4D). Between the mesothelial layer and the submesothelial lymphatic capillaries, we observed a thin fibrous connective tissue that was discontinuous and formed apertures that communicated directly with the pleural cavity. These apertures were fringed with D2-40-positive, CD31-positive, and CAM5.2-negative lymphatic endothelial cells (Fig. 4). An immunofluorescent multiple staining method highlighted these structures (Fig. 5). Three-dimensional histological image reconstruction of the pulmonary ligament indicated the proximity of the lymphatics to the mesothelial layer and submesothelial-rich lymphatics that were irregularly dilated, cistern-related or anastomotic (Fig. 6).

Light micrographs of serial sections of the pulmonary ligament. The submesothelial layer consists of fibrous connective tissue, which is occasionally discontinuous due to interruptions by stomata. The stomata are lined with low-molecular weight cytokeratin CAM5.2(-), D2-40(+), and CD31(+) lymphatic endothelial cells (

Low-power photomicrographs of immunofluorescent multiple staining performed on the pulmonary ligament (fluorescence microscope). This tissue section is one of the serial sections following Figure 4C.
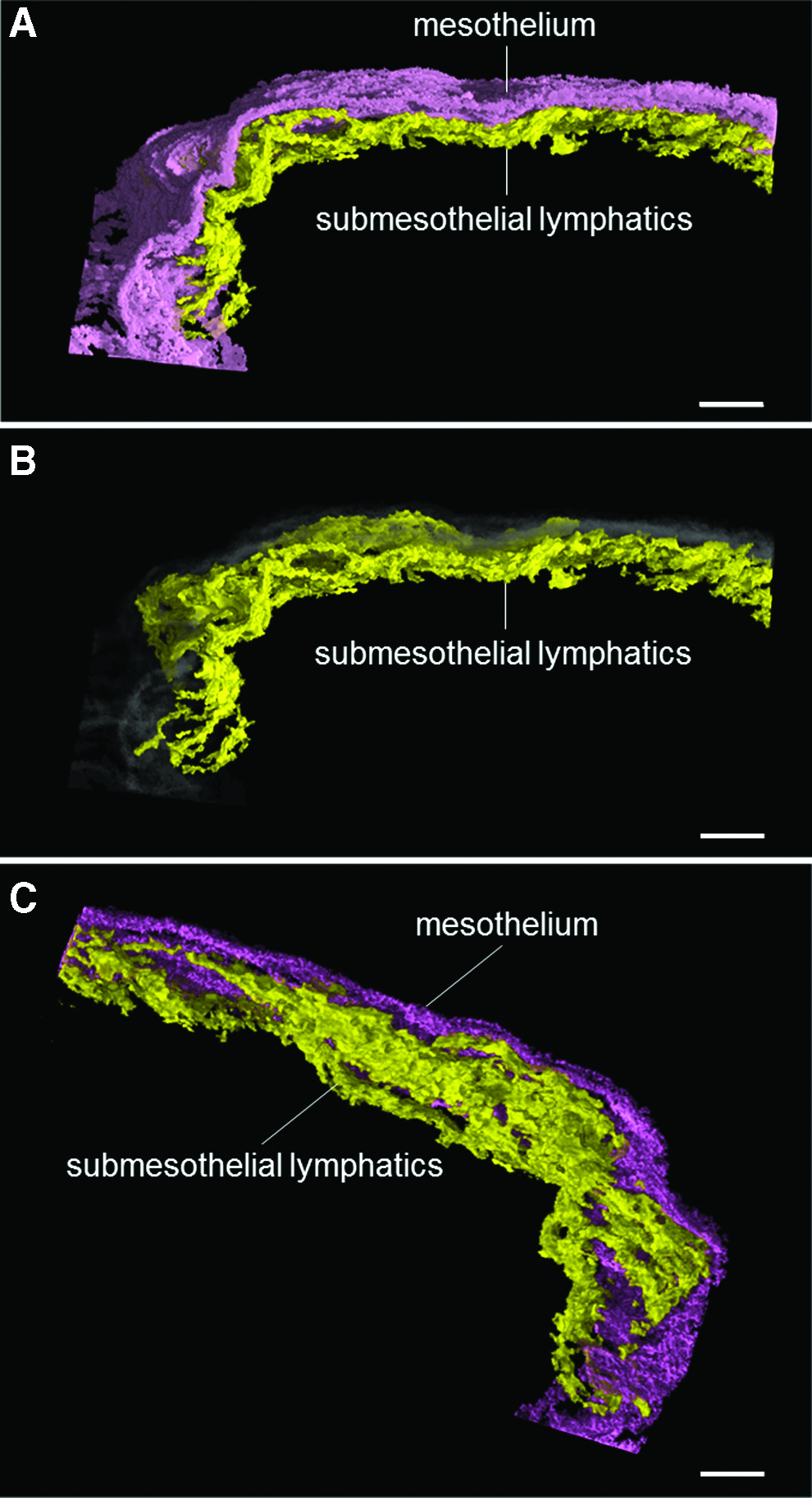
Three-dimensional histological image reconstruction of the mesothelium and lymphatics in the pulmonary ligament. The violet color denotes mesothelial cells, the yellow color denotes lymphatic endothelial cells, and the gray color indicates the transparent image of mesothelial cells.
The sizes and densities of these apertures varied from case to case (Table 2). The median aperture sizes ranged from 2.25 to 8.75 μm in the left pulmonary ligaments and from 2.50 to 12.50 μm in the right pulmonary ligaments. The aperture densities ranged from 2 to 9 per mm2 in the left pulmonary ligaments and from 2 to 18 per mm2 in the right pulmonary ligaments. However, no significant differences were found in the sizes (n=11, p=0.359) or densities (n=11, p=0.438) of the apertures between the left and right pulmonary ligaments.
n/e=not evaluated because of pleural adhesion. (n)=frequency of apertures observed per 1 mm2.
Discussion
In the present study, the apertures exhibited structural adequacy as lymphatic stomata on the surface of the pulmonary ligament in adult humans, thereby providing evidence of lymphatic stomata in the adult human pleura.
In the serosal membrane, the term stomata has historically been used to describe the following three microstructures: 1) gaps formed in the submesothelial connective tissue that do not directly communicate with submesothelial lymphatics but may constitute a pre-lymphatic fluid pathway, which is often referred to as macula cribriformis;28,29 2) apertures in which the lymphatic endothelial cells are exposed to the serosal cavity without patency but are accompanied with a flap valve-related intercellular overlapping of endothelial cells, which is occasionally referred to as closed lymphatic stomata;30,31 and 3) apertures fringed with lymphatic endothelial cells that enable direct communication between the lymphatic lumen and the serosal cavity, 32 which is occasionally referred to as open lymphatic stomata. The structural and immunohistochemical properties of the apertures observed in the present study were consistent with those of open lymphatic stomata.
In various types of mammalian pleural cavities, lymphatic stomata are exclusively observed in the parietal pleura and are considered to be a major route for pleural fluid resorption and the egress of cells or foreign particles.33,34 Pleural effusion occurs when the entry rate of liquid increases, the exit rate of liquid decreases, or a combination of both. 5 Given that lymphatics in the parietal pleura have a large capacity with respect to the exit rate (0.28 mL/kg/h, which is nearly 30 times the baseline rate of 0.01 mL/kg/h), a situation in which only the entry rate increased would require a sustained rate of greater than 30 times the normal rate to exceed the reserve lymphatic drainage capacity. However, if the exit rate exclusively decreased, it would require more than a month at the normal entry rate of 12 ml/day to produce an effusion detectable by chest radiograph. 5 It is also important to note that a portion of foreign particles inhaled and deposited into the lung is thought to reach the pleura, pass through the pleural space, and exit via the stomata. 35 Interestingly, long fibers and long carbon nanotubes, such as asbestos fibers, cannot negotiate the stomata and are retained, thus initiating inflammation and pleural pathology. 36 Therefore, lymphatic stomata are considered to be directly or indirectly involved in certain pleural diseases.
The physiological mechanism of intrapleural drainage via lymphatic stomata has not been established. In general, lymphatics are thought to have two types of valve systems: a flap valve system and an outlet valve system.37,38 The former consists of overlapping of adjacent lymphatic endothelial cells with a loose, button-like junction at the initial lymphatics that allows fluid to enter from the interstitium into the lymphatics but prevents reflux. 37 The latter consists of plicae of the lymphatic inner wall that are typically preset as a set of two semilunar, pocket-like structures facing each other in the lymphatic lumen. 38 This outlet valve prevents reflux between adjacent lymphangions and enables unidirectional lymph flow in collaboration with a pumping action of the lymphatic vessels. 38
Of particular note is that the lymphatic vessels effectively adapt their contractile force to the particular hydrodynamic conditions according to different anatomical regions. 39 With regard to the pleural cavity, the intrapleural pressure and surface area of the pleura vary dynamically depending on a number of factors, such as breathing patterns and physical exertion. For example, the mean cephalocaudal distances during motion of the central portion of the diaphragm where the lower portion of the pulmonary ligament is attached are approximately 20.6 mm during spontaneous breathing and 64.2 mm during maximal deep breathing in healthy younger adults. 40 Several investigators have speculated that back-flow from the lymphatic stomata into the serosal cavity is prevented by minute overlapping of mesothelial and endothelial cells according to serosal membrane movement that is synchronously coordinated during breathing;41–43 whether this cellular overlapping in the lymphatic stomata can efficiently prevent regurgitation against these dynamic changes remains to be determined. Because not all of the stomata we observed were equipped with flap valve-related cytoplasmic processes, some of the flow via the stomata is potentially bidirectional.
Although the role of the pulmonary ligament remains to be completely elucidated, it does play a significant role in influencing the presentation and configuration of many events that affect the lower lobe, the adjacent pleural space, and the mediastinum. 23 Some of the lymph from the lower lobe of the lung flows into the pulmonary ligament; 44 a lymph node chain is present in the pulmonary ligaments of the lung where the lymph nodes correspond to station 9. 45 The lymphatic vessels of the pulmonary ligament drain toward the tracheal bifurcation, the thoracic duct, or the intra-abdominal lymph nodes in the celiac region. 45 Interestingly, these lymph flows can travel bi-directionally even under normal conditions.46–51 In addition, cancer metastasis to the pulmonary ligament has a potential role in the pathogenesis of pleural carcinomatosis. 22 The functional roles of the pulmonary ligament must be explored from the perspective of the lymphatic stomata.
In conclusion, our study has confirmed the presence of lymphatic stomata in the adult human pleura. Understanding the properties of these structures under normal and abnormal conditions will help to elucidate several mechanisms of human pleural diseases.
Footnotes
Acknowledgments
We thank the following individuals at Tokyo Medical University for sharing their expertise on human anatomical pathology: Motoshige Kudo, MD, PhD; Reisuke Takahashi, MD, PhD; Isao Yoshihama, PhD; and the late Yoshiro Ebihara, MD, PhD. We also thank Michiyo Kanazawa, LT; Yukiko Nishio, LT; Hiroyuki Machida, MD, PhD; Hajime Kitamura, MD, PhD; Shoji Yamanaka, MD, PhD; Yoshiaki Inayama, MD, PhD; and the late Kiyoshi Gomi, MD, PhD at Yokohama City University for providing technical advice. Finally, we thank Edward F. Barroga, DVM, PhD, and J. Patrick Barron, Professor Emeritus at Tokyo Medical University for reviewing our manuscript, as well as Tatsuo Shimada, MD, PhD, at Matrix Medicine, Faculty of Medicine, Oita University for providing constructive criticism.
Author Disclosure Statement
No competing financial interest exists. This research was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan (No. 20790993 and No. 24590242 to H.O.), Exploratory Research from the Yokohama Foundation for Advancement of Medical Science (to H.O.), and Medical Research from the Tokyo Medical University Cancer Center (to H.O.).